Adrienne Hollis, PhD, JD, the Senior Climate Justice and Health Scientist at the Union of Concerned Scientists, explains the role scientists must play in mitigating the harm caused by plastic waste and pollution from polymer production.
Published March 4, 2021
By Stephen D. Albright, PhD
Sunset over petrochemical plants in Lake Charles, Louisiana. (David Wilson from Oak Park, Illinois, USA, CC BY 2.0, via Wikimedia Commons)
New scientific discoveries often have profound impacts beyond what researchers can initially imagine. Polymers, and plastics derived from them, are an instructive example: the plastics that were once heralded as cheap, durable, and functional have also created an environmental crisis. Plastic waste and pollution from polymer production are significant hazards for communities around the world.
Adrienne Hollis, PhD, JD, the Senior Climate Justice and Health Scientist at the Union of Concerned Scientists (UCS), recently answered some questions about the impact of plastics and the role scientists have in mitigating their harms. Before joining UCS, Dr. Hollis served as a section chief at the Agency for Toxic Substances and Disease Registry, an agency within United States Department of Health and Human Services, and as an Associate Professor at the Florida A&M University Institute of Public Health.
How would you define environmental justice and why should basic science researchers care about it?
Hollis: To me, basic science research focuses on gaining a fundamental understanding of the natural environment and how natural resources are transformed. Environmental justice talks about the adverse effects on communities from exposure to the unnatural transformation of the natural environment, through actions like air or water pollution. A specific focus of environmental justice is the disproportionate impact of exposure on disadvantaged areas and communities of color. But I would defer to communities and community organizations for their definition. That is what matters.
Outside of moral and ethical considerations of fairness, researchers are urged to follow the Precautionary Principle, based on the concept of “Do No Harm” in the medical profession. It states that if anything has a suspected risk of harm, to either the public or the environment, scientists should immediately engage in actions to prevent harm, even in the absence of complete scientific data identifying risk. These actions are at the core of environmental justice, and should apply across all areas of basic science research.
One of the most striking examples of communities of color and/or low socioeconomic status being disproportionally affected by environmental hazards is a stretch of Louisiana along the Mississippi River. Called by many “Cancer Alley,” it is home to a high density of oil refineries and petrochemical plants, key steps of polymer and plastic production. What have been some of the hazards and illnesses documented in this region?
Hollis: I would first state that community members would be the best source of information on health effects because of their historic knowledge and community data on this issue. What I can say is that high rates of many health conditions—miscarriages, cancer, heart problems, respiratory problems like asthma and chronic obstructive pulmonary disease (COPD), and others—are present and well-documented in this region.
A perfect example of a hazard is the 2020 fire at a Lake Charles, Louisiana chlorine plant after Hurricane Laura. During and after the fire, residents were ordered to shelter in place, close all windows, and not operate air conditioners to prevent chlorine exposure. Amidst a pandemic and summer heat, the situation could have been so much more devastating—widespread COVID-19, heat stroke, or chlorine poisoning were all real possibilities. And yet, facilities keep coming!
Nick Fewings, via Unsplash
Researchers in polymer chemistry are working towards developing polymers and plastics that can be more sustainably produced and disposed of. What kinds of changes to a polymer’s life cycle would be most impactful for communities hit hardest by industrial pollution?
Hollis: People living in places like Cancer Alley deal with facilities that release traditional air pollution as well as greenhouse gases while making plastics. Changes that would be impactful include ceasing the extraction of fossil fuels for polymer production and changing the plastic production processes that generate pollutants like ethylene oxide, styrene, and benzene. Processes that exclude the use of these chemicals would be optimal.
But the most impactful step would be to get rid of those facilities. Hopefully, as new processes are developed to improve plastic recycling and reuse, there will be decreased demand for facilities that produce virgin plastics. In the meantime, research and development of alternatives to biopolymers and petroleum-based products—both of which lead to adverse health effects—would also be a great intermediate step.
What actions could scientists and engineers take during the research process to mitigate and prevent adverse impacts when their research translates into products? What should research practices that incorporate environmental justice look like?
Hollis: In my opinion, it is not really about making production better and safer. It is about the Precautionary Principle, which all scientists should adhere to: do no harm. This means taking preventive action when you suspect harm could occur and most importantly, increasing public participation in decision making. Scientists and engineers must, at the outset, identify the communities that may be impacted, work with those communities early and often to identify concerns, and move forward together. Scientists and engineers must ask themselves if they would want to live in a place that produces these products, and whether the processes they are developing to mitigate and prevent harm are good enough for them or their families.
By definition, a rare disease is one that afflicts relatively few people compared to the general population. Collectively, though, there are over 7,000 of these conditions known, causing immense suffering for an estimated 300 million patients. Because most rare diseases stem from specific genetic mutations, they’ve proven difficult to treat.
Genome sequencing and molecular medicine might soon change those grim statistics, though. For example, using short DNA or RNA sequences complementary to the messenger RNA for a gene, researchers can inhibit the expression of the associated protein. These complementary sequences—called antisense oligonucleotides—could soon be delivered as drugs to treat many rare diseases.
On October 2, 2020, The New York Academy of Sciences and Takeda Pharmaceuticals hosted the Frontiers in Rare Diseases: 2020 Innovators in Science Award Symposium, an event highlighting breakthroughs in rare diseases research and honoring 2020 Innovators in Science Award Winners Adrian Krainer, PhD and Jeong Ho Lee, MD, PhD. Presentations, a panel discussion, and a virtual poster session covered the basic science, recent clinical breakthroughs, and remaining challenges in this rapidly evolving field.
Symposium Highlights
While many rare diseases are inherited, others arise through mutations in somatic cells during life.
Antisense oligonucleotides can alter the expression of specific genes, potentially mitigating or reversing many genetic diseases.
Clinical trials for rare disease therapies must be tailored to the pathogenesis of each disease.
Redirecting neural stem cells to become neurons could treat many neurodegenerative diseases.
The COVID-19 pandemic is inspiring new collaborations that could be adapted to rare disease research.
Speakers
Jeong Ho Lee, MD, PhD Korea Advanced Institute of Science and Technology
Adrian Krainer, PhD Cold Spring Harbor Laboratory
Annemieke Aartsma-Rus, PhD Leiden University Medical Center
Don Cleveland, MD, PhD University of California, San Diego
Huda Zoghbi, MD Jan and Dan Duncan Neurological Research Institute, Texas Children’s Hospital
Brad Margus Cerevance
Graciana Diez-Roux, PhD Telethon Institute of Genetics and Medicine
David Fajgenbaum, MD University of Pennsylvania
Anne Heatherington, PhD Takeda Pharmaceuticals
Sponsors
The Winner’s Circle
Speakers
Jeong Ho Lee, MD, PhD Korea Advanced Institute of Science and Technology
Adrian Krainer, PhD Cold Spring Harbor Laboratory
Not Born This Way
Jeong Ho Lee, Early-Career Scientist winner of the 2020 Innovators in Science Award, discussed his work studying how somatic cell mutations—mutations that occur after development, during the normal process of cell division—result in rare neurological diseases caused by somatic cell mutations in the brain. Much of the recent boom in work on genetic diseases has focused on germline mutations. Because these mutations occur early in embryonic development, they show up in many types of cells throughout the body and are passed on to future offspring. These rare germline mutations can often be identified by sequencing the genomes of cells in easily accessible tissues, such as blood or skin. With advances in next-generation sequencing, “it’s become much easier to identify the germline mutations coding for many rare neurological disorders,” said Lee.
Somatic cell mutations occur throughout life, in every part of the body.
Nonetheless, germline mutations account for only a minority of rare neurological disorders. For example, 98% of epilepsy cases cannot be explained by germline mutations.
“We hypothesized that somatic cell mutations may be responsible for these unexplained neurological [diseases],” said Lee.
Somatic cell mutations occur during the ordinary cell division process that takes place billions of times in developing embryos, and continues to occur throughout life as somatic, or non-gamete, cells turn over.
DNA replication isn’t perfect, and human cells average 0.1 to 3 mutations per genome every time they divide. Lee theorized that a patient who hadn’t inherited an epilepsy-causing germline mutation might instead acquire somatic cell mutations in a subset of brain cells during development or later in life. If that happened, the mutation would only show up in the affected area of the brain, not in any other cells of the body.
One treatment for certain types of epilepsy is to resect the portion of the brain causing the seizures. Lee and his colleagues took samples of the brain tissue resected in these operations, along with blood samples from the same patients, and performed deep DNA sequencing to identify somatic mutations that occurred only in the affected brain tissue, not in the blood. They identified such mutations, including ones unique to genes involved in motor nerve activity, in 30% of the patients. When the scientists introduced the same mutations into a small percentage of neurons in developing mice, the animals developed epilepsy.
Next, the investigators looked at brain tumors, which can also cause epilepsy. One rare brain tumor type involves both glial cells and neurons, triggering epilepsy. Sequencing genetic information from cells in the tumors revealed that in 46% of affected patients, the glial cells and the neurons in the tumor shared an identical mutation.
“It means that the…neural stem cell already contained this… mutation,” said Lee, “and differentiated into the neuron and the glial cell.”
That could explain the high rate of disease recurrence in patients with these tumors; even if surgeons remove the entire tumor, the mutant stem cells might continue to produce more defective neurons and glial cells, which could then seed the growth of a new tumor.
To confirm that, Lee’s team collected an additional round of samples, this time sequencing cells not only from resected brain tumors and blood, but also from the subventricular zone in each patient’s brain, an area rich in undifferentiated neural stem cells. They found the tumor-associated mutation in the subventricular zone samples as well as the tumors, indicating that the error occurred in the neural stem cells, whose neuronal and glial descendants then migrated to where the tumor grew.
The researchers are also looking at neurodegenerative disorders such as Alzheimer’s disease.
“We hypothesized that somehow brain somatic mutation maybe accumulates over aging, and maybe associates with [Alzheimer’s disease development],” said Lee.
By performing deep sequencing on brain tissues from patients with and without Alzheimer’s disease, he and his colleagues identified somatic mutations unique to the diseased brains, supporting their theory.
In addition to identifying the underlying mechanisms behind neurological diseases, Lee is trying to help patients in other ways. In one effort, he has begun providing his results to clinicians to use in genetic counseling. Because conditions caused by somatic mutations aren’t heritable, while those caused by germline mutations are, patients who might be considering having children need to know which category they’re in.
The investigators are also trying to find ways to repair or mitigate the effects of somatic mutations in the brain, but it’s a tall order.
“Even if we found a molecular genetically validated target in the patient’s brain, it would be very difficult to develop a traditional drug to penetrate the blood-brain barrier and regulate the target,” Lee explained.
Instead, he’s hopeful that chemically modified strings of nucleic acids, called antisense oligonucleotides, will be able to target the somatic mutations he’s identified.
“I believe in the next five, ten, or twenty years, we probably can solve a lot of the rare neurological disorders,” he said.
Different Diseases, Different RNA Splices
Adrian Krainer won the 2020 Innovators in Science Senior Scientist Award, recognizing years of work spent developing treatments for rare diseases. Krainer and his colleagues were the first to develop an effective drug to treat spinal muscular atrophy. Affecting about 1 in 10,000 people worldwide, spinal muscular atrophy is an inherited genetic disease caused by a defect in the SMN1 gene. SMN1 encodes the SMN protein, which is essential for motor neuron survival. Patients with the mutation experience progressive loss of motor neurons, leading to loss of muscle control and, in most forms of the disease, early death.
Another gene, SMN2, also encodes the SMN protein, but cells usually splice out one of the protein coding sequences, or exons, from the SMN2 messenger RNA, preventing it from making the full-length protein. As a result, 80-90% of the protein translated from SMN2 RNA is truncated, nonfunctional, and rapidly degraded by the cell. Krainer reasoned that preventing the exon-skipping event might allow patients’ unmutated SMN2 genes to produce more functional SMN protein, overcoming the deficit caused by their mutated SMN1 genes. To do that, his team turned to antisense oligonucleotides, which encode the complementary, or antisense, sequence of a specific RNA target. When introduced into a cell, the antisense oligonucleotide binds specifically to its target sequence, triggering various cellular responses.
By designing an antisense oligonucleotide that altered the splicing of SMN2 messenger RNA, the researchers were able to get SMN1-mutant cells to produce more functional SMN protein. Subsequent preclinical and clinical trials proved that their antisense oligonucleotide also works in spinal muscular atrophy mouse models and in patients, respectively, significantly mitigating their motor neuron losses.
“Therefore this is a way that allows them to make closer to normal levels of a functional SMN protein in the presence of this drug,” said Krainer.
The oligonucleotide, now sold as nusinersen (Spinraza), was approved in the US in 2016 and the EU in 2017. Over 11,000 patients now receive it worldwide.
Nusinersen (Spinraza) pioneered many aspects of molecular medicine.
Based on the success of nusinersen, Krainer and his colleagues have begun looking at other RNA processing events to target with antisense oligonucleotides. One project focuses on familial dysautonomia, an inherited genetic disorder that affects only 310 known patients worldwide. These individuals have profound defects in their sensory neurons and autonomic nervous system, leading to symptoms that range from insensitivity to pain to difficulty swallowing.
“It is a very severe disease, a rare disease with a complex set of symptoms,” said Krainer, adding that “median survival is about 40 years of age.”
The condition is caused by a mutation in the gene for a protein called ELP1. As in SMN2, the mutation causes one exon of the gene’s messenger RNA to be spliced out, leading to a loss of functional ELP1 protein.
“So, we started targeting this aberrant splicing event using the same screening strategy and the same chemistry that we used…for spinal muscular atrophy,” said Krainer.
That effort identified an antisense oligonucleotide that can reverse the ELP1 RNA splicing defect in cultured cells from patients, as well as a transgenic mouse model.
“We feel that this is ready for clinical development; it is a challenge, though, because of the rarity of this disease,” said Krainer.
With only a few hundred patients in the US and Israel, the market for familial dysautonomia therapies is minuscule, and effective screening of potential carriers of the affected gene has led to very few new patients being born.
Not all RNA splicing-related diseases are rare, though. Work by several researchers has shown that in at least some cases, a change in the splicing of messenger RNA can help cancer cells grow. Alternatively, spliced forms of the messenger RNA for the PKM gene can produce two different isoforms of the metabolic enzyme pyruvate kinase. PKM1 predominates in normal adult tissues, while tumors and some developing tissues favor PKM2 production.
Using the same approach that worked in their rare disease work, Krainer’s team screened antisense oligonucleotides and identified candidates that bound the PKM messenger RNA and directed its splicing to favor PKM1 protein production. Putting these oligonucleotides into hepatocellular carcinoma cells causes the cells to shift their metabolism and slow their growth. In a mouse model of hepatocellular carcinoma, injecting the antisense oligonucleotides led to a significant reduction in tumor growth compared to control animals treated with saline solution.
Annemieke Aartsma-Rus, PhD Leiden University Medical Center
Don Cleveland, MD, PhD University of California, San Diego
The Kindest Cut
Annemieke Aartsma-Rus began the meeting’s third session with a presentation about her group’s efforts to address Duchenne muscular dystrophy with antisense oligonucleotides. While Krainer’s approach to rare diseases focuses on conditions where an exon needs to be added back into a messenger RNA, Aartsma-Rus described a case where it’s better to remove one.
Duchenne muscular dystrophy is an X-linked genetic disorder. In most cases, a mutation in the dystrophin gene shifts the messenger RNA’s reading frame, causing translation of the dystrophin protein to fail.
“Patients become wheelchair dependent around the age of 12, need assisted ventilation around the age of 20, and generally die in the second to fourth decade of life,” said Aartsma-Rus.
A related but milder disorder, Becker muscular dystrophy, also involves a deletion in the dystrophin gene but doesn’t shift the messenger RNA’s reading frame. As a result, patients with Becker muscular dystrophy produce partially functional dystrophin and exhibit a slower disease progression.
Skipping an exon in the RNA can fix a frame-shift mutation.
Looking at the affected DNA and RNA sequences, Aartsma-Rus reasoned that most Duchenne muscular dystrophy patients could make Becker-like dystrophin, if their cells could simply skip the affected exon in their dystrophin messenger RNA. To test that, she and her colleagues developed chemically modified antisense oligonucleotides that would remain stable in blood and tissues, and began testing them as potential drugs. By designing an oligonucleotide that targeted RNA splicing, the team restored dystrophin expression in cultured cells carrying a Duchenne muscular dystrophy mutation.
The researchers discovered a potential roadblock in a mouse model: antisense oligonucleotides injected into the animals’ tail veins were absorbed almost entirely by the liver and kidneys. The investigators could inject the molecules directly into muscles instead, but that clearly wouldn’t be a practical way to deliver treatment to patients.
“We have over 700 different muscles, and you’ll have to treat patients repeatedly,” said Aartsma-Rus, “so local injection of each and every muscle weekly or even monthly is likely not realistic.”
However, in a mouse model of Duchenne muscular dystrophy, the team discovered that oligonucleotides injected into the animals’ tail veins were absorbed into muscles ten times better than they had been in wild-type mice.
“The first time we thought we’d made a mistake, so we repeated it a couple of times,” said Aartsma-Rus, “but every time we saw that there was higher uptake by the dystrophic muscle than the healthy muscle.”
Dystrophin deficiency causes muscle cells to become more permeable, leading to leakage of cellular components, but this leakage works in both directions; the dystrophic cells readily absorbed oligonucleotides that healthy cells excluded.
Flush with this preclinical victory, the team began setting up clinical trials in 2007. The initial multi-center, open-label trial found that the antisense oligonucleotides caused no serious side effects, and eight of the twelve patients tested saw their conditions remain stable throughout the trial. To evaluate efficacy, the investigators moved into a phase 2b trial, which continued to show dose-dependent effectiveness in treated patients. However, a larger phase 3 trial yielded disappointment, with no significant difference in outcomes between treated and control patients.
“So, what happened [to explain why] we see these beneficial effects in the phase 2 trial, but in the phase 3 trial we see no effect?” Aartsma-Rus asked.
Analyzing the results and the disease further, she realized that the trials were built on the flawed assumption that the patients’ progression would be linear. Instead, they realized that younger patients tend to remain stable for an extended period, followed by a rapid decline later in life. By mixing different ages in the phase 3 trial, patients with worse disease symptoms likely masked any treatment benefits in those with milder symptoms.
Looking at the trial’s failure, Aartsma-Rus concluded that she and her colleagues should have opened discussions with regulatory agencies sooner, and studied the natural history of the disease more thoroughly, before initiating the phase 3 study. Unfortunately, the expensive late-stage failure has soured companies on further clinical development of exon-skipping antisense oligonucleotides for Duchenne muscular dystrophy. Aartsma-Rus has since focused on preventing such an outcome in the future.
“Now we have an open dialogue with academics, with patients, with regulators in the EU, and it is also starting in the US, developing new outcome measures,” she said, adding that “future trials will be better.”
Batting for Lou Gehrig
Don Cleveland discussed his group’s efforts to treat neurodegenerative diseases in the brain, especially those that develop gradually with age. In many of these conditions, such as Alzheimer’s and Parkinson’s disease and amyotrophic lateral sclerosis, “the genes that contribute to disease are all widely expressed…throughout the nervous system, not within individual classes of neurons,” said Cleveland. Mechanistic studies have suggested that decreasing the expression of the defective gene products in some of these cells could moderate the course of disease, so Cleveland and his colleagues set out to do just that.
The researchers first focused on amyotrophic lateral sclerosis (ALS), also known as Lou Gehrig’s disease. About four to five million people alive today will die of ALS, a progressive neurodegenerative condition that can be inherited or occur spontaneously in adults. One inherited form of the disease stems from a mutation in the gene for superoxide dismutase, which causes neurons to die through mechanisms that aren’t entirely clear yet.
Using the same strategy as his co-speakers, Cleveland’s lab designed antisense oligonucleotides that bind specifically to the superoxide dismutase messenger RNA and target it for degradation in the cell. That decreases the level of the enzyme, an intervention that had previously been shown to ameliorate ALS progression in a mouse model of the disease. The next challenge was delivering the oligonucleotides to affected neurons in the brain.
Antisense oligonucleotides have immense potential to be used as drugs against a wide range of diseases.
“These DNA drugs were ten to fifteen times the size of a typical drug, and they’re heavily charged,” said Cleveland, “so the pharmacology textbooks all said that there was no uptake mechanism that would permit them to be efficiently taken up [by neurons].” Nonetheless, he continued, “we tried it anyway, and it turns out that the cells of the nervous system hadn’t read the textbooks.”
Injecting the antisense oligonucleotides into the cerebrospinal fluid of mice genetically modified to develop severe ALS doubled the animals’ survival times.
While the superoxide dismutase defect was the first ALS mutation discovered, the most common cause of the inherited form of the disease is a mutation in a gene called ORF72, which inserts extra nucleotides into a non-coding region of the gene. This causes defective messenger RNA to accumulate, killing neurons because of a lack of functional ORF72 gene products and the accumulation of toxic byproducts of the altered gene. Antisense oligonucleotides targeting the defective RNA, however, inhibit its accumulation without reducing the production of working ORF72 gene products in cultured cells.
In an animal model of the ORF72 defect, the results were even more impressive.
“We dosed these animals [with the antisense oligonucleotides] at the age of disease onset and asked what happens, and the answer is we prevented further disease development for the life of those animals with a single dose injection applied at the initial signs of disease,” said Cleveland.
His team initiated clinical trials on this therapy in 2018, just seven years from the date when researchers had first published the data showing the ORF72 mutation caused ALS.
Although it’s an important target for research, inherited ALS accounts for only 10% of the disease’s total cases. In 90% of patients, the condition develops spontaneously due to somatic cell mutations later in life. Many of these cases involve mutations in the TDP-43 gene, which encodes a nuclear protein that regulates Stathmin-2, which in turn plays a critical role in regulating the cytoskeleton in neurons. TDP-43 normally binds the Stathmin-2 precursor RNA and ensures that it gets spliced properly into messenger RNA. Mutations that inactivate TDP-43 cause a loss of functional Stathmin-2, which is a hallmark of sporadic ALS.
Using cultured neurons, Cleveland and his colleagues found that a properly designed antisense oligonucleotide could compensate for the loss of TDP-43 activity, restoring normal RNA splicing and Stathmin-2 expression.
“This now enables a strategy for therapy for sporadic ALS,” said Cleveland.
If the result holds in other preclinical models, he expects to take that approach into clinical trials in 2023.
Besides correcting specific defects within a cell, antisense nucleotides can potentially redirect a cell’s fate entirely. That’s the central theme of another project in Cleveland’s lab, in which the team is causing astrocytes to change their identities. Astrocytes are companion cells in the nervous system that arise from the same stem cells as neurons. Using antisense oligonucleotides, the investigators can suppress two genes that direct cells into the astrocyte lineage, causing them to become neurons instead. Cleveland is initially focusing on treating Parkinson’s disease with this approach, but he explained that “this…conversion of astrocytes into replacement neurons may be broadly applicable for neurogenic disease.”
Huda Zoghbi Jan and Dan Duncan Neurological Research Institute, Texas Children’s Hospital
Maybe Not So Rare
Huda Zoghbi gave the meeting’s keynote presentation, which covered her work on Rett syndrome. Caused by spontaneous mutations in the MECP2 gene on the X chromosome, Rett syndrome is a progressive neurodegenerative disease that primarily manifests itself in girls. MECP2 is critical for gene regulation in neurons. Because females carry two copies of the X chromosome and an inactivate one in each cell, an inactivating mutation in MECP2 impairs the function of 50% of the affected individual’s neurons. That manifests itself as a rapid regression in motor and cognitive abilities by age two.
In boys, who have only one X chromosome, inactivation of MECP2 is generally lethal before age two. They don’t live long enough to develop the classic symptoms of Rett syndrome. However, recent work has revealed that some males acquire mutations that cause less severe defects in MECP2.
“What we’ve learned is when people carry milder mutations, we will see milder phenotypes, such as mild learning disability with…neuropsychiatric features,” said Zoghbi.
These individuals’ phenotypes can range from autism to hyperactivity or schizophrenia, but most die by middle age due to neurodegeneration. Females with mild defects in MECP2 show non-random inactivation of their X chromosomes, favoring the healthy copy of the gene and enabling them to develop and live normally. Some patients also have duplications in their MECP2 genes, often leading to severe neurological problems and premature death.
To understand the mechanisms driving Rett syndrome, Zoghbi and her colleagues developed a series of genetically modified mice carrying various duplications or mutations in MECP2. Consistent with the findings in humans, these animals display a spectrum of phenotypes depending on the severity of their MECP2 disruptions.
“The brain is very sensitive to the activities and functions of this protein, and we’ve done a lot of studies on both the loss and the gain models,” said Zoghbi.
She and her colleagues found that all types of neurons require functional MECP2 to operate normally.
Mutations affecting different types of neurons can cause a wide range of neurological phenotypes.
Next, Zoghbi and her colleagues tried inactivating MECP2 in excitatory and inhibitory neurons separately. They found that in both cases, animals developed obesity, lost motor coordination, and died young. However, targeting MECP2 only in inhibitory neurons led to more learning and social defects in the animals, while inactivating it only in excitatory neurons caused more anxiety and tremors. These phenotypes represent the downstream effects of the genes MECP2 would normally regulate.
“Given that it’s important for practically every cell, really there’s two major ways you can think of treating this disorder, either gene replacement therapy…or perhaps exploring modulation of the [MECP2 regulatory] circuit,” said Zoghbi.
Taking the latter approach, the investigators implanted electrodes into the brains of mice to deliver small electrical pulses. This type of deep brain stimulation, which has been shown to reverse many types of neuronal signaling and development defects, is already approved for human treatment of several neurological disorders. Stimulating the brains of Rett syndrome model mice leads to significant recovery in their learning, memory, and motor abilities that persists for weeks after treatment.
“It was really quite a dramatic rescue in that all these phenotypes normalize, and their normalization…lasted for several weeks,” said Zoghbi.
The treated animals’ neurons also displayed gene expression patterns similar to wild-type animals, whereas untreated animals showed significant gene dysregulation.
“The Rett brain, at least in mice, is responsive to neuromodulation,” said Zoghbi.
Looking at the MECP2 gene itself, Zoghbi’s team identified regulatory sequences that control its expression level. Altering these sequences to increase or decrease the amount of MECP2 expressed in mice underscored their earlier findings, showing that even modest changes in MECP2 levels led to detectable neurological phenotypes.
Like other speakers at the meeting, Zoghbi and her colleagues are also exploring the potential of antisense oligonucleotides as therapies. That approach seems especially promising for patients with duplications in MECP2 that lead to overexpression of the gene. In mice that recapitulate this condition, the researchers found that treatment with antisense oligonucleotides against MECP2 could reduce the amount of functional protein in neurons down to wild-type levels. The treatment reversed the animals’ motor defects.
Titrating the antisense oligonucleotide dosage also revealed that even modest decreases in excess MECP2 can lead to major improvements in symptoms.
“If you can even partially decrease the protein…you will probably rescue quite a bit of the features of the disease,” Zoghbi said. She added, “I’ve really never worked with a protein that is so exquisitely sensitive to the levels.”
Graciana Diez-Roux, PhD Telethon Institute of Genetics and Medicine
David Fajgenbaum, MD University of Pennsylvania
Anne Heatherington, PhD Takeda Pharmaceuticals
Silver Linings
The meeting’s general session concluded with a panel discussion led by Brad Margus, co-founder and CEO of Cerevance. With a background in business, Margus moved into rare disease drug development after his daughter was diagnosed with ataxia-telangiectasia, a genetic disorder that causes neurodegeneration and immune dysfunction. The panel also featured Graciana Diez-Roux, chief scientific officer at the rare disease-focused Telethon Institute; David Fajgenbaum, a physician-scientist who both studies and suffers from Castleman syndrome; and Anne Heatherington, a data scientist for Takeda Pharmaceuticals with extensive experience studying Duchenne muscular dystrophy.
Panel members discussed the need for improvement in collaborations between patients and researchers.
“There is a lot of miscommunication within the rare disease research space, [but] I think there’s been a really great trend for groups like Takeda and others toward engaging patients in the research process,” said Fajgenbaum, adding that “I also think clinicians can really be a part of this.”
Besides improving clinical trial recruitment, involving patients more directly in research can have far-reaching benefits for scientists.
“It’s incredible how our PhD students, when they have the chance [to interact] with the patients and [get] to know the patients’ organizations…how their motivation and their love for what they do changes,” Diez-Roux said.
Besides increasing collaborations between patients and scientists, all of the panelists endorsed the need for strong, well-defined partnerships with pharmaceutical companies. Margus described his company’s efforts to improve data collection and sharing for ataxia-telangiectasia, which included building a system that uses wearable devices to collect movement data from patients around the clock.
“The data [are] truly owned by the families and the community, and we can make decisions about sharing the data with academics or any researcher in the world in a matter of days,” said Margus.
Good partnerships require more than just good databases, though. Academic researchers accustomed to independent, curiosity-driven experimental design and flexible deadlines sometimes have trouble accommodating pharmaceutical companies’ urgent, goal-directed needs.
“I think the model has to be somewhere between…the industry knowing how to deal with the academic research and academic researchers being open to notice that industries have…different goals in some respects,” said Diez-Roux.
The group also discussed the impact of the COVID-19 pandemic. In the short term, of course, the global shutdown caused by the SARS-CoV-2 virus has halted or delayed many rare disease studies. However, panelists agreed that some of the innovative approaches developed for the pandemic response could transform many aspects of rare disease research in the future.
“We have been very involved in a lot of the COVID alliances, and have been steeped in novel ways of working,” said Takeda’s Heatherington.
As an example, she pointed to the company’s involvement in multi-corporation consortia to develop new therapies and even entirely new platforms for therapies.
“That’s a real breakthrough in terms of how we do our business, that extent of collaboration for [competitors to] come together,” Heatherington continued.
At the same time, “the public is realizing more how important research is, and this goes for COVID, but I think it goes for all diseases,” said Diez-Roux. Both she and Heatherington also pointed out that the pandemic has underscored the potential tradeoffs between speed and safety in therapeutic development, and highlighted the importance of oversight in clinical trials.
The meeting concluded with a virtual poster session, featuring rapid-fire presentations of some of the newest research in rare diseases and offering attendees the ability to interact with the presenters directly. Like the other presentations, the posters represented the diversity and enthusiasm of rare disease researchers.
“What makes me optimistic is the passion and the knowledge…and the fact that we have people that are so dedicated to rare diseases,” said Heatherington.
Anthony Fauci says vaccine developers can build on many years of research to stay ahead of SARS-CoV-2 variants
Published February 02, 2021
By Alan Dove, PhD
Coronavirus Covid-19 Protection and Vaccine. Doctor drawing up solution from vaccine bottle and filling syringe injection for patient vaccination in medical clinic, Coronavirus in background
Anthony Fauci, MD Dir., National Institute of Allergy and Infectious Diseases
As concerns swirl around the emergence of novel variants of the SARS-CoV-2 coronavirus, Anthony Fauci, Director of the National Institutes of Allergy and Infectious Diseases, points to reassuring results from both clinical and laboratory tests, and underscored the ability of scientists to adapt rapidly to the evolving pandemic.
The new variants, one first isolated in the UK and one in South Africa, carry mutations in the gene encoding the spike protein that all of the currently approved and candidate vaccines target. Preliminary experiments have shown that some of the antibodies patients raise in their bodies against the spike protein don’t bind as well to the variant forms.
Speaking at a New York Academy of Sciences symposium, The Quest for COVID-19 Vaccines, Fauci explained that “the diminution [in binding] is about five or six fold,” but remains within the range expected to be protective. He added that real-world clinical trial data backs that up, with the latest results from Johnson & Johnson’s COVID-19 vaccine showing 85% efficacy in preventing severe disease even in a South African cohort where most of the cases involved one of the feared variants.
Building Upon Decades of Previous Research
At the same time, decades of prior work have positioned vaccinologists well to respond quickly if the virus does evolve to circumvent vaccine-mediated immunity. Indeed, the COVID-19 vaccine development effort to date has already illustrated how fast that response can happen. Less than a year after the first genome sequence of the SARS-CoV-2 coronavirus was published, millions of people around the world were receiving highly effective vaccines, a result Fauci calls an “extraordinary historic accomplishment.”
Putting this astonishing achievement in perspective, Fauci compared it to previous vaccine efforts. “Even as we developed more technologies, measles, for example, took ten years, hepatitis B took sixteen years, but…COVID-19 took 11 months,” said Fauci. The new pandemic vaccines were in fact decades in the making, building on a scientific legacy that is also helping researchers prepare to address new viral variants.
Tracing the history of the current crop of COVID-19 vaccines back to work on HIV vaccines in the 1990s, Fauci described the basic and applied science that built a system spring-loaded to respond to a pandemic. “Then along came SARS-CoV-2, and again, [through] that same work that dates back years, the marriage between vaccinology and structure-based vaccine design” quickly revealed the most promising antigen target for COVID-19 vaccines.
Structure-Based Design
In structure-based design, scientists begin with the atomic structure of an antigen, and predict how modifications to it could enhance its potency. For SARS-CoV-2, that process identified a specially modified version of the virus’s spike protein as the best antigen; that antigen is now the basis for nearly all currently approved and candidate COVID-19 vaccines. A parallel body of work had shown the capabilities of modern vaccine platforms such as messenger RNA, recombinant proteins, and genetically engineered viral vectors.
As the new vaccines finished preclinical trials early in 2020, their developers already had access to an established network of clinical trial sites.
“The extraordinary investments that were made decades ago in putting together the HIV clinical trial network was immediately adapted, by using many of these sites [as] part of the COVID-19 Prevention Network,” said Fauci, adding that the first phase 1 clinical trial began just over 60 days after the release of the SARS-CoV-2 genome sequence, a head-snapping speed for clinical development.
Effectively Combatting New Variants
Turning to the new variants originally seen in the UK and South Africa, now known as B.1.1.7 and B.1.351 respectively, Fauci added that the nature of the new vaccines’ underlying technologies will also make them relatively straightforward to update if necessary.
“Multiple companies…are now doing an upgraded version of their vaccines, which would likely serve as a boost,” said Fauci.
Regulatory authorities are already pondering how to handle such booster vaccines, but they may be able to accept an abbreviated approval process similar to the one used for seasonal flu shots. In that approach, the new boosts “would be considered by the FDA as literally a strain change,” subject to only two phases of safety and immunogenicity tests instead of full-scale phase 3 trials, said Fauci.
Efficacy versus Effectiveness
The vaccine effort also now faces obstacles that are harder to address through science and technology. Fauci contrasted the ideas of efficacy and effectiveness of a vaccine. While the former can be calculated from clinical trial data, the latter stems from how widely a community adopts the vaccine; a highly efficacious vaccine that few people get will fail to curb the virus’s spread.
“One of the challenges that we are facing [is apparent] if you look at the intent to get COVID-19 vaccines,” said Fauci, pointing to surveys that show that significant numbers of Americans remain hesitant about vaccination. “We need to respect that, but we need to try and convince them of the importance, for their own safety and the safety of their family and the American public, to get vaccinated,” he added.
Though he has made a preliminary estimate that “herd immunity,” or overall protection of the population, could require vaccination of 70-85% of the population, Fauci cautioned that those figures are just an educated guess; only long-term monitoring of infection rates will reveal when the country is effectively protected.
Lewis C. Cantley’s discovery of the enzyme phosphatidylinositol-3-kinase (PI3K) paved the way for a better understanding of cellular metabolism and its role in human diseases. In response to insulin, PI3K signals through lipids to activate a cellular cascade resulting in increased glucose uptake and subsequent cell growth and division. Cantley’s work has led to new cancer therapies, as PI3K pathway mutations are among the most common to drive cancer development, and a better understanding of insulin resistance in diabetes.
For his groundbreaking discovery of PI3K and critical body of research, Lewis C. Cantley, PhD, of Weill Cornell Medical College, received the 2020 Dr. Paul Janssen Award for Biomedical Research. On September 16, 2020, the New York Academy of Sciences hosted the award symposium to celebrate his achievements. Following Cantley’s award lecture, other experts in the field shared their work on the intersection between cellular metabolism, biology and disease.
Symposium Highlights
Differences in cell metabolism across cancer types may help explain why cancer cells are differentially sensitive to drugs that target metabolism.
The tumor suppressor protein p53 regulates several pathways that manage the production of reactive oxygen species in the mitochondria.
Metabolic pathways represent a powerful and to-date, underappreciated set of therapeutic targets for cancer.
Drugs that regulate metabolic pathways involved in cell differentiation are promising targets for acute myeloid leukemia.
Cancer researchers are coming to appreciate how a patient’s diet can be therapeutically applied and may directly modulate their disease progression and therapeutic response.
Speakers
Lewis C. Cantley, PhD Weill Cornell Medical College
Matthew Vander Heiden, PhD Massachusetts Institute of Technology
Karen Vousden, PhD Francis Crick Institute
Ulrike Philippar, PhD Johnson & Johnson
Costas Lyssiotis, PhD University of Michigan
Discovering Phosphatidylinositol-3-kinase and Its Link to Cancer
Speakers
Lewis C. Cantley Weill Cornell Medical College
Metabolism, Health, and Cancer
Lewis C. Cantley described how the discovery of the enzyme phosphatidylinositol-3-kinase (PI3K) and its signaling pathway led to the development of a new class of cancer drugs called phosphoinositide-3 kinase inhibitors.
He traced his foundational work on PI3K inhibitors to a single slide that his then-graduate student, Malcolm Whitman, produced for a lab meeting in 1987 when he was at Tufts University in Boston. The lab was studying phosphatidylinositol and its role in a signaling cascade regulated to insulin and cell growth. They purified an insulin-activated lipid kinase and found that when activated, it is associated with proteins linked to cancer.
The slide from a 1987 lab meeting that sparked decades of research.
At the time, researchers thought that phosphatidylinositol gets phosphorylated at position 4 on its sugar ring to produce a lipid called PI4P, which is involved in cell regulation. But Whitman found these phosphorylated lipids seemed to have two subtypes—one consistently ran a millimeter further on the gel. “That one-millimeter difference convinced me, as a chemist, that these had to be different species,” Cantley recalled. It turned out that their insulin-regulated kinase—now called PI3 kinase—produces a different molecule, called PI3P, and modulates a previously undiscovered insulin-regulated pathway that regulates the cell’s ability to take up glucose.
Cantley’s team went on to elucidate how PI3K regulates cells’ response to insulin signaling. “Almost every step in the first half of glycolysis is regulated by the PI3 kinase pathway,” he said. Collaborating with a team led by John Blenis, now at Weill Cornell Medicine, Cantley’s also fleshed out the connection between PI3K and multiple other cancer related signaling pathways, such as PTEN, Ras, and mTOR. Cantley called it “really quite remarkable” that “every tumor has at least one of the molecules in this pathway mutated—and many have several.” Indeed, accumulating research since then shows PI3K is one of the most frequently mutated oncogenes in cancer.
Although four different genes encode PI3Ks, just one of them—PIK3CA, which mediates insulin response, is widely mutated in cancers. Yet despite extensive effort, researchers have struggled to get PIK3CA-targeted drugs approved. Because this form of the protein mediates insulin activity, any drug that targets it makes patients insulin-resistant. “So you’re fighting the battle of insulin resistance as you are trying to treat the cancer, Cantley explained.
PIK3CA mutations are especially prevalent in uterine, cervical, breast, and ovarian cancer. In 2009, Cantley received a $12 million grant from the Stand Up To Cancer foundation to form a “dream team” of researchers to investigate how to develop PI3K inhibitors for women’s cancers and explore effective drug combinations. Through this grant, Cantley and his team conducted an early-stage trial of BYL719 (Alpelisib), a PIK3CA inhibitor developed by Novartis, in combination with a chemotherapy agent called letrozole, which lowers estrogen production, in people with metastatic breast cancer. The combination reduced glucose uptake to tumors and extended progression-free survival by roughly one year. The US Food and Drug Administration approved it in 2019.
PI3 Kinase inhibitor BYL719 combined with the chemotherapy agent letrozole reduced glucose uptake from tumors of a patient over the course of one month.
But in that early clinical trial, Cantley noticed that although the drugs’ response correlated with PIK3CA mutations overall, it was uneven; some patients with PIK3CA mutations didn’t respond, and some with mutations in unrelated genes did. “This was not a clear home run,” he said. “I argued, as we looked at the data, that maybe this has something to do with patients’ insulin levels.”
The insulin receptor (IR) is expressed in most tumors. Cantley and his colleagues wanted to interrupt the cycle in which high insulin levels trigger the IR and PI3K activity in the tumor, ultimately driving glucose uptake. To do so, the researchers tracked insulin levels in patients and mice taking PI3 kinase inhibitors. All three drugs they tested raised insulin levels 20-fold. In additional experiments, cells grown from patients with PIK3CA tumors died when exposed to PIK3CA inhibitors but were rescued when insulin was added. “So those ambient levels of insulin really are keeping the tumor alive,” Cantley said.
In subsequent studies, Cantley and his team tested the effects of insulin-lowering drugs, including metformin, as well as a ketogenic diet in mice. They found that a ketogenic diet effectively maintained low glucose and insulin levels while administering a PI3K inhibitor. In mice carrying tumors with a PIK3CA mutation, combining the PI3K inhibitor with a ketogenic diet significantly suppressed tumor growth compared to the control group. “This really tells us that keeping insulin down during the treatment with a PI3 kinase inhibitor could potentially have huge improvements in patient responses,” Cantley said.
Researchers are looking more closely at the effect of a ketogenic diet on the efficacy of PI3K inhibitors for endometrial cancer, breast cancer, and lymphoma. Previously a postdoc in Cantley’s lab and now at Weill Cornell Medicine, Marcus Goncalves is spearheading this effort with a trio of clinical trials currently enrolling patients.
Matthew Vander Heiden Massachusetts Institute of Technology
Karen Vousden Francis Crick Institute
Metabolic Limitations in Cancer
All cells in the body, including cancer cells, exist in different metabolic environments, and thus have different nutritional resources available to them, said Mathew Vander Heiden. Cancer cells have especially high metabolic needs because by definition, they proliferate—doubling the mass of proteins, nucleic acids, and lipids in order to go from one cell to two. Understanding how different types of cancer cells reorganize their metabolic pathways to accomplish this feat can bring insight into the role metabolism plays in cancer therapeutics.
Tissues solve their metabolic needs differently. Metabolism in brain cells, for example, differs from that in liver cells. These differences must be reflected in the gene expression patterns of the tissues’ metabolic networks. When a cell becomes cancerous, it takes its existing metabolic network, based on its environment, and reorganizes it to support its proliferation. That’s why cancers exhibit varied metabolisms and are sensitive to different therapies, Vander Heiden said.
His lab studies how a cell’s environment constrains its metabolic network. In one recent study, the researchers characterized the nutrients available in the interstitial fluid of pancreatic and lung tumors in mice. Transplanting a tumor into a different tissue site changed the nutrients available to it. But the mutational profile of a tumor had a much weaker effect on its metabolism. More recent human data suggests that nutrient profiles in the interstitial fluid of kidney cells and kidney tumor cells is similar. The findings suggest that nutrient availability is an intrinsic property of different tissues, and that cancer must adapt to the food available in a specific area. “That’s a cool idea, because it has a profound effect on how we think about metastasis,” said Vander Heiden. His lab has conducted metabolic phenotyping of mouse cancers transplanted to different tissue sites and found that the most significant outlier in the metabolic profile is in the brain. That matches clinicians’ experience with HER2-positive breast cancer, which tends to respond well to treatment except when the cancer reaches the brain.
To probe tissue-intrinsic metabolic responses, researchers in the lab of Rakesh Jain, also at Harvard, transplanted breast cancer tissue either into mammary fat pads or the brains of mice. They then treated the muse with PI3K inhibitor and found that the tumor shrunk in the mammary tissue but not the brain. Related studies showed that the brain microenvironment partially drove differences in response.
Fatty acid synthesis is increased in the breast cancer tissue transplanted into mouse brain.
In collaboration with Jain’s lab, Vander Heiden’s team implanted tumor cells into the brains and mammary fat pad tissue of mice. They found different metabolic gene expression and activity between the two sites. They also found more glucose uptake into fatty acids in the brain tumor tissue than in the mammary tissue, suggesting that fatty acid synthesis increases in brain metastases. Ultimately, they showed that these differences affect how tumors develop in the brain and facilitate tumor growth. The microenvironment and nutritional differences of tumor cells is key to understanding varied responses to metabolism-targeted therapies.
Metabolic Control of Tumor Progression
P53 is a key tumor suppressor gene. Some seven million cancer patients per year carry a mutant version of it. However, virtually all tumors, even those with a normal p53 gene, have lost p53’s tumor suppressive activity, said Karen Vousden. Early research showed that p53 suppresses tumors but activates cell death and senescence, killing tumor cells. But more recently, Vousden and others report another type of p53 activity, in which it contributes to the cell’s survival and its ability to adapt to stressful conditions, such as the accumulation of reactive oxygen species (ROS). Her lab is examining the gene’s role in metabolic signals such as nutrient fluctuation and oxidative stress.
Next, they looked at p53’s role in adapting to nutrient starvation. Comparing cell lines with p53 to without it, they found that p53 mitigates oxidative stress caused by cells lacking amino acids the body normally produces, such as serine. The absence of serine had stronger negative effects in cells without p53, reflecting the gene’s ability to drive antioxidant defense, Vousden said.
To look at how p53 protects cells from oxidation, the researchers focused on a downstream enzyme called TIGAR. Although the protein’s full suite of functions is still unknown, it promotes the production of NADPH, a molecule that supports antioxidant activity. Cells that lack TIGAR are more sensitive to oxidative stress and can’t maintain NADPH levels. Studies suggest that this effect is specific to mitochondria. Organoids lacking TIGAR have a much higher level of toxic ROS than organoids expressing the enzyme, and treating the cells with mitochondrial antioxidants — but not membrane antioxidant — mitigates this effect.
p53 controls reactive oxygen species via downstream molecules, including TIGAR.
Vousden’s lab also studied the effects of TIGAR during various stages of tumor development. They found that loss of TIGAR impedes tumor growth in both the pancreatic and intestinal adenoma models. Interestingly, mice with these tumors also had an increased rate of lung metastasis. Treating these mice with antioxidants mitigated the effect on lung metastasis, suggesting that ROS influences cancer development differently at different stages of the disease.
Targeting Metabolism and Differentiation Therapy in AML
Acute Myeloid Leukemia (AML) is a critical disease area in Janssen’s drug discovery effort. A clinically heterogenous disease with multiple subtypes, AML is characterized by a diverse landscape of chromosomal abnormalities and gene mutations. One hallmark of AML, myeloid differentiation block, is linked to metabolism, said Ulrike Philippar. Myeloid differentiation in normal cells results in the generation of mature blood cells from hematopoietic stem cells. This process is blocked in AML cells, resulting in uncontrolled proliferation of progenitors, and ultimately, aggressive leukemia. Differentiation therapies have thus been a recent focus of drug development for AML, and unmet medical need for the disease remains high.
Philippar first described two US Food and Drug Administration-approved differentiation therapies. The first, called all-trans retinoic acid, or ATRA, was first used in 1985 to treat acute promyelocytic leukemia (APL), a subtype of AML. ATRA binds to a translocated protein in APL, leading to disruption of the differentiation block. The second therapy, IDH1 and IDH2 inhibitors, treats AML patients with an IDH mutation. The drug came to be used in combination with arsenic trioxide. These agents bind to a translocated protein in APL, disrupting the differentiation block.
Philippar and her team conducted two CRISPR/Cas9 screens to identify novel targets that inhibit proliferation in cell lines in vitro and/or in a bone marrow transplant mouse model in vivo. They identified dihydroorotate dehydrogenase (DHODH), an enzyme located in the mitochondrial membrane involved in pyrimidine synthesis. DHODH is also essential for the production of the nucleotide uridine monophosphate (UMP), the first building block in the production of RNA and DNA synthesis. Researchers, including Philippar and her colleagues, have shown that malignant cells, particularly AML cells, are metabolically dependent on pyrimidine production because they cannot salvage sufficient uridine from the extracellular environment.
Janssen identified a potent, selective proprietary DHODH inhibitor. The molecule strongly inhibited proliferation in 25 AML cancer cell lines. Janssen’s DHODH inhibitor also showed strong antiproliferative activity in primary AML samples. A few patient samples appeared to be resistant to the drug, and Janssen researchers will continue to investigate the basis of that resistance.
Preclinical studies suggest that DHODH inhibition is an effective treatment strategy for AML
The researchers also probed the DHODH inhibitor’s mechanism of action. The molecule induced cell cycle arrest in S phase, resulting in increased apoptosis. Furthermore, treatment with the DHODH inhibitor also increased cellular differentiation in AML cell lines. Adding excess uridine can reverse these effects, which validates the inhibitor’s on-target activity. Janssen’s DHODH inhibitor led to tumor regression in subcutaneous AML xenografts and increased the lifespan of mice bearing disseminated AML cancer cells approximately twofold.
Philippar said that DHODH inhibitor therapy takes away the pyrimidine source and leads to starvation of cells by forcing them into a fasting state. The researchers hypothesize that normal cells can tolerate fasting and recover; however, leukemia and other cancer cells cannot tolerate fasting because they require higher pyrimidine synthesis. Hence, prolonged pyrimidine starvation of leukemia cells results in a cell fate decision leading to differentiation, and ultimately, apoptosis and tumor regression.
DHODH confirms the relevance of metabolic targets for AML. However, the clinical diversity of AML may be a challenge for metabolic drugs, and researchers will have to better understand patient selection as they develop these drugs in the clinic.
Lewis C. Cantley, PhD Weill Cornell Medical College
Matthew Vander Heiden, PhD Massachusetts Institute of Technology
Karen Vousden, PhD Francis Crick Institute
Ulrike Philippar, PhD Johnson & Johnson
Panelists reflected on what moderator Costas Lyssiotis, a former postdoctoral student in Cantley’s laboratory, framed as a key theme of the symposium: harnessing diet as a way to treat cancer.
Cantley stated that previous efforts to use diet to understand cancer have largely failed, because getting trial participants to adhere to a diet and accurately report what they eat is nearly impossible. In a recent clinical trial that tested a ketogenic diet as a neoadjuvant for endometrial cancer, Cantley’s collaborator Marcus Goncalves used the metabolic kitchen at Weill Cornell Medical School to generate 21 meals per week for each trial participant. Weekly blood draws made it possible for researchers to be sure patients adhered to the diet. “To show [that] a dietary intervention works, you have to do it in a very controlled manner, not just tell people what they should eat and hope that they find it at the market,” Cantley said. Ultimately, the aim is to get dietary interventions approved as therapies so that insurance companies will cover them. He noted that companies such as Bayer and Novartis are excited by the possibility because it can potentiate pharmaceutical therapies. “We should hold diets to the same standards we hold drugs to,” said Cantley.
Vander Heiden agreed about the need for more rigorous dietary trials. His lab found that alterations in diet led to changes in the composition of metabolic molecules in interstitial fluid, and presumably those changes extend to nutrients available in different tissues and in blood. Animal studies are especially useful for identifying how nutrient availability changes with diet, he said; and they might point to unexpected differences beyond those already identified for the glucose and insulin pathway and serine.
Translating dietary interventions from animals to humans may not be straightforward. “What happens in mice doesn’t necessarily happen in people,” Vousden said. She and her colleagues are developing a serine-depleted diet for people with cancer, along the lines of low phenylalanine diets prescribed for children with phenylketonuria, an inherited condition that raises the level of the amino acid building block phenylalanine in the blood.
Any nutrient may be modulated for cancer therapy, but researchers must have a firm mechanistic understanding of why that alteration might work. “I think that’s at the heart of whether it will be successful, and whether people will follow these diets,” Vousden said. A solid grounding in the mechanism underlying a possible dietary intervention’s effect can help motivate patients to follow a restrictive diet for their clinical benefit.
Philippar noted that so far, considering diet is not standard practice in industry drug development. But it is potentially important, not just for targets that modulate the metabolism but also for immunological approaches. Researchers now know that diet can affect gut bacteria, which might in turn affect drug response. In clinical trials run by Janssen, she explained, researchers generally check whether a patient is in a fed or fasted state when receiving an experimental therapy, but they do not check on what exactly the patient has eaten.
Single-cell RNA sequencing makes it possible to look at the tumor microenvironment and to determine how changes in diet affect the expression levels of immune genes. In 2019, Cantley, Goncalves and others showed that just one, 12-ounce serving of a sugary drink such as orange juice, apple juice, or soda each day enhances intestinal tumors in mice. A combination of fructose and glucose causes the effect, the researchers found, and knocking out a molecule called ketohexakinase, which phosphorylates fructose, limits tumor growth. The connection to sugary drinks “is very surprising,” says Cantley, “but I think it may explain why we’ve almost tripped the rate of early onset colorectal cancer in young adults in the last 20 years.”
Dr. Krainer’s research examines anti-sense therapy and its application to spinal muscular atrophy.
Published December 15, 2020
By Melanie Brickman Borchard, PhD, MSc
Adrian R. Krainer, Ph.D., St. Giles Foundation Professor at Cold Spring Harbor Laboratory Photo credit: Cold Spring Harbor Laboratory
Adrian R. Krainer, PhD, St. Giles Foundation Professor at Cold Spring Harbor Laboratory, was awarded the 2020 Ross Prize in Molecular Medicine by the Feinstein Institutes for Medical Research and Molecular Medicine for his pioneering work in introducing anti-sense therapy into clinical use and for its successful application to spinal muscular atrophy (SMA), an illness that has been the leading genetic cause of infant death.
“I was surprised to win the Ross Prize and really appreciate it,” remarked Krainer. “I view it as recognition of not just what I have done but of my whole team, which is the people currently in the lab and the ones that preceded them, plus our collaborators. It’s been a collective effort.”
Krainer emigrated from his native Uruguay to the United States in the late 1970s. He studied biochemistry and genetics at Columbia University. Later, during his graduate studies at Harvard, he became excited by a cutting-edge area of research—RNA splicing, a process that removes introns from precursor messenger RNA and joins the exons to enable translation of mRNA into a protein.
After working on the biochemistry of human RNA splicing, he was recruited to the Cold Spring Harbor Fellows Program upon graduation, where he focused on addressing basic mechanisms and regulation of splicing, what he referred to as, “curiosity-driven research, where we were just trying to learn something about how this process works and its natural regulation.”
Advancing Research on Spinal Muscular Atrophy
After spending fifteen years leading studies on the basic mechanisms and regulation of RNA splicing, in 1999 Krainer attended an invitation-only NIH symposium focused on SMA. This symposium was the catalyst for a revolutionary shift in the direction of his work. There, Krainer saw an opportunity to further elucidate the mechanisms he was already working on. He wanted to use this knowledge to find a potential therapy for SMA patients.
“Meetings are hugely important. Because of that meeting a little light bulb went off [related to the intersection of my work and SMA]. Not that I knew how we would solve the problem, but there was a realization that this problem fits really well with things we have been doing and is very worthwhile,” said Krainer.
A year later Krainer made a commitment to study SMA and by 2004 he entered into a partnership with Ionis Pharmaceuticals to focus on the development of Spinraza (generic name Nusinersen), the first FDA-approved drug to treat SMA associated with mutations in the SMN1 gene (approved in 2016). Since then, more than 11,000 people have been treated with this groundbreaking therapy.
“This is the best one can hope for as a researcher. It is really a dream come true that the basic research is translated into an actual drug that saves lives and is changing the quality of life for so many patients and families.”
Krainer added that the success of Spinraza has the potential to spiral outwards.
“It transcends this one disease, because it’s an example of what can be done with the antisense platform, now it can be used again and again for other neurological diseases and beyond.”
Reflecting on His Work
Today, Krainer continues to pursue the basic science aspects of splicing in his lab. Additionally, he seeks to refine the understanding of the complex machinery used for this process. Among other activities, his lab also focuses on antisense technology to develop therapies for other diseases caused by splicing defects and on understanding how splicing factors and dysregulated alternative splicing promote cancer progression.
Krainer sees being a scientist as a “privilege” and very much a collaborative effort wherein “everyone is doing something that they love.” Even so, he recognizes there are many bumps in the road for scientific discovery.
“One has to be very persistent,” he said. “I think that failure along the way comes with the territory. There’s a lot of troubleshooting and persistence required. If something doesn’t work, you try again or try in a different way. So, it’s a constant challenge and that’s part of the fun of the whole thing.”
The Ross Prize in Molecular Medicine was established in conjunction with the Feinstein Institutes for Medical Research and the Springer Nature journal Molecular Medicine.
According to the National Center for Education Statistics, white males made up 53% of all full-time professors in 2018. And while the “STEM pipeline” is becoming more diverse–more than 40% of women and roughly 15% of people of color receive their PhDs in STEM fields–colleges and universities need to implement inclusive policies to initiate change on a large scale.
On October 9, 2020, the New York Academy of Sciences hosted a webinar with Georgetown University Medical Center affiliates to share their progressive efforts to decrease systemic inequities and improve workplace culture at their institution. In 2019, the university launched the Bias Reduction and Improvement Coaching (BRIC) program to raise awareness of unconscious bias and attenuate systemic barriers at institutions with the hope of promoting diversity and inclusion in STEM.
Highlights
Bias impacts application, hiring, and promotion processes, as people make decisions based on shortcuts, unconscious preferences, and assumptions.
The Bias Reduction and Improvement Coaching (BRIC) program brings together a group of individuals from various demographic backgrounds for training in the skills and language needed to raise awareness of bias.
This “train the trainer” model empowers people to feel confident starting conversations about prejudice and how to mitigate bias in their respective departments and workplaces.
Speakers
Susan Cheng, EdLD, MPP Georgetown University Medical Center
Kristi Graves, PhD Georgetown University Medical Center
Caleb McKinney, PhD, MPS Georgetown University Medical Center
Reducing Systemic Inequities in Academia
Unconscious Bias in STEM
Search committees looking to fill a job should be as objective as possible, especially when studies have shown that teams made up of diverse people are more innovative and high-performing. However, people rely on mental shortcuts and assumptions when making hiring decisions. They often use reflexive habits and exhibit unconscious preferences without realizing it.
Caleb McKinney, who trained as a microbiologist, transitioned to science education, and is now an Assistant Professor and Assistant Dean for Graduate and Postdoctoral Training and Development, related this phenomenon of reflexive habits to a “hot pot.” You learn from previous experience to pull your hand away when a stove is hot. With the same mindset, you can use your prior knowledge to make quick assumptions and form preferences about someone. He urged everyone to take an Implicit Association Test online to learn more about unconscious bias.
But how does conscious and unconscious bias impact STEM community development? Assistant Professor and Senior Associate Dean for Diversity, Equity, and Inclusion, Susan Cheng, noted one example. STEM emphasizes innate intelligence over hard work, but in letters of recommendation, professors are more likely to refer to male scientists as “brilliant,” whereas female scientists are “productive.” The way a job description is written says a lot about what admissions may be looking for in a student or what faculty may desire during recruitment. Search committees may deem a person “not a good fit” for the institution. The only way to combat this is to use checkboxes to ensure job description criteria are followed systematically. “Implicit biases are always in the background, and you need to manage them actively,” said Cheng.
Kristi Graves, a clinical health psychologist and Associate Professor of Oncology, explained that bias also affects STEM professionals’ upward trajectories. For instance, scholarly productivity metrics are very numeric and usually include the number of papers published, impact factor for the journal in which you’ve published, and the amount of grant funding you’ve obtained. But faculty members don’t have access to the same opportunities. A male professor going to another male for a collaboration (because he is like him) is an example of similarity bias.
It’s critical to note that Black, Indigenous, People of Color (BIPOC) make up a small percentage of faculty members. BIPOC faculty members often act as the representative BIPOC for diversity panels and mentoring groups, which takes time away from work and research. And the amount of time spent on essential work and research affects prospects for promotions. Graves believes that hiring committees should have explicit discussions about implicit bias throughout the year to increase faculty diversity. “Everyone has bias,” said Graves. “The trick is to try to become aware of the bias, and then when you notice it, you do something about it so the negative impact that flows from that bias is not sustained or perpetuated.”
Although many colleges and universities have increased awareness and implemented more inclusive policies, the culture has not shifted enough to facilitate a more diverse institutional community. Even representative images on posters and brochures should indicate that a university values different types of people in STEM and that the depicted individuals can serve as role models for scientists who want to know what the institution values.
Understanding the BRIC Program
All three panelists have been heavily involved in the Bias Reduction and Improvement Coaching (BRIC) program at Georgetown University. The program leaders selected people from different backgrounds in various departments across the university for the program. Supervisor or departmental approval was required to participate since the program would take away hours spent on “numeric success metrics.” The inaugural group of 27 coaches—five of whom are coach leads—went through four, three-hour immersive sessions held quarterly. During these meetings, which covered the science of bias and its impact on hiring, promotions, retention, and overall workplace culture, participants learned evidence-based strategies to raise awareness and reduce discrimination. Participants led presentations and department talks on what they learned and received feedback from the coach leads.
The program’s goal is to have many people who can confidently initiate conversations about bias in their workplace. It is designed to establish training across the medical center by providing a faculty learning environment, explained Cheng. The messenger is so important because having the information come from a colleague you know and trust to understand the institutional context you work in is invaluable.
Figure 1. The BRIC program schedule included three-hour sessions, with smaller pod meetings in between, and presentation feedback for the participants before disseminating the information to colleagues.
McKinney participated in the BRIC program and pinpointed three main attributes of the initiative. The training provided self-knowledge to reflect upon one’s personal bias, leadership skills to feel equipped to speak up about bias when necessary, and the ability to communicate these strategies when training others. Participants were asked to reflect on their time in the program and took surveys to assess its impact. Additionally, audience members from BRIC coaches’ presentations were surveyed to see if it was scaled to the department, and follow-ups were conducted to see if departments made any significant changes.
Program Outcomes
Although the initial training was geared toward faculty and staff, post-docs and graduate students organized bias reduction workshops and helped create presentations for their departments. Cheng believes that many students have already developed these skills, while faculty and staff are trying to catch up by participating in the available programs. In addition, departments are asking for workshops on microaggressions, anti-racism, and bias. Graves explained that the program built tremendous confidence for those presenting the material in a safe and confidential space. She also shared a reflection from a participant in the program who felt BRIC was “an effective approach to raise awareness about unconscious beliefs and attitudes and to discover biases in a non-confrontational manner.”
By bringing in participants from different sections of the medical center, the BRIC program facilitated collaboration between faculty and staff from various departments who would not typically work together. This teamwork increased cognitive diversity and allowed participants to build on each other’s thoughts in a broad group discussion. McKinney emphasized that BRIC fostered peer mentorship and feedback, and helped strengthen a sense of community throughout Georgetown University Medical Center.
He was impressed with how much he learned about himself while participating in the program. “To be truly empathetic, you have to be self-aware. You have to recognize and challenge the assumptions you may have about people and situations,” McKinney said. “The BRIC programs allows you to put yourself in other people’s shoes. You learn from each other how people’s experiences and backgrounds shape their individual context, and that’s so important for building empathy.”
Metrics for Success
The panelists shared an essential set of standards that needed to be met for the BRIC program to be successful. Most importantly, improving diversity requires commitment from everyone. That commitment starts with raising awareness and then addressing the issues to create a sense of belonging in the workplace. “Once people are more aware of these biases and start to engage in mechanisms to reduce those biases, you can really [assess an] environment that’s hostile and not welcoming,” said Cheng.
Graves sought feedback from leadership at Georgetown before starting the program. “Until you enact specific behaviors and policy changes, it doesn’t mean a lot,” she said. The institution is responsible for creating an inclusive environment for trainees, post-docs, and faculty and ensuring that people have equal opportunities to succeed. Establishing an inclusive environment doesn’t have to be a top-down method; valuable feedback can come from anyone.
Cheng also highlighted the importance of decisions and transparency. Critical decision making, which includes communicating news and defining expectations and limitations, should be collaborative. For example, department chairs should define a clear set of expectations, goals, and values before a selection process, and the selection committee should routinely review those criteria. “In STEM, we should be really good at creating objective definitions of how we know when we’ve made our goal,” said Graves.
In addition, all employees should periodically revisit training on inclusion and bias, not just at the onset of the job. McKinney advocated for structured mentorship for minority groups, including cross-cultural mentoring relationships. “Mentors from majority backgrounds have an opportunity to shape retention by fostering these welcoming environments for junior individuals to succeed,” he said. Mentorship also includes facilitating career identities for graduate students and post-docs. While it is critical to have support and map out your trajectory on an academic career path, mentors can also highlight opportunities in industry and focus on broad career paths.
The Future of BRIC
Bias awareness is critical now, when many interviews and meetings are being held virtually due to the pandemic. Graves saw this as a positive because it allows institutions to create new networks and reach students early on in their academic trajectories. They can reach a wider talent pool, and recruit candidates from various backgrounds who were not previously reached. Companies should also reassess their open opportunities because the way job descriptions are written and where they are posted plays an essential role in who applies. Equal opportunity statements at the end of job descriptions show candidates that a company values diversity and inclusion.
Georgetown University is not the only institution spearheading programs for systemic inequity awareness. Cheng praised numerous universities, such as UCLA, UCSF, and The Ohio State University, who have been at the forefront of implicit bias research and training. All three panelists are eager to continue the BRIC program. They hope that by scaling this bias awareness across Georgetown, there will always be individuals on committees who have been trained and can challenge their colleagues’ assumptions.
While we’ve faced pandemics before, adapting to the realities presented by COVID-19 has been no easy feat. The specific hurdles that members of our community face are varied, but there’s no question that the virus has had an impact on everyone’s life.
Published September 28, 2020
By Roger Torda
We wanted to know how our members are doing: how their work or education has changed; what obstacles they’ve faced; and what opportunities or new ways of approaching their research have emerged. Below are just a few of the stories they’ve shared with us.
Answering the Call to Contribute
We’re incredibly proud of the contributions Academy members have made during the pandemic, from research, to supporting their communities and families, to working at the frontlines. Here is one particularly inspiring story from a member who shifted his focus entirely as the pandemic began.
Joe Thomas (Brooklyn, New York)
“As a PhD student in biomedical engineering, I am very used to doing work that I know won’t have a clinical application for at least 10 years. Earlier this year I found myself thrust into a position where my work would have a meaningful impact on patients the very same day. With widespread academic lab closures around the city, I decided to volunteer in SUNY Downstate’s pathology department. They needed scientists who had experience performing PCR, and I had just learned the technique a few months prior. The lab was severely understaffed for the workload and there was a very real chance that I would be exposed to the virus and become sick. However, I felt called to step in and provide support since I knew that getting timely test results could be a matter of life and death…I went from being a behind the scenes scientist to being on the front lines literally overnight…I know my story isn’t unique, so I applaud all frontline workers who stepped up and put themselves in harm’s way when it mattered.”
Approaching Learning in New Ways
Aditya Chaudhary
Remote learning, whether for a short time or longer term, hasn’t been an easy adjustment. But we’ve also heard stories from students and educators in our network about some of the upsides of these changes, including added perks that might be missed in the future.
Aditya Chaudhary (Lucknow, India)
“I have learned that my teachers, my school, my friends and I are resilient and that we are capable of coming up with creative solutions to problems when we’re faced with unforeseen uncertainties…Another perk is that we can all sleep in just that little bit longer as we don’t have to take into account travel time. Also, by sneakily switching my camera off I am able to learn and eat my breakfast simultaneously!”
Rida Yumn Ahmed (New Delhi, India)
Rida Yumn Ahmed
“I’m in senior year of high school and it’s supposed to be the most important year as it sets the stage for higher education, but we’re lacking access to practicals and missing our experiments in the lab. However, I’ve tried experiments through virtual labs which gives me a sense of conducting the practicals and has enhanced my knowledge as well…Thankfully the Academy has provided virtual platforms like The Junior Academy which has been such a productive and collaborative platform which made quarantine more fun…All this virtual exposure to scientific papers, talks, and projects, has made me realize that STEM has no boundaries and we’re building the future!”
Involving the Whole Family
We even heard from one family with three Academy members, each finding ways to use their interest in STEM to make an impact during the pandemic.
NseAbasi NsikakAbasi Etim (Uyo, Nigeria)
“During the first few months of the COVID-19 pandemic, there was national lockdown in my country. This prevented me from going to teach students and from being in laboratory to conduct research…I resorted to volunteering online to fight COVID-19 by serving as a mentor in #AfricaVsVirus Challenge. My team designed a virtual classroom for online learning for K-12 to higher education, and it was one of the winning projects. I also volunteered as a mentor in Hacking COVID-19 Africa Challenge. Furthermore, I signed up as a mentor in Youth Innovation and DesignBootcamp 2020 on COVID-19, organized by the United Nations Economic Commission forAfrica (UNECA) and its partners. My team, which took first position, designed a kit containing self-sterilized face masks, an enhanced face shield, and a portable UV-light sterilizer for sterilizing Personal Protective Equipment (PPE) in hospitals and at home. So while in lockdown, I was still able to work remotely and contribute to global efforts to fight the coronavirus.”
From left: Nsikak-Abasi Aniefiok Etim, NseAbasi NsikakAbasi Etim, and NsikakAbasi Etim Jr
Nsikak-Abasi Aniefiok Etim (Uyo, Nigeria)
“As a passionate STEM researcher, I was keen to learn how the novel infectious disease was transmitted and how to break the chain of infection in my immediate community. I promptly enrolled in an online course where I received training on key aspects of covid infection and immunity…As the country continues to navigate in the midst of the pandemic, I am still working in a virtual environment to break the chain of transmission and provide technological and non-technological solutions to challenges posed by the pandemic.”
NsikakAbasi Etim Jr. (Uyo, Nigeria)
“A short while into the lockdown, I pondered how to use my time productively. … [This] included taking various courses to widen my scope and knowledge and attending workshops related to my STEM field to fully equip me with skills to enhance my professional growth and development…I had and still have the desire to contribute to fighting this pandemic, so I enrolled in the Mohammed Bin Rashid University of Medical and Health Sciences (MBRU) Community Immunity Ambassador Program which gave me new knowledge to share with my community and help stop the spread of COVID-19…I also participated in various challenges aimed at solving problems posed by the pandemic. This period is really invaluable for me because I can use it to gain new knowledge and skills, and spend quality time with my family.”
Building a New Future
More than anything else, we heard how the pandemic is driving our network to think about the future and how we might use this time to learn lessons that can inform our work and collaborations in the years to come.
Menglu Yang (Boston, Massachusetts)
“I am on my third year of postdoc training, and I was planning to seek a new job at the beginning of this year. I was so disappointed when conferences got canceled, which are essential for job-hunting. But when the stay-at-home order began, I had more time to listen to my heart…I also took a series of zoom lectures on career development. Only during this special time have I had a chance to think seriously about my career path…Also, I have developed another hobby of writing manuscripts outdoors, where being surrounded by nature helps me stay focused.”
Ramik Wiliams
Ramik Williams (New York, NY)
“I work in philanthropy and my work brings me into proximity with several STEM organizations…Going forward I will look to learn from STEM organizations of various sizes and scopes that have successfully implemented a remote working capacity and seek to share any information that might help organizations plan for future, similar situations.”
Rupam Ghosh (Chandannagar, India)
“My labs are unreachable but we are adapting the computational methods for our research, and now I’ve found it is easier and relaxing…In my view, COVID-19 has opened our eyes in many ways, not only to the bad but also to slow down. I think life is changing and after all this ends we shouldn’t try to get back to our past but should work to adapt.”
The brain is affected by bodily changes—including microbiome composition—that influence cognition and behavior. This eBriefing will explore the interaction between the brain, gut & microbiome, with a focus on how the microbiome influences developmental, neuropsychiatric, and immune-related disorders, including socioaffective processing disorders such as autism.
In this eBriefing, You’ll Learn:
How the microbiome is seeded and maintained throughout life
How stress effects health of the microbiome
How changes in microbiome composition result in changes in behavior
The latest research in therapies targeting microbiome
Speakers
John Cryan, PhD University College Cork
Kirsten Tillisch, MD University of California, Los Angeles
Microbiome and Mental Health
John Cryan, PhD
University College Cork
John Cryan, PhD, is focused on understanding the interaction between brain, gut, and microbiome and how it applies to stress and immune-related disorders, including irritable bowel syndrome and obesity and neurodevelopmental disorders such as autism. Dr. Cryan is a Professor & Chair of the Department of Anatomy & Neuroscience at the University College Cork in Ireland. He spent four years at the Novartis Institutes for BioMedical Research in Basel Switzerland, as a LabHead, Behavioural Pharmacology prior to joining UCC and is a Senior Editor of Neuropharmacology and Nutritional Neuroscience and an Editor of British Journal of Pharmacology.
Kirsten Tillisch, MD
University of California, Los Angeles
Kirsten Tillisch, MD, was the first to demonstrate an effect of gut microbial manipulation with probiotics on emotional brain responses. Her ongoing research is focused on the role of the mind-body connection in chronic pain syndromes as well as the effects of mindfulness, hypnotherapy, and other non-drug therapies for irritable bowel syndrome. She is the Chief of Integrative Medicine at the Greater Los Angeles VA and a Professor of Medicine at the David Geffen School of Medicine at UCLA.
Newborns have a limited ability to fight infectious pathogens. As a result, morbidity and mortality are high during the first few months of life, particularly in low- and middle-income countries. Active research is taking place, and great strides have been made to identify the factors that influence the risk of infection and disease in pregnant women and newborns. One promising approach—maternal, neonatal, and early infancy vaccines—has the potential to protect the health of mothers and children worldwide. Although several existing vaccines are safe and effective for use during pregnancy, no vaccines have been formally approved or licensed specifically for use in pregnant women.
On June 23, 2020, the New York Academy of Sciences hosted a symposium to explore challenges and achievements in the development and licensure of maternal vaccines. In a series of keynote and plenary presentations, the symposium covered recent findings regarding the maternal-to-newborn transfer of antibodies, lessons learned from the use of licensed vaccines during pregnancy, new targets for maternal immunization and contextual factors that influence the vaccination of pregnant women and their offspring.
Symposium Highlights:
Infectious disease is one of the leading causes of stillbirth and newborn death around the world.
Because antibodies can be transferred from the mother to the baby, boosting maternal antibodies can help protect the newborn against respiratory or invasive diseases.
Certain vaccines that are routinely used in the general population (e.g., influenza, pertussis), are also recommended for pregnant women to protect both mother and child.
Several pregnancy-specific vaccines, such as Group B Streptococcus, Respiratory Syncytial Virus, and Human Cytomegalovirus, are currently in different stages of development.
Contextual factors, like access to health care during pregnancy and after birth, are important determinants in the success of maternal and neonatal immunization worldwide.
Speakers
Stephen L. Brusatte The University of Edinburgh
Sinéad Farrington The University of Edinburgh
John Marioni European Bioinformatics Institute and University of Cambridge
Keynote: Protecting Infants with Maternal Vaccination
Speaker
Shabir Madhi University Witwatersrand
Prospects of Maternal Vaccination to Protect Young Infants
One of the United Nations’ Sustainable Development Goals is to reduce the global maternal mortality rate and eradicate preventable deaths in newborns and children under five by 2030. “Of all children under the age of five who die, roughly two thirds will in fact die within the first six months of life” explained vaccinologist Shabir Madhi. Hence, shielding newborns can really advance the fight against child mortality. Maternal and neonatal vaccines could prevent lethal infections at this vulnerable stage of life. However, to develop those vaccines, we need to understand the biological causes of early-life mortality.
Unfortunately, the quality of epidemiological and clinical data regarding child mortality is poor. Neonatal and fetal deaths are underreported and under-investigated, particularly in countries with the highest rates of early-life mortality. In low- and middle-income countries, autopsies of children are rare. As a result, our understanding of early-life mortality is still limited.
Top pathogens identified as the cause of death in newborns in a multi-country study conducted by the Child Health and Mortality Prevention Surveillance (CHAMPS) Network.
Madhi and his team are trying to fill this research gap. In a large study, Madhi and his colleagues collected tissue samples and clinical records of deceased children across seven countries in Africa and Southeast Asia. This diagnostic approach was sufficient to establish the chain of factors that may have ultimately caused the deaths of these infants. Madhi and his team also sought to ascertain the biological causes of stillbirth. Together, these studies revealed that infections accounted for about 20% of stillbirths and 54% of newborn deaths. Furthermore, the investigators were able to identify the top pathogens behind those infections, like K. pneumoniae, or E. coli. These findings can help inform the strategic development of maternal vaccines, a promising intervention in the fight against child mortality.
Pat Furlong, Panelist Parent Project Muscular Distrophy
Roman J. Giger University of Michigan School of Medicine
Altered Mother-To-Newborn Transmission of Pioneering Microbiota and Child Health
The human body is host to a large number of microbes, such as bacteria and fungi. This community of microorganisms, or microbiota, occupies the gut, skin, and cavities. It plays a role in essential functions, like the promotion of immune responses and the production of vitamins. So it’s not surprising that changes to the composition of the microbiota are associated with various diseases. In his research, epidemiologist Noel Mueller studies how the gut microbiota affects metabolic health during early development.
The first exposure to these microbes occurs in the birth canal. This mom-to-newborn transfer of microbiota provides the baby with a healthy collection of microorganisms. Mueller and his team have found that babies delivered by cesarean section (CS) have less of these protective microbes. Instead, opportunistic pathogens are more likely to colonize these babies’ microbiota. The proportion of cesarean-delivered babies continues to increase worldwide. As a result, “even if [CS] poses a small relative risk in health outcomes, it can have a large impact at the population level,” Mueller explained.
During “vaginal seeding,” cesarean-delivered babies are inoculated with their mothers’ microbiota.
CS is associated with a higher risk of developing allergies, obesity, and asthma. Lack of exposure to the mother’s microbiota in the birth canal may be at the root of some of these disorders. Mueller and his collaborators investigated a simple intervention called “vaginal seeding,” which consists of inoculating cesarean-delivered babies with their mother’s microbiota. In this “bacterial baptism,” maternal vaginal microbiota is wiped in the neonate’s face, mouth, and body. Preliminary data suggest that vaginal seeding can restore some beneficial microbes that may otherwise be lacking in these babies. A large randomized controlled trial assessing the efficiency and safety of this technique is currently underway.
Antibody Transfer From Mother To Infant: The Physiology of Breast Milk
For Kirsty Le Doare, an expert in pediatric infectious disease, breast milk is like your grandmother’s chicken soup. “It contains all the nutrients that a baby needs to grow and thrive,” she said. In addition, breast milk also protects infants from infections. Hence, breastfed infants are less vulnerable to gastrointestinal and respiratory tract infections than formula-fed infants. However, it is still unclear how breast milk modulates the infant immune response.
Le Doare wants to change that through her research on age-related immune response to infectious diseases. She, along with her team, conducted a study with Gambian mother/infant pairs. They found that IgA antibodies for Group B Streptococcus (GBS) in breast milk reduced the likelihood of GBS colonization days after birth and increased the likelihood of GBS clearance later in life. Interventions like maternal vaccines can harness this form of neonatal protection against pathogens.
After some forms of maternal immunization, antibodies against certain pathogens persist in the breast milk for at least six months, protecting the neonate. Le Doare and her team are using novel culture models to understand how these antibodies fight pathogens. Although breast milk antibodies are a critical protective agent for the neonate, oligosaccharides in breast milk have also been found to lower the risk of infection. For instance, these sugar molecules can act as a decoy for pathogens, which bind to them and stay away from intestinal cells. A better understanding of these mechanisms could be leveraged to develop therapies to protect neonates against invasive diseases.
The Structure of the Human Placenta Enables Humoral and Cellular Immune Defense
According to virologist Lenore Pereira, 1%-3% of infants are infected with Human Cytomegalovirus (HCMV) every year. In about 25% of infected babies, HCMV can cause congenital disorders such as cerebral palsy, microcephaly, and deafness. Mothers that have strong neutralizing antibodies due to prior HCMV infection are less likely to transmit the infection to the baby, and most infants born of seropositive mothers are asymptomatic. However, the immune mechanisms that help prevent infection are not well understood.
HCMV infects the developing baby by crossing the uterine-placental interface and replicating in the placenta. Using ex vivo explants of first-trimester placentas, Pereira and her team have been able to identify the mechanisms of infection as well as the protective potential of some antibodies. Neutralizing antibodies, namely those that target a specific complex of glycoproteins in the surface of HCMV, reduce viral spread, infection, and cell death in early-gestation placentas.
The investigators also demonstrated that, in the maternal component of the placenta, HCMV infection induces an increase in effector-memory T cells. These cells may confer protection to the babies of seropositive mothers. These findings could lead to the development of antibody treatments that restrict HCMV infection and associated pregnancy complications from congenital infection.
Lessons from Current Vaccines & New Targets for Immunization
Speakers
Janet Englund, MD Seattle Children’s Hospital
Stanley Plotkin, MD Vaxconsult LLC, University of Pennsylvania
Ajoke Sobanjo-ter Meulen, MD, MSc Bill & Melinda Gates Foundation
Maternal Vaccines Licensed for Adults: What Can Be Learned from Recent Experiences with Influenza, Pertussis and Tetanus Vaccines
Maternal immunization is not a new strategy, said pediatrician and infectious disease expert, Janet Englund. Englund discussed the history of maternal vaccines, whose popularity has ebbed and flowed throughout the years. As early as 1879, maternal immunization was used to confer protection from smallpox in infants.
For centuries, tetanus toxoid was one of the leading causes of neonatal death. A landmark study in New Guinea demonstrated that maternal immunization with tetanus toxoid protects newborns. As a result, this vaccine has been routinely administered to pregnant women for years. Thanks to this, Englund said, 45 countries have been able to eradicate maternal and neonatal tetanus, a testament to the potential of maternal immunization to fight global epidemics.
In 2012, an outbreak of pertussis was observed in the US and other developed countries, including the UK. In October of that year, the UK introduced the maternal pertussis vaccine, which was associated with a dramatic decrease in the rate of neonatal pertussis. While most health authorities recommend that pregnant women get this vaccine during the third trimester, recent studies have shown that earlier is better; maternal immunization during the second trimester maximizes pertussis antibody transfer to the infant.
Pregnant women, Englund explained, are at a higher risk of severe influenza infections than non-pregnant women. Influenza infection during pregnancy is associated with preterm birth and low birth weight infants. Maternal influenza immunization is safe and it effectively protects the mother and the newborn. However, less than 50% of pregnant mothers in the US get vaccinated. Along with issues of insufficient insurance coverage, “vaccine hesitancy plays a very important role”, Englund lamented.
Human Cytomegalovirus Vaccines
Physician and vaccinologist Stanley Plotkin gave another presentation on cytomegalovirus (CMV). While co-speaker Lenore Pereira focused on the mechanisms of transplacental CMV transmission, Plotkin looked at the factors involved in CMV infection during pregnancy, immunity, and the status of CMV vaccine development status.
Many people, particularly in developing countries, become infected with cytomegalovirus (CMV) at some point in their lives. CMV infection does not cause obvious disease in most healthy individuals. However, in pregnant women, CMV can cross the placenta and infect the fetus. This can lead to congenital disorders such as microcephaly or deafness. CMV infection is also more serious for adults with weakened immune systems.
Plotkin explained that CMV infection during pregnancy usually occurs when mothers are exposed to toddlers carrying the virus. In developing countries, CMV infects most women before they become pregnant, and newborns are less likely to suffer from congenital disorders upon their mothers’ CMV infection. “We think that natural immunity is protective,” said Plotkin. In a pioneering study, his team found that vaccinating kidney transplant recipients with a weak strain of CMV protected them from contracting severe disease.
Candidate vaccines that are currently being developed to combat human cytomegalovirus infection.
One of the most promising vaccine candidates is the glycoprotein-B (gB) with MF59 adjuvant. This vaccine induces a strong antibody response, and these antibodies protect against CMV infection. Other CMV vaccines are also in the research and development phase. As these vaccines become approved and licensed, some of the first populations to be vaccinated will probably be transplant patients, young girls, and women of child-bearing age who have not been previously infected by CMV.
Updates on Group B Streptococcus (GBS) Vaccine Development
Ajoke Sobanjo-ter Meulen, infectious disease and global health expert, shed light on the current state of Group B Streptococcus (GBS) vaccine development. GBS is a pathogen commonly found in the gut or lower vaginal tract. Because it can cause life-threatening infections in pregnant women, newborns, and immunocompromised adults, it is associated with maternal and neonatal morbidity and mortality, preterm births, and stillbirths. Fatality rates due to GBS infection are higher in low- and middle-income countries.
If pregnant women in the US test positive for GBS colonization, they are treated with antibiotic prophylaxis, which significantly reduces disease during the first hours of life. However, a vaccine has a higher protective potential and it would be a much more feasible approach in low- and middle- income countries, where the diagnostic and therapeutic infrastructure required for that kind of treatment may not be available.
Burden of GBS disease around the world and the advantages of maternal GBS immunization over intrapartum antibiotic prophylactic (IAP) treatment
GBS vaccines given to women during pregnancy can significantly reduce maternal GBS colonization and disease, stillbirths and neonatal sepsis, and meningitis. In a modelling study, Sobanjo-ter Meulen and colleagues estimated that, by improving all of these health outcomes, a maternal GBS vaccine could prevent 90,000 infant deaths and 57,000 stillbirths worldwide. Several vaccine candidates are currently being developed. One challenge facing licensure trials is that, due to the low incidence, a sample size of about 40,000-60,000 pregnant women would be required to ascertain the efficacy of a maternal GBS vaccine.
According to Sobanjo-ter Meulen, public oversight and private investment could help overcome these challenges. That kind of partnership has helped advance the GBS6 vaccine, which demonstrated high safety and immunogenicity levels in healthy adults and is currently being evaluated in a phase-II trial in pregnant women in South Africa.
Infant Vaccination and Barriers to Maternal Immunization
Speakers
Barney Graham, MD, PhD National Institute of Allergy and Infectious Diseases (NIAID), NIH
Ruth Karron, MD Johns Hopkins Bloomberg School of Public Health
Approaches to Infant Vaccination for Respiratory Syncytial Virus
The Respiratory Syncytial Virus (RSV) is a common cause of respiratory tract infections. In newborns, RSV infection can lead to severe disease, usually due to obstruction of small airways. One of the key goals in RSV vaccine development, said immunologist and virologist Barney Graham, is to protect children younger than six months of age from RSV infection.
A failed vaccine trial in the 1960s stalled RSV vaccine development. In the study, vaccinated children became more vulnerable to RSV infection and were more likely to experience severe illness than control groups. According to Graham, the field of RSV vaccine development has only regained speed within the last 10-15 years.
Graham’s work in the structure of RSV fusion protein (F) has been critical in recent advances in RSV vaccine development. This glycoprotein on the surface of RSV mediates viral entry into host cells. During cell entry, the structure of F proteins undergoes a conformational change. The prefusion and postfusion forms of F proteins have different properties as vaccine antigens. Graham and his collaborators led a phase-I clinical trial using a stabilized prefusion F protein. In young adults, this vaccine elicited a potent neutralizing activity, and it is currently being tested in phase-II maternal immunization trials.
A similar strategy can be generalized across other virus families, including coronaviruses. In fact, his work in structure-based immunogen design allowed Graham and colleagues to rapidly solve the structure of the new coronavirus and has greatly contributed to the current efforts to develop a candidate vaccine.
Maternal Immunization: Overcoming Barriers to Uptake and Access
Vaccine research and development is not the only obstacle in maternal and neonatal immunization. “In the end, vaccines are only useful if they can be delivered,” said global health expert Ruth Karron, before discussing contextual factors that influence the successful implementation of maternal vaccines.
When it comes to pregnancy-specific vaccines, medical, social, and economic considerations are paramount. These vaccines are usually administered in the context of antenatal care. Without a robust antenatal care system, implementing an effective maternal immunization program can be challenging. For instance, vaccines that can be administered with some flexibility throughout the second or third trimester will be more likely to lead to successful outcomes in cases when pregnant women have limited opportunities to go to the doctor. Also, attitudes surrounding maternal immunization need to be considered. Vaccine hesitancy can be particularly acute when it comes to pregnancy, as some believe it can be harmful for the child or negatively affect fertility in the future. Failing to understand the effects or the burden of a specific disease can also be an obstacle. These issues have to be addressed broadly with all stakeholders, which include the pregnant women but also other community members, healthcare providers, and policymakers.
Factors that influence the successful deployment of pregnancy-specific vaccines. Slide: Ruth Karron.
Karron and her collaborators created ethical guidelines to include the interests of pregnant women and their offspring in the development of vaccines . Some of these guidelines are very relevant in the context of epidemics. As the current COVID-19 pandemic has revealed, pregnant women and their offspring are among the most severely affected by outbreaks. They are more vulnerable to infections, but they are also disproportionately affected by an overburdened health care system. In her work, Karron advocates for the inclusion of women of childbearing age and pregnant women at every stage of vaccine development and deployment.
Immunotherapy, which harnesses the immune system to target and attack cancer cells, has emerged as a revolutionary approach to cancer treatment. Despite its effectiveness for a wide range of cancers, eligibility for treatment is dependent on the patient’s immune system, age, and genetic profile, as well as how advanced the cancer is and whether it has responded to prior treatment. Current research aims to improve treatment strategies and better predict patient outcomes. On May 11-12, 2020, the New York Academy of Sciences hosted the annual Frontiers in Cancer Immunotherapy symposium. Experts in tumor immunology, cancer genetics, and computational biology discussed novel therapeutic targets, tumor evolution, and the mechanisms driving resistance to current treatment. Learn about the latest research advances in cancer immunotherapy in this summary.
Symposium Highlights
Computational neoantigen model predicts cancer patient outcomes.
Combination immunotherapy produces new T cells that extend patient survival.
Personalized cancer vaccines demonstrate therapeutic benefits.
New computational genomics tools provide pediatric cancer insight.
Immune checkpoint inhibitor associated toxicity yields new clinical syndrome.
Macrophage reprogramming can halt metastatic cancer progression.
Immune cell “neighborhoods” are altered during cancer progression.
Multi-specific CAR T cell therapy may reduce immunotherapy resistance.
Speakers
James Allison, PhD MD Anderson Cancer Center
Mikala Egeblad, PhD Cold Spring Harbor Laboratory
Benjamin Greenbaum, PhD Memorial Sloan Kettering Cancer Center
Crystal Mackall, MD Stanford University
Elaine Mardis, PhD Nationwide Children’s Hospital
Garry Nolan, PhD Stanford University
Jeffrey Sosman, PhD Feinberg School of Medicine, Northwestern University
Catherine Wu, MD Dana-Farber Cancer Institute and Harvard Medical School
Benjamin Greenbaum, PhD Memorial Sloan Kettering Cancer Center
Modeling Immune-Mediated Evolution
Benjamin Greenbaum examines immune interactions that contribute to cancer progression. His lab uses statistical physics and computational biology to study the role of neoantigens in tumor evolution. Neoantigens are mutated peptides present on the surface of cancer cells that have the potential to be immunogenic, meaning T cell receptors can recognize them for an immune response. The Greenbaum lab developed a mathematical model to understand the role of neoantigens. “The goal of this framework is to try to quantify the immunogenicity of neoantigens in an evolutionary model to better predict response to therapy,” said Greenbaum.
Mathematical model predicts whether or not a patient is likely to have immunogenic neoantigens.
In this model, the tumor is characterized by the presence of neoantigens that are likely to provoke an immune response as well as the likeliness of that neoantigen progressing in forward evolution. Using this approach, the Greenbaum lab was able to separate patients who responded to treatment versus those who did not for both melanoma and small-cell lung cancer. The team will apply this model to predict patient outcomes in the clinic.
Immune Checkpoint Blockade in Cancer Therapy: Historical Perspective, New Opportunities
A pioneer in the field of cancer immunotherapy, James Allison has devoted his career to studying T cell response regulation and developing strategies for cancer treatment. In 2018, he was awarded the Nobel Prize in Physiology or Medicine jointly with Tasuku Honjo “for their discovery of cancer therapy inhibition of negative immune regulation,” as well as the Dr. Paul Janssen Award for Biomedical Research. One of Allison’s primary research areas is the role of immune checkpoint molecules, which help prevent the immune system from attacking healthy tissue. Early work in the Allison lab found that blocking a major immune checkpoint protein, cytotoxic T-lymphocyte-associated protein 4 (CTLA-4), allows T cells to target and destroy tumors. The FDA approved anti-CTLA-4 therapy, which demonstrated success in clinical trials. The effects have been significant: in metastatic melanoma, a disease with a median survival of seven months, anti-CTLA-4 therapy extended the survival of approximately 20% of patients by ten years after a single round of treatment.
Combination immunotherapy aims to extend the lives of a greater percentage of patients compared to mono-immunotherapies.
However, Allison wondered why this treatment wasn’t successful for all patients. After the discovery of another checkpoint inhibitor protein, programmed cell death protein 1 (PD1), Allison’s lab decided to use mass spectrometry to examine T cell populations before and after anti-CTLA-4 therapy, anti-PD1 therapy, and therapy combining both of these treatments. Although new T cell phenotypes arise following all three treatments, the combination therapy produces a synergistic effect that leads to the greatest increase in particular T cells that help target tumors. “It seems to be this that is responsible for the increase in efficacy, not just the combination of the effects of the monotherapies alone,” said Allison. His future work aims to enhance our understanding of combination checkpoint blockade therapy to extend the lives of more patients.
Catherine Wu, MD Dana-Farber Cancer Institute and Harvard Medical School
Driving T cells into Tumors: A Role for Personal Cancer Vaccines
Catherine Wu works to enable more specific tumor targeting. She explained that one critical challenge is increasing the number of patients—right now, approximately 30%—with lasting responses to immunotherapies. Therapeutic vaccines may provide a solution. Wu said that these vaccines would, “stimulate antigen-specific immunity against determinants that are expressed in the cancer, and in doing so, increase the breadth and diversity of tumor-specific T cells.” Toward this goal, her lab has developed personalized vaccines for patients. The process begins with identifying specific mutations in a patient’s tumor using DNA and RNA sequencing. Next, human leukocyte antigen (HLA) typing is performed, and then personalized HLA-binding peptides are predicted. Excitingly, these vaccines, in combination with checkpoint blockade therapy, have demonstrated success in high-risk melanoma and glioblastoma patients. To improve HLA predictions, her lab has also developed an approach using mass spectrometry to examine antigen processing. To date, they have expanded from 16 to 95 HLA alleles that cover different racial groups such that they have 95% global coverage. This work represents an unprecedented advancement in distinguishing tumor-presenting epitopes.
Immunogenomics and the TME in Pediatric CNS Cancers
Elaine Mardis uses genomics to understand cancer progression and advance immunotherapeutic treatments. Specifically, her work focuses on understanding pediatric cancers. Unlike adult cancers, pediatric cancers have few druggable targets and are generally less well understood. By using and innovating computational approaches to characterize the tumor microenvironment and cancer progression, the Mardis lab provides unprecedented insight into pediatric cancers. For example, patient tumors are analyzed using exome sequencing and RNA sequencing with multiple analyses. Mardis has also developed a platform for neoantigen prediction called pVACtools, which aims to identify neoantigens from genomic fusion breakpoints. This work led to the discovery that recurrent pediatric central nervous system cancers contain immune cells in the tumor microenvironment that have been recruited from the periphery. This likely provides an immune-suppressive context based on checkpoint blockade, but neoantigen alterations may allow for the immune system to be engaged. However, new approaches may be required to extend immunotherapy to pediatric cancers because there are significant differences in the immune system based on age.
Jeffrey Sosman, PhD Feinberg School of Medicine, Northwestern University
Immune Related Toxicities: Mechanisms and Disease Outcome
Jeffrey A. Sosman is an oncologist and cancer immunotherapy researcher studying immunotherapy toxicity. Although cancer immunotherapies have transformed the therapeutic landscape, these treatments have a variety of toxic effects that limit treatment potential. Fairly common toxicities include rashes, joint and tissue diseases, colitis and hepatitis, while more rare toxicities include encephalitis and myocarditis. Dr. Sosman presented a case study on a patient that developed immune checkpoint inhibitor (ICI) associated myocarditis, which he defined as a new clinical syndrome. Immune checkpoint inhibitors prevent natural “brakes” in the immune system so that T cells can attack cancer cells. Although myocarditis is rare in ICI-treated patients (less than 0.1%), this toxicity has a 50% mortality rate. Sosman shared that onset of ICI-associated myocarditis is highly unpredictable, though it can occur early on in treatment. He also noted that patients treated with combinations of immune checkpoint therapies are at higher risk for developing this toxicity. Future work aims to better predict serious toxicity and to understand the relationship between toxicity and tumor response.
Regulation of Cancer Progression by the Tumor Microenvironment
Mikala Egeblad studies the tumor microenvironment in cancer. Her lab has examined the role of bacterially derived lipopolysaccharides (LPS) in cancer progression, which is understood to influence macrophages within the tumor phenotypically. Specifically, the effect of LPS depends on the presence of either pro-inflammatory signals (IFNγ), which create tumoricidal macrophages, or anti-inflammatory signals (IL-4 and -13, TGFβ), which produce tumor-promoting macrophages. However, LPS cannot be used to treat cancer because of its toxicity in humans. Considering a novel therapeutic approach, Egeblad said, “we wanted to see if we could take tumor-promoting macrophages and reprogram them to become tumoricidal.” Their approach involved the use of monophosphoryl lipid A (MPLA), an LPS derivative that is already used as a vaccine adjuvant.
Macrophages can be programmed to become tumoricidal or tumor-promoting.
They hypothesized that if they delivered MPLA and IFNγ to tumors, macrophages would become tumoricidal. The lab observed that tumors from both mice and patients with breast cancer contained anti-tumor macrophages following treatment, which stopped metastatic progression. Egeblad and her team plan to elucidate how long lasting the responses are and whether they can be further improved by combining this treatment with checkpoint blockade immunotherapy.
Garry Nolan has developed multiple technologies to improve our understanding of both normal immune function and immunopathologies. One such tool termed CODEX (CO-Detection by indexing) modifies traditional fluorescent microscopes for high-dimensional imaging so that users can obtain spatial and quantitative insight into cells within complex tissues. As a multiplexed imaging platform, CODEX allows users to stain tissue with 50-120 antibodies that have unique barcodes that can be annealed to fluorophores for visualization. Interestingly, Nolan’s lab has used this technology to identify specific “neighborhoods” of immune cells, defined as tissue regions within each cell that have a similar surrounding of cell types. They have also discovered that cellular neighborhoods communicate with each other and can change during various stages of cancer. This information provides critical insight into disease progression that may inform clinical outcomes in the future.
Next Generation CAR T Cells
Crystal Mackall studies the basis of tumor-immune interactions to develop new cancer immunotherapies. Specifically, her lab works to improve chimeric antigen receptor T cell (CAR T cell) therapy, in which a patient’s T cells are engineered to express a synthetic receptor that recognizes an antigen on their tumor. Despite its effectiveness, some patients become unresponsive to this treatment over time. “As we think about the future of this field, we need to talk about the issue of resistance,” said Mackall, “we need to unpack it and identify where and how these cells are failing.” The loss of specific antigen expression has been identified as a significant contributor to resistance, as it can eliminate the ability of CAR T cells to recognize the tumor.
Challenges such as the loss of antigen expression can lead to immunotherapy resistance.
To address this problem, Mackall’s lab engineered a “multi-specific CAR” to simultaneously target two antigens. Even if one antigen’s expression is lost over time, the other will still be targeted which may reduce resistance. In a clinical trial, she found that this therapeutic strategy was well tolerated in both children and adults with leukemia and lymphoma. Mackall’s lab will further optimize the engineering of other multi-specific CARs to overcome resistance.




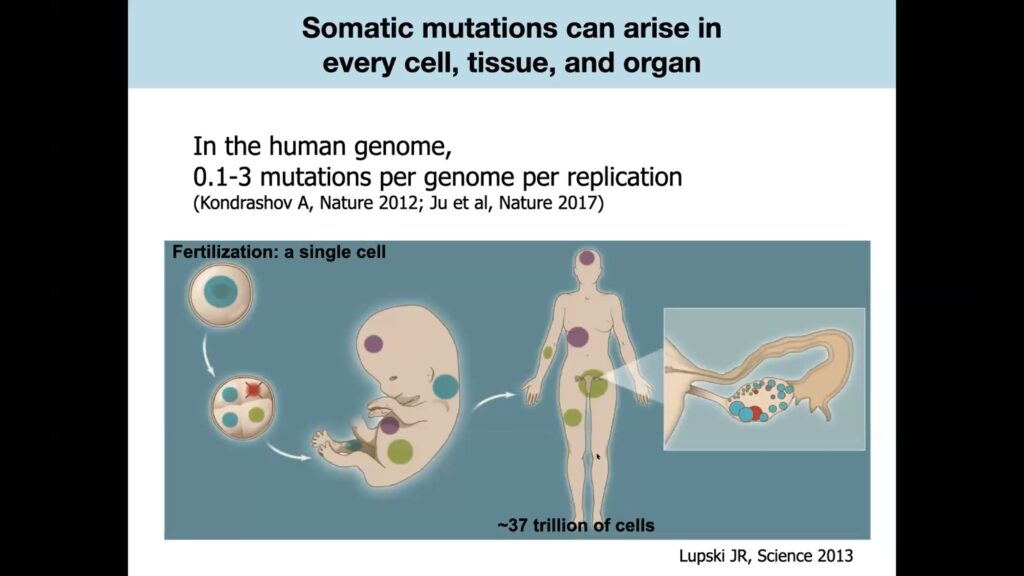
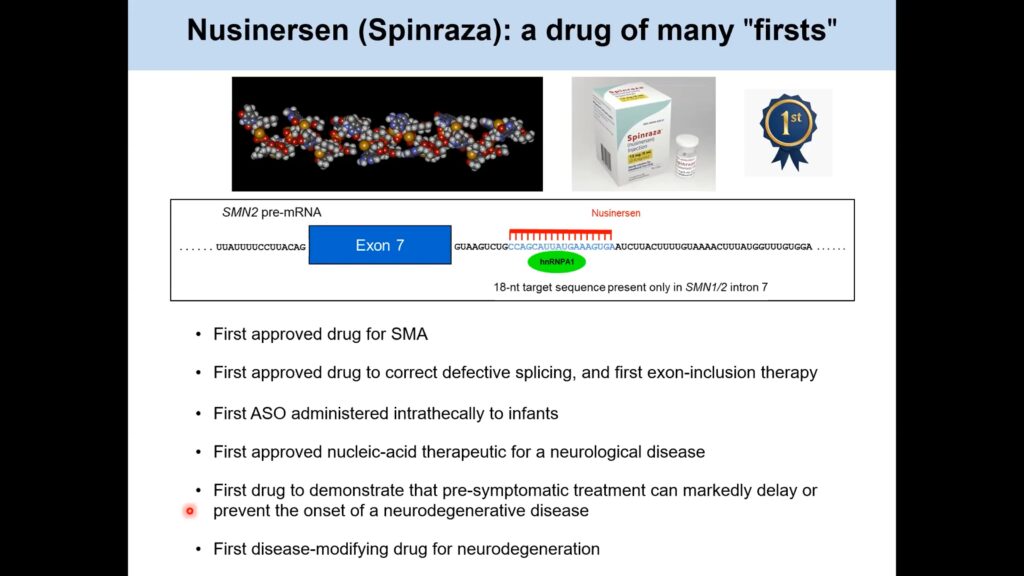
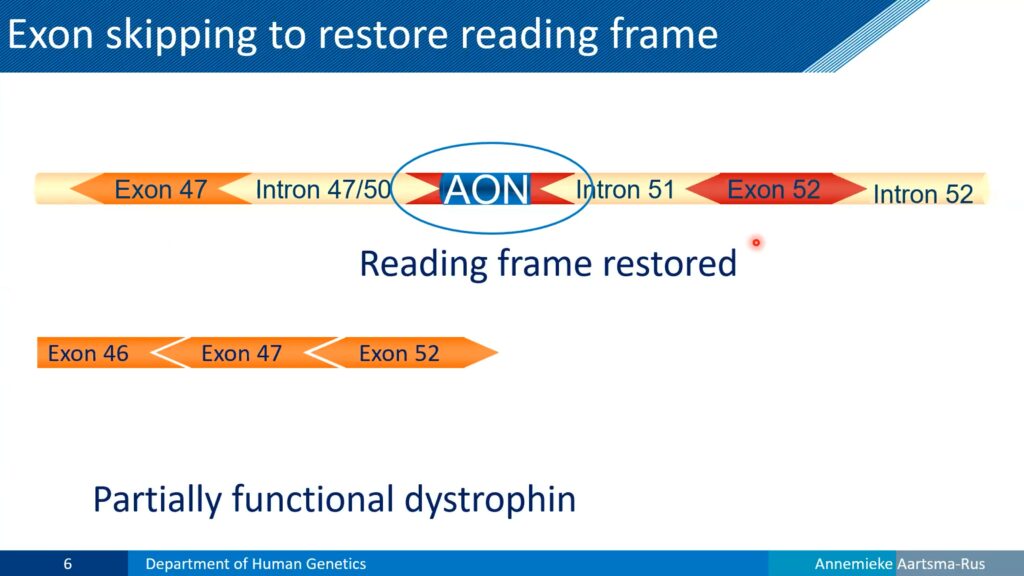
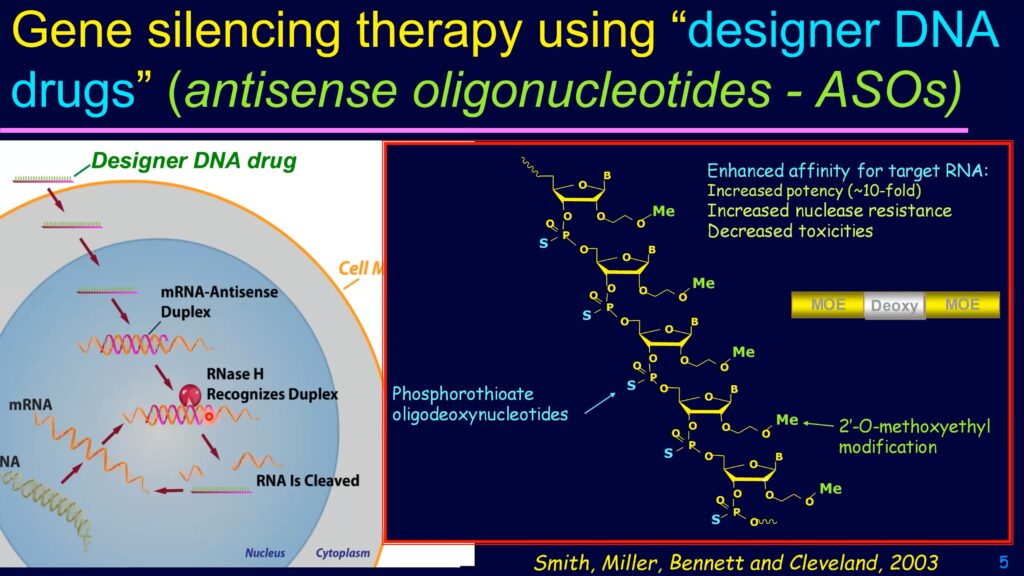
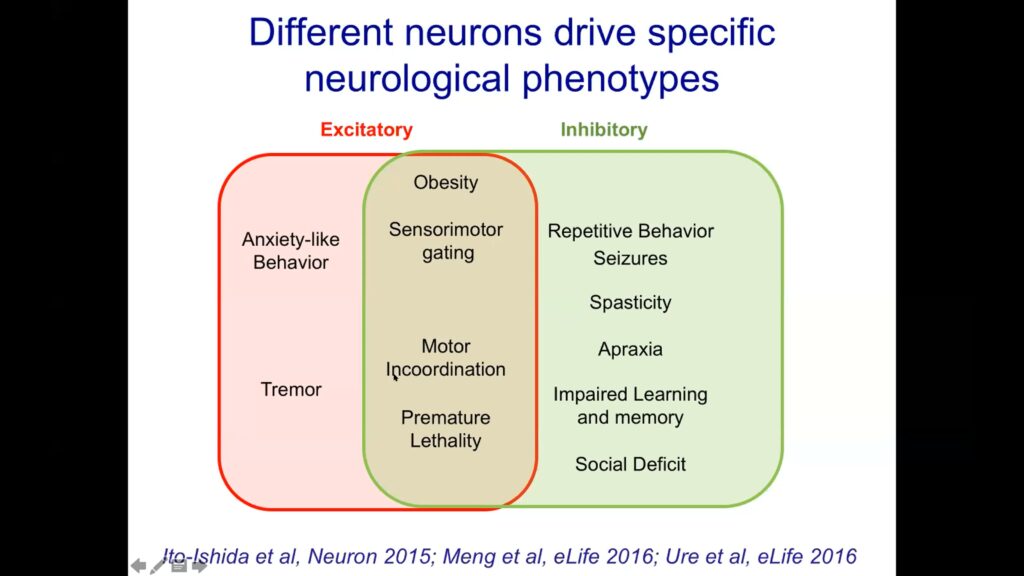



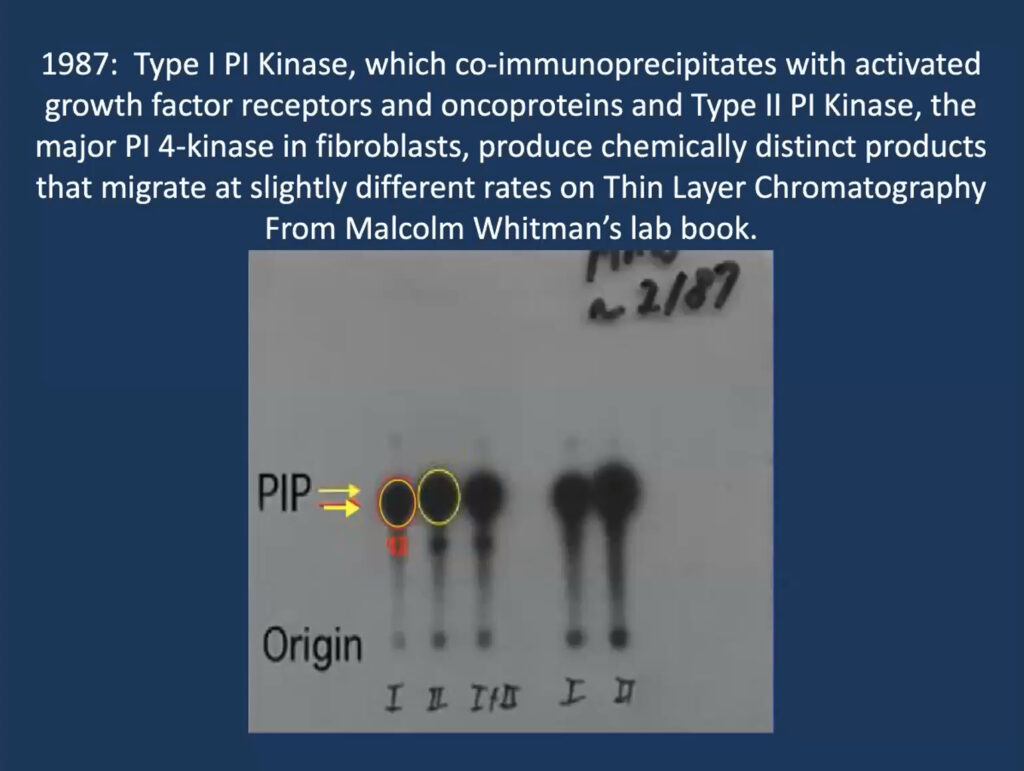
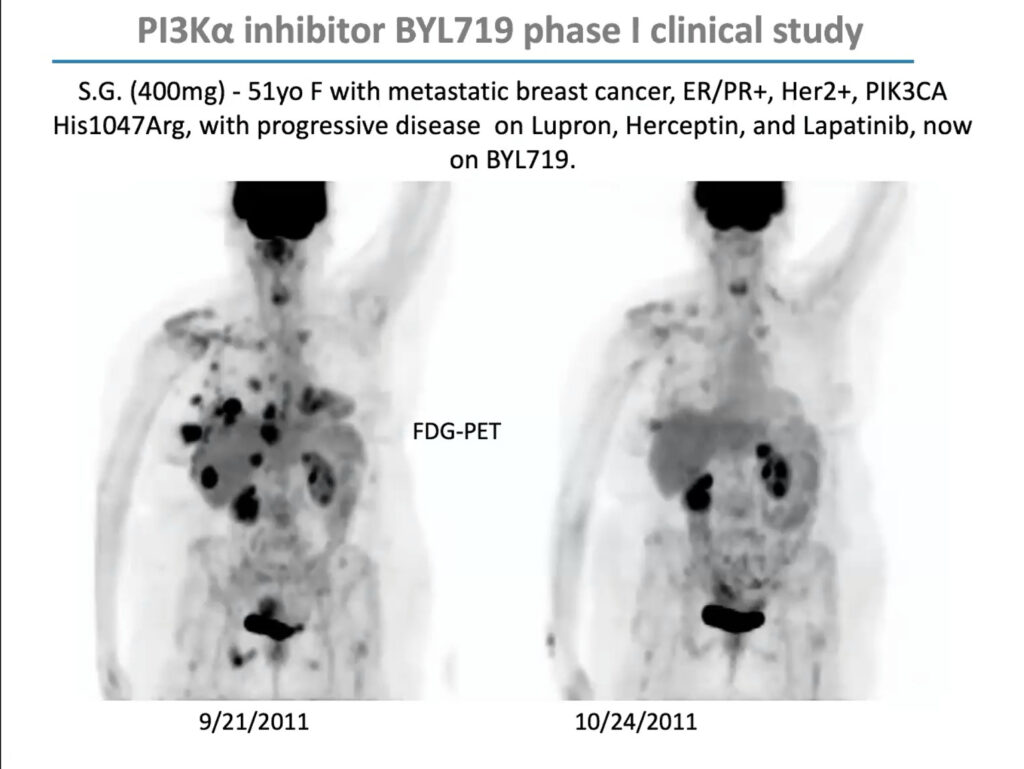
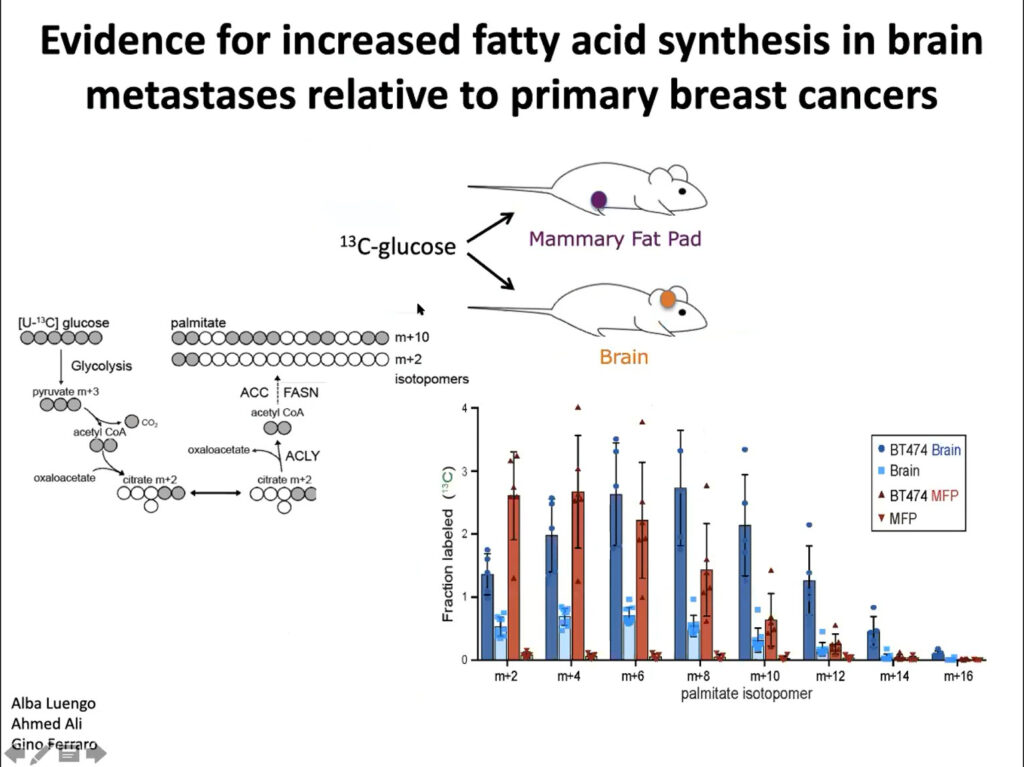
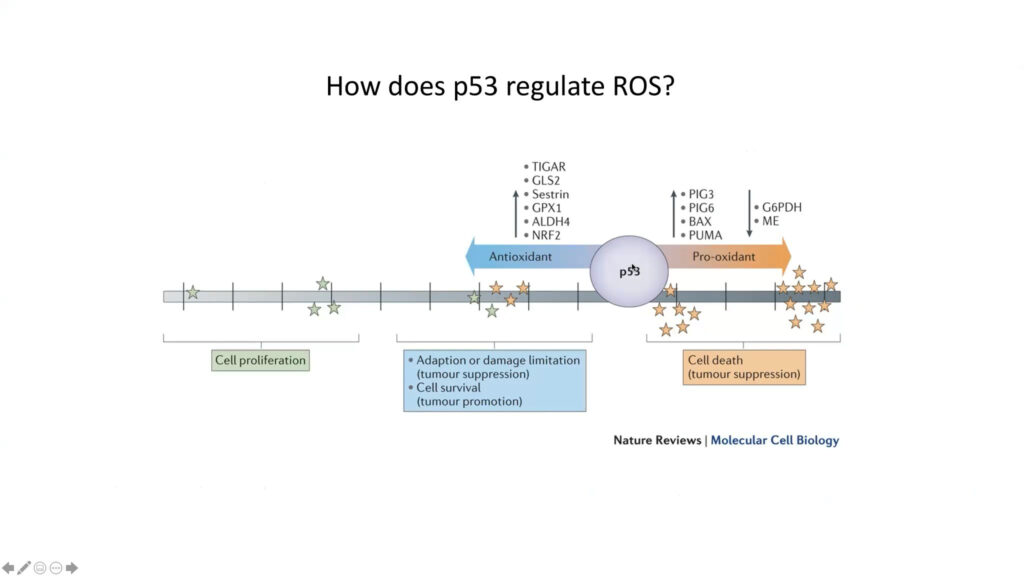
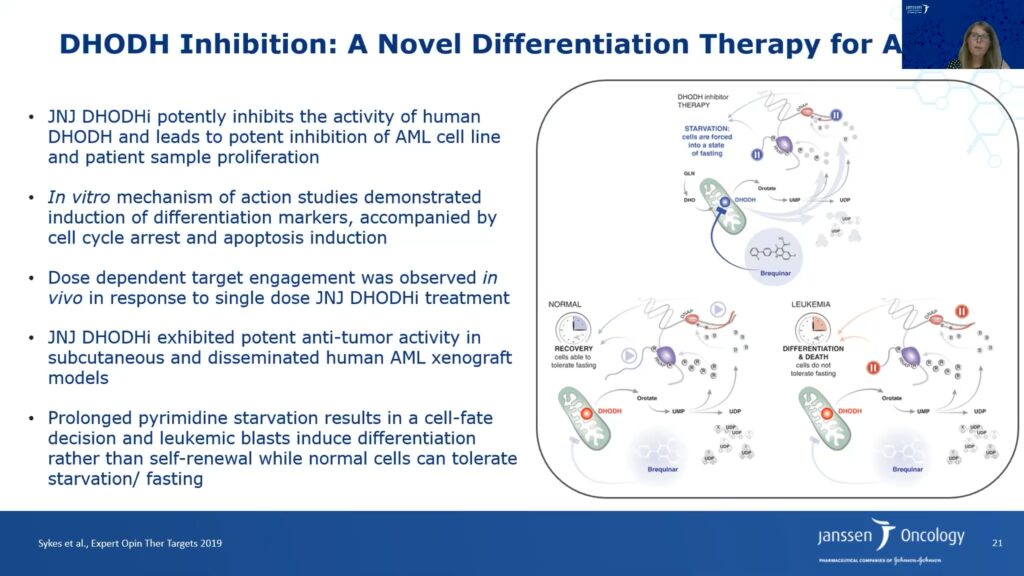
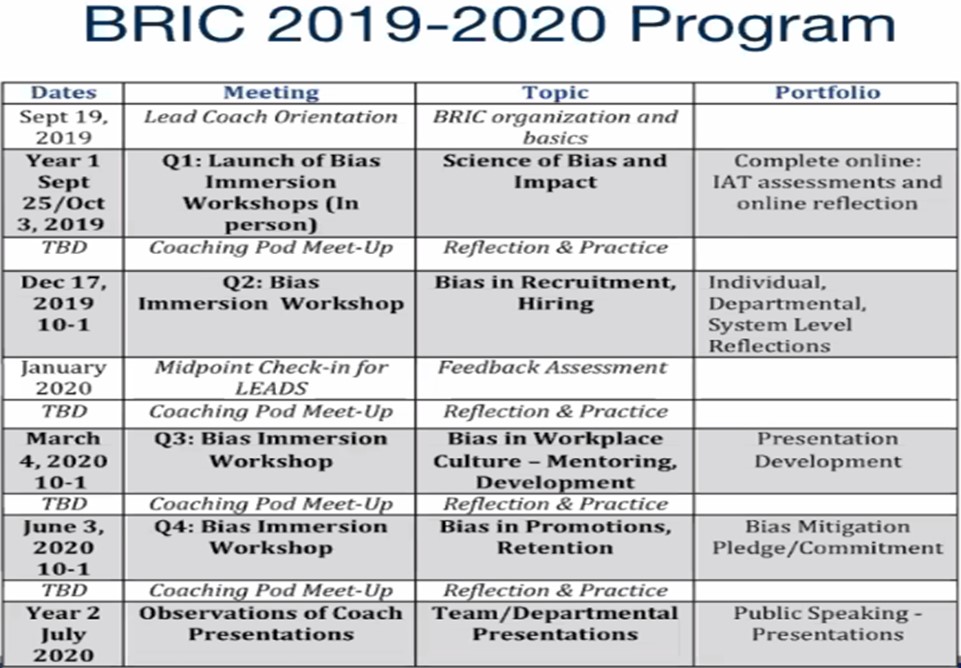







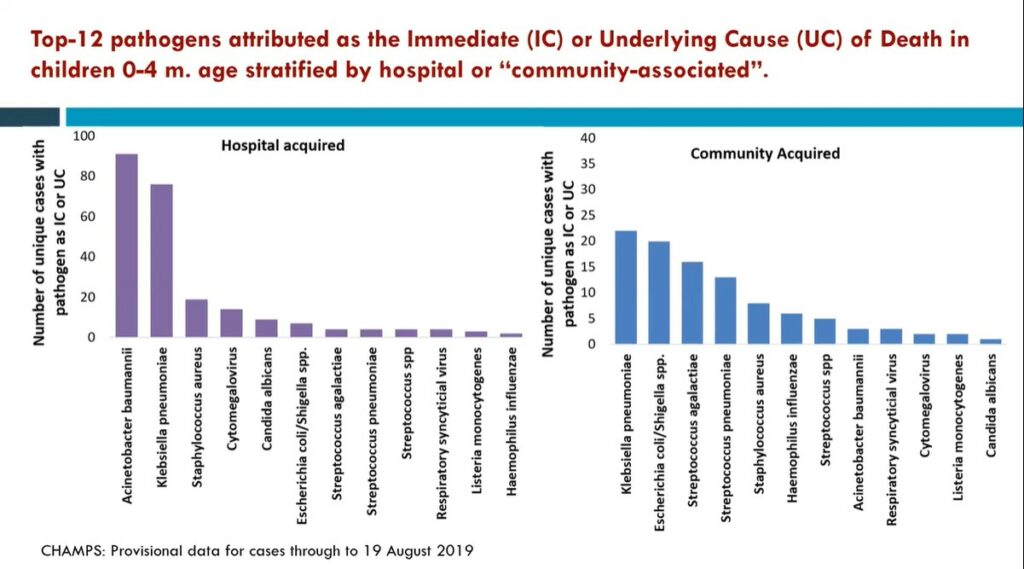
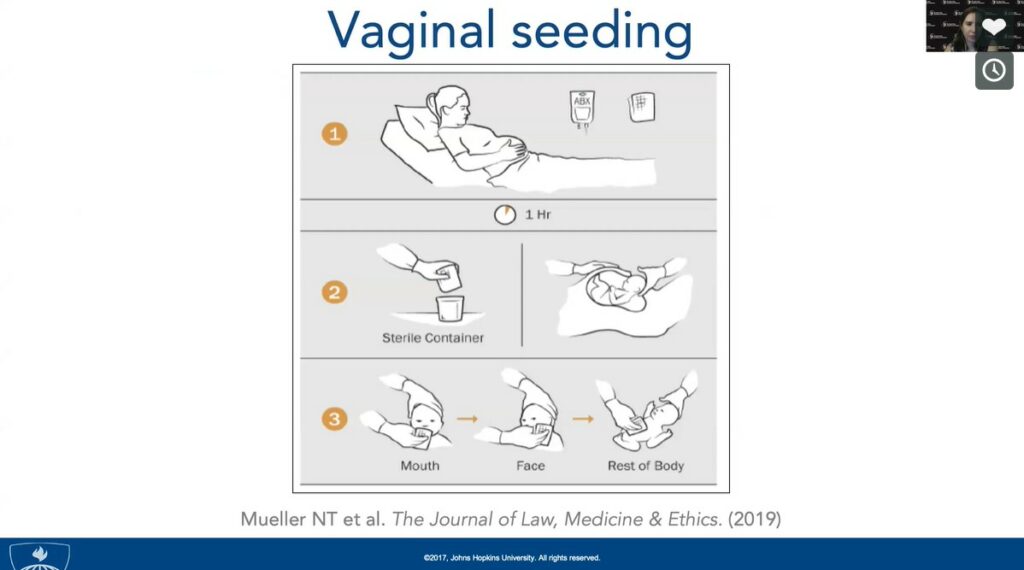
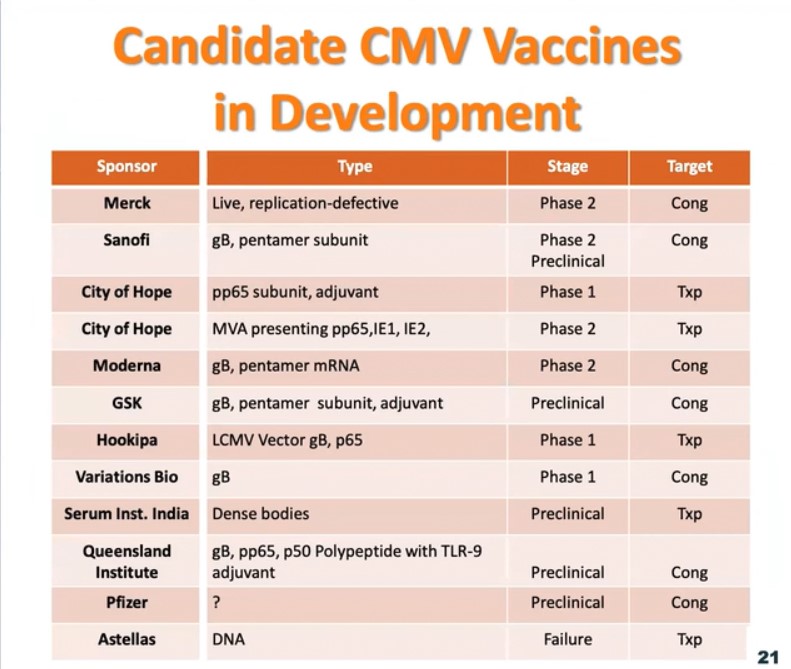
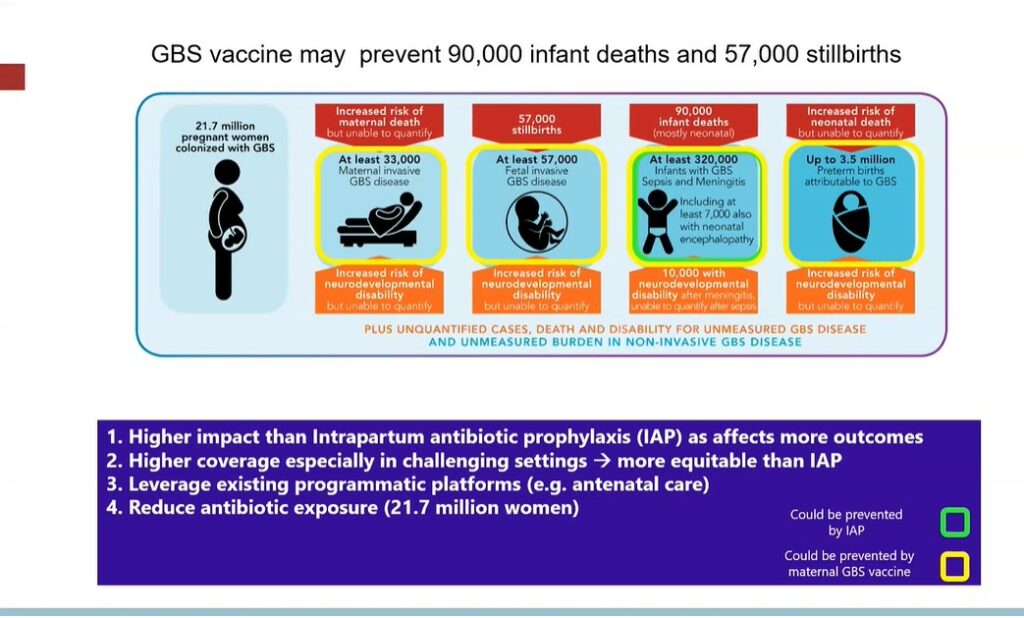
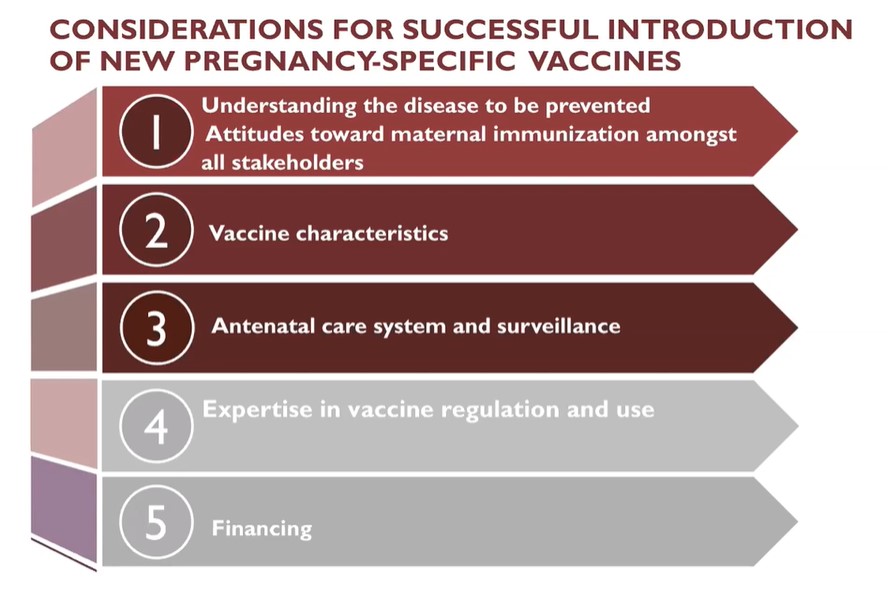
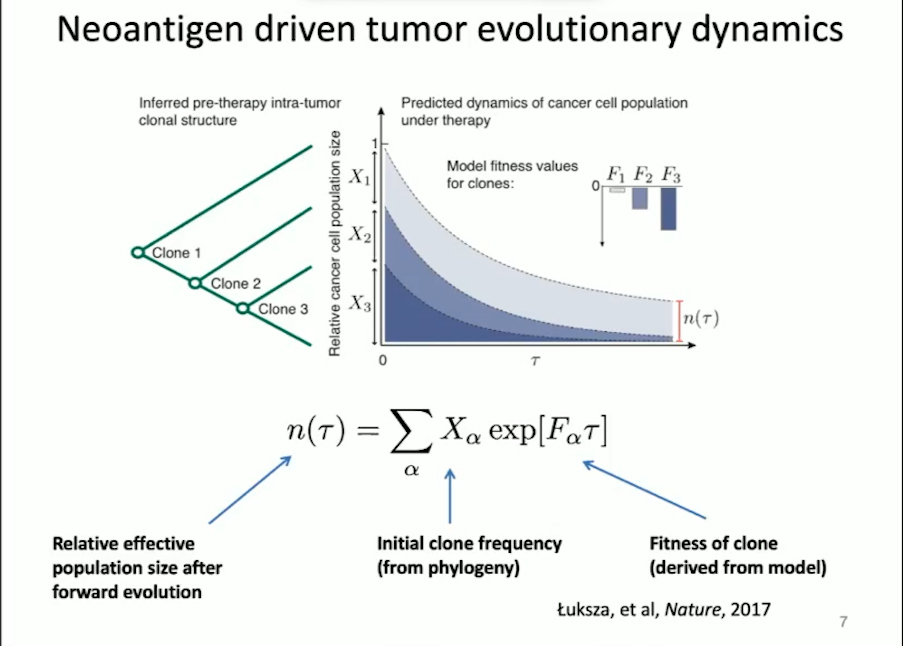
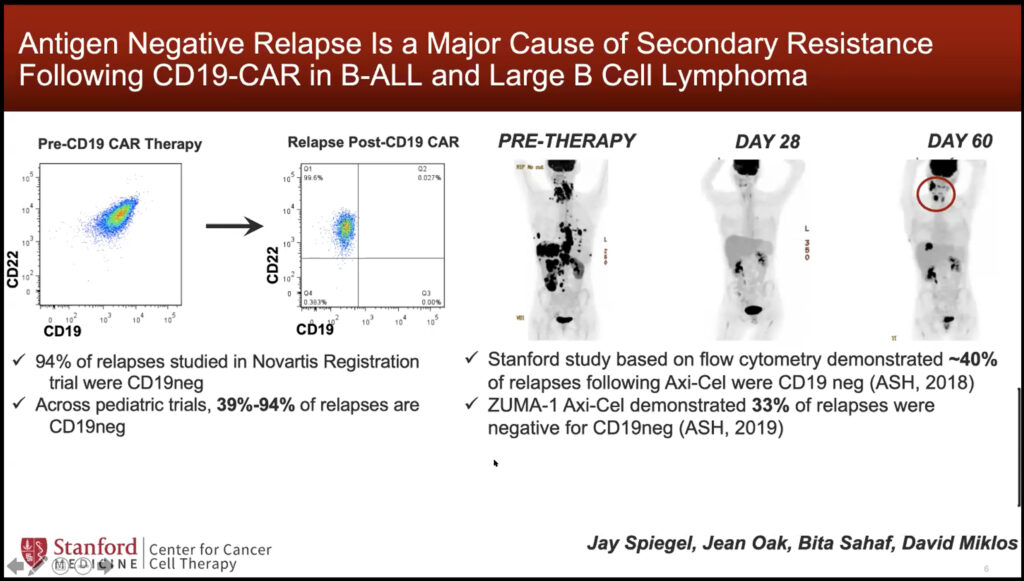
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}