Parkinson’s: A Perplexing Puzzle for Researchers
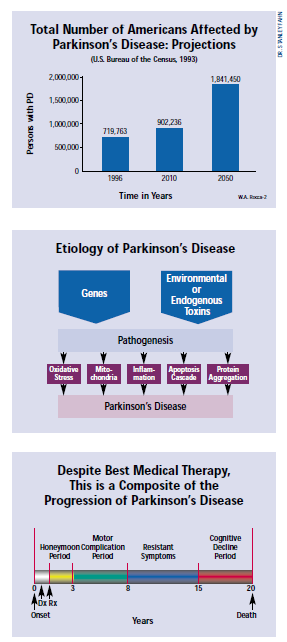
Nearly two centuries after James Parkinson first defined “shaking palsy” in 1817, million of people throughout the world struggle daily with the disabling effects of Parkinson’s Disease. Neither a cause nor a cure has yet been found for this enigmatic and deadly disease.
Published November 1, 2002
By Vida Foubister

Speaking as chair of the opening session at a recent three-day seminar on Parkinson’s Disease, sponsored by The New York Academy of Sciences (the Academy), Stanley Fahn, MD, director of the Center for Parkinson’s Disease and Other Movement Disorders at Columbia University, wasted no time in summing up the dilemma.
Many decades ago, he told the large gathering of scientists and clinicians – whose registry resembled a global “who’s who” in PD research – “two basic science findings in clinical, pathological and animal models led to the dopamine hypothesis of Parkinson’s disease. And we’ve been there ever since.”
Dopamine, produced by the dopaminergic neurons in the substantia nigra region of the brain, was found to reverse bradykinesia in animals. Bradykinesia, which includes difficulty initiating movement, slowness in movement and paucity or incompleteness of movement, is considered the most prominent and disabling symptom of PD. The second finding was that PD patient brains were markedly depleted in dopamine and the amount of depletion correlated with the disease’s severity.
Since the 1960s, the early features of the disease have been treated with levodopa (L-dopa) and similar drugs that function by replacing the lost dopamine. “Before my drug takes effect, I am unable to move well enough to really get out of bed,” explains Joan I. Samuelson, president of the Parkinson’s Action Network. “Then, an hour later, I can get up, get dressed and walk into the room and function. That’s miraculous.”
Treating Symptoms, Not PD
The fact that this drug exists, and that PD was the first neurological disease to be treated with pharmacological drugs, isn’t trivialized. However, there is a growing sense that the field is ripe to move beyond this early discovery and symptomatic treatment.
L-dopa and other related drugs often cause significant side effects, most notably dyskinesias – or involuntary movements – that limit their usefulness. And even though many patients initially respond well to therapeutics, they lose their effectiveness as the disease progresses. Most importantly, these drugs only function to treat the symptoms of Parkinson’s and do nothing to slow the disease process.
Patients, clinicians and scientists spent three days in September, essentially sequestered at a wooded retreat near Princeton, N.J., discussing where the field should go. As the organizers hoped, the setting of this conference, Parkinson’s Disease: The Life Cycle of the Dopamine Neuron, brought people together across many disciplines and stimulated discussions that continued from early morning sessions into impromptu evening debates.
The high level of interaction at the conference stimulated both new ideas for research and treatment, as well as connections between the existing body of scientific and clinical knowledge. Yet it also highlighted the dichotomy that exists in the field. Despite all that is known about Parkinson’s, its cause remains essentially unknown and untreatable.
That dichotomy was reflected by the participants. Some pushed for more basic research, including investigation into the non-motor aspects of the disease that are often overlooked due to the focus on the role of dopamine neurons. However, others urged the scientists to move their many promising new findings out of the lab and into the clinic.
Important Leads

John Q. Trojanowski, MD, PhD, co-director of the Center for Neurodegenerative Disease Research at the University of Pennsylvania School of Medicine, is among those who believe there are a “number of phenomenally important leads that have potential implications for therapies.” He pointed to new findings about some of the proteins that have been implicated in PD, namely alpha-synuclein and parkin. “Knowing the culprits, the molecular criminals, is the first step towards taking them out of the action or doing something to improve what’s broken,” Trojanowski said.
Lewy bodies, a pathological marker of Parkinson’s disease in the substantia nigra, contain a fibrillar form of alpha-synuclein. Though it’s long been known that patients with the familial form of the disease can have a mutation in the gene coding for this protein, new data presented at the conference suggests that alpha-synuclein abnormalities in patients with sporadic Parkinson’s might be due to mitochondrial dysfunction. (Sporadic Parkinson’s is more common than the familial form of the disease.)
“We know from a genetic standpoint that alpha-synuclein does what it does because you have a mutation, but why in everybody else does synuclein go bad?” asked Ted M. Dawson, MD, PhD, director of the Morris K. Udall Parkinson’s Disease Research Center of Excellence at the Johns Hopkins University School of Medicine. “Well, it might be because oxidative stress is hammering it.”
Some New Clues
Peter T. Lansbury Jr., PhD, an associate professor of neurology at Harvard Medical School, presented some new clues about what in the alpha-synuclein fibrillization process causes disease. His research suggests that an intermediate, called a protofibril, is toxic to dopamine neurons and he has also found that the formation of this protofibril can be inhibited by beta-synuclein.
“Beta-synuclein has a nice therapeutic profile: It stops oligomerization all together,” Lansbury said. “We are proceeding with this idea as a therapeutic strategy. Specifically, we’re interested in developing small molecules that would induce increased expression of endogenous beta-synuclein.”
Mutations in parkin, another so-called molecular criminal, are the most common cause of familial PD. It’s been found to function as a unbiquitin E3 ligase that labels proteins for degradation and disposal. That means when parkin isn’t functioning, proteins such as synphilin-1 and Pael receptor build up in the cell. “The current theory is that the accumulation of these substrates causes Parkinson’s disease,” Dawson said. “So enhancing the function of parkin, identifying the substrates and then figuring out ways to get them degraded” are possible therapeutic approaches.
The Cellular Level
Moving from proteins to the cellular level, another session at the conference focused on the mitochondria and the circumstances under which it produces toxic oxygen-free radicals that lead to apoptosis or cell death.
“There’s more and more reason to believe that in Parkinson’s disease, either because of environmental toxins like pesticides or because of genetic defects, the mitochondria produce an abnormally high level of these reactive oxygen species,” said Gary Fiskum, PhD, professor and research director in the department of anesthesiology at the University of Maryland School of Medicine.
One way to elucidate this pathogenic mechanism is by using genomics and proteomics to identify genes that are expressed in response to environmental toxins and mitochondrial oxidative stress. “The idea is that you may come up with things you have no preconceived notion would be associated with the disease process and that, conceivably, might give you a new insight into the disease,” explained M. Flint Beal, MD, neurologist-in-chief at The New York Presbyterian Hospital.
Beal’s research has focused on two known antioxidants – coenzyme Q10 and creatine – that act either to inhibit the production of mitochondrial free radicals or to detoxify them once they’re produced. “We have good animal data that [coenzyme Q10 and creatine] prevent damage to dopaminergic neurons,” he said. “What we’re going to do now is see if we can administer those in combination with some anti-inflammatory drugs and get even better protection.”
New Approaches
Much excitement has been generated in the field by the promise of two approaches to replace the dopamine neurons that are lost in patients with Parkinson’s disease. One involves manipulating endogenous precursor cells in the adult brain to become dopamine neurons. The other approach focuses on transplanting embryonic stem cells, which have been coaxed to become dopamine neurons, into the adult brain.
“There’s evidence that even a mature and degenerating brain will accept new cells, including neurons, that will grow to reconnect damaged parts,” said Ole Isacson, Dr. Med. Sci., M.B., director of The Morris K. Udall Parkinson’s Disease Research Center of Excellence at Harvard University Medical School.
The implications of these therapies for patients, though not novel, can be dramatic. Such was the film clip presented by Isacson that showed a patient with advanced Parkinson’s disease walk down a hallway before and after receiving a transplantation of fetal dopamine cells. The first walk down the hall seemed to take forever, as the patient struggled with every step. Then, after the transplant, the patient appeared to stride down the hall and back.
Though this demonstrates the potential of this strategy, Ronald McKay, PhD, senior investigator at the National Institute of Neurological Disorders and Stroke, doesn’t believe it represents a possible therapy for patients. “It’s just too difficult,” he said. Among the problems he cited is the challenge of obtaining a sufficient number of fetal cells for the procedure.
The Promise of Embryonic Stem Cells
Instead, McKay emphasized the promise of embryonic stem cells that have been engineered to become dopamine neurons – both for cell therapy and for further study of the disease. Those studies include determining what signals and factors are required to make an immature cell become a dopamine neuron. “The title of this meeting is the life cycle of the dopamine neuron. We’re essentially dissecting the life cycle of the neuron,” he said. “There’s many signals at different stages that influence the properties of the cells.”
Manipulating precursor cells in the brain to become dopamine neurons might have some advantages due to their existing regional differentiation. “Rather than one tube of all-purpose cells, one potentially can recruit precursors that would give rise to the right kind of replacement neurons,” commented Jeffrey D. Macklis, MD, D.HST, associate professor of Neurology and Neuroscience at Harvard Medical School.
Overall, the basic scientific understanding of Parkinson’s disease appeared to reach a new level at the conference, generating hope that the focus of the next such meeting will be on clinical therapies. “This kind of session tells you how complicated [the disease] is, but any day now there could be a revolutionary big idea,” Samuelson said. “If it’s in the treatment end of things, it could revolutionize the lives of a million people pretty quickly, and that’s a big deal.”
Also read: The Role of Glial Cells in Alzheimer’s, Parkinson’s