The 2020 Innovators in Science Award winners include a biochemist/molecular geneticist from Cold Spring Harbor Laboratory and brain disorder researcher from the Korea Advance Insitute of Science and Technology.
New York, NY | July 8, 2020 and Osaka, Japan | July 8, 2020 – Takeda Pharmaceutical Company Limited (“Takeda”) (TSE:4502) and the New York Academy of Sciences announced today the Winners of the third annual Innovators in Science Award for their excellence in and commitment to innovative science that has significantly advanced the field of rare disease research. Each Winner receives a prize of US $200,000.
Senior Scientist Award: Adrian R. Krainer
The 2020 Winner of the Senior Scientist Award is Adrian R. Krainer, Ph.D., St. Giles Foundation Professor at Cold Spring Harbor Laboratory. Prof. Krainer is recognized for his outstanding research on the mechanisms and control of RNA splicing, a step in the normal process by which genetic information in DNA is converted into proteins. Prof. Krainer studies splicing defects in patients with spinal muscular atrophy (SMA), a devastating, inherited pediatric neuromuscular disorder caused by loss of motor neurons, resulting in progressive muscle atrophy and eventually, death. Prof. Krainer’s work culminated notably in the development of the first drug to be approved by global regulatory bodies that can delay and even prevent the onset of an inherited neurodegenerative disorder.
“Collectively, rare diseases affect millions of families worldwide, who urgently need and deserve our help. I’m extremely honored to receive this recognition for research that my lab and our collaborators carried out to develop the first approved medicine for SMA,” said Prof. Krainer. “As basic researchers, we are driven by curiosity and get to experience the thrill of discovery; but when the fruits of our research can actually improve patients’ lives, everything else pales in comparison.”
Early-Career Scientist Award: Jeong Ho Lee
The 2020 Winner of the Early-Career Scientist Award is Jeong Ho Lee, M.D., Ph.D, Associate Professor, Korea Advanced Institute of Science and Technology (KAIST). Prof. Lee is recognized for his research investigating genetic mutations in stem cells in the brain that result in rare developmental brain disorders.
He was the first to identify the causes of intractable epilepsies and has identified the genes responsible for several developmental brain disorders, including focal cortical dysplasias, Joubert syndrome—a disorder characterized by an underdevelopment of the brainstem—and hemimegalencephaly, which is the abnormal enlargement of one side of the brain. Prof. Lee also is the Director of the National Creative Research Initiative Center for Brain Somatic Mutations, and Co-founder and Chief Technology Officer of SoVarGen, a biopharmaceutical company aiming to discover novel therapeutics and diagnosis for intractable central nervous system (CNS) diseases caused by low-level somatic mutation.
“It is a great honor to be recognized by a jury of such globally respected scientists whom I greatly admire,” said Prof. Lee. “More importantly, this award validates research into brain somatic mutations as an important area of exploration to help patients suffering from devastating and untreatable neurological disorders.”
The 2020 Innovators in Science Award Ceremony and Symposium
The 2020 Winners will be honored at the virtual Innovators in Science Award Ceremony and Symposium in October 2020. This event provides an opportunity to engage with leading researchers, clinicians and prominent industry stakeholders from around the world about the latest breakthroughs in the scientific understanding and clinical treatment of genetic, nervous system, metabolic, autoimmune and cardiovascular rare diseases.
“At Takeda, patients are our North Star and those with rare diseases are often underserved when it comes to the discovery and development of transformative medicines,” said Andrew Plump, M.D., Ph.D., President, Research & Development at Takeda. “Insights from the ground-breaking research of scientists like Prof. Krainer and Prof. Lee can lead to pioneering approaches and the development of novel medicines that have the potential to change patients’ lives. That’s why we are proud to join with the New York Academy of Sciences to broadly share and champion their work — and hopefully propel this promising science forward.”
“Connecting science with the world to help address some of society’s most pressing challenges is central to our mission,” said Nicholas Dirks, Ph.D., President and CEO, the New York Academy of Sciences. “In this third year of the Innovators in Science Award we are privileged to recognize two scientific leaders working to unlock the power of the genome to bring innovations that address the urgent needs of patients worldwide affected by rare diseases.”
About the Innovators in Science Award
The Innovators in Science Award grants two prizes of US $200,000 each year: one to an Early-Career Scientist and the other to a well-established Senior Scientist who have distinguished themselves for the creative thinking and impact of their research. The Innovators in Science Award is a limited submission competition in which research universities, academic institutions, government or non-profit institutions, or equivalent from around the globe with a well-established record of scientific excellence are invited to nominate their most promising Early-Career Scientists and their most outstanding Senior Scientists working in one of four selected therapeutic fields of neuroscience, gastroenterology, oncology, and regenerative medicine.
Prize Winners are determined by a panel of judges, independently selected by The New York Academy of Sciences, with expertise in these disciplines. The New York Academy of Sciences administers the Award in partnership with Takeda.
For more information please visit the Innovators in Science Award website.
About Takeda Pharmaceutical Company Limited
Takeda Pharmaceutical Company Limited (TSE:4502/NYSE:TAK) is a global, values-based, R&D-driven biopharmaceutical leader headquartered in Japan, committed to bringing Better Health and a Brighter Future to patients by translating science into highly-innovative medicines. Takeda focuses its R&D efforts on four therapeutic areas: Oncology, Rare Diseases, Neuroscience, and Gastroenterology (GI).
We also make targeted R&D investments in Plasma-Derived Therapies and Vaccines. We are focusing on developing highly innovative medicines that contribute to making a difference in people’s lives by advancing the frontier of new treatment options and leveraging our enhanced collaborative R&D engine and capabilities to create a robust, modality-diverse pipeline. Our employees are committed to improving quality of life for patients and to working with our partners in health care in approximately 80 countries. For more information, visit https://www.takeda.com.
On March 5, 2020, the New York Academy of Sciences celebrated the Laureates and Finalists and winners of the 2020 Blavatnik Awards for Young Scientists in the United Kingdom. The one-day symposium featured fast-paced, engaging research updates from nine scientists working in diverse fields within life sciences, chemistry, and physical sciences and engineering. This year’s Blavatnik UK honorees are probing the deepest mysteries ranging from the universe to the human mind, tackling longstanding questions that have occupied scientists and philosophers for millennia. Is there life beyond our Solar system? How is knowledge organized in the brain? What is the fundamental nature of gravity? Find out how this game-changing group of young scientists is working to answer these questions in this summary of the symposium.
Symposium Highlights
Environmental factors can influence the defense strategies bacteria use to fend off invading viruses. Insights into this process are advancing the potential for phage therapy as an alternative to antibiotics.
New analytical and computational tools are revealing the neural machinery that allows the brain to create models of the world and facilitates decision-making and behavior.
Chemists can exploit chirality to create novel molecules with a wide variety of applications in drug design, consumer electronics, and catalysis.
The scientific community is closer now than ever to realizing the commercial potential of nuclear fusion as a source of clean energy.
The first viable theory of massive gravity might help explain some of the biggest mysteries in physics, including the accelerated expansion of the universe.
Hosted By
Victoria Gill Science Correspondent BBC News
Speakers
Tim Behrens, DPhil University of Oxford and University College London
Ian Chapman, PhD UK Atomic Energy Authority
Matthew J. Fuchter, PhD Imperial College London
Stephen M. Goldup, PhD University of Southampton
Kirsty Penkman, PhD University of York
Claudia de Rham, PhD Imperial College London
Eleanor Stride, PhD University of Oxford
Amaury Triaud, PhD University of Birmingham
Edze Westra, PhD University of Exeter
Program Supporter
Changing the Game in Life Sciences
Speakers
Eleanor Stride, PhD University of Oxford
Edze Westra, PhD University of Exeter
Tim Behrens, DPhil University of Oxford & University College London
Engineering Bubbles
Mechanical engineer Eleanor Stride never planned to design drug delivery systems. She was “convinced I wanted to spend my career designing Aston Martins,” until a chance discussion with a supervisor piqued her interest in therapeutic applications of engineered microbubbles. Just two microns in diameter, microbubbles can be used as ultrasound contrast agents, but Stride sees a role for these tiny tools in the fight against cancer. “In many cases, the problem with cancer drugs [is] how we deliver them,” she said, explaining that systemic chemotherapy agents often cannot penetrate far enough into tumors to be effective. These drugs can also cause side effects and damage healthy tissues.
Microbubbles can help sidestep these challenges, safely encapsulating drug molecules within a stabilizing shell. The shell can be functionalized with magnetic nanoparticles, allowing clinicians to direct the bubbles’ aggregation at tumor sites and visualize them with ultrasound. As the bubbles compress and release in response to the ultrasound beam, the oscillation helps the bubbles penetrate into the surrounding tissue. “If we increase the ultrasound energy, we can destroy the bubble, allowing us to release the drugs on demand,” said Stride, noting that molecules released from a single 2-micron microbubble can circulate up to 100 times that diameter, pumping drugs deep into tumor tissues. This approach is highly localized—drugs are only released at the tumor site—which eliminates the potential for systemic toxic effects.
Ultrasound-stimulated oscillation of microbubbles creates a vortex in surrounding fluids. The vortex pumps drug molecules deep into tumor sites.
In 2019, Stride and a team of collaborators published the results of trials using oxygen-loaded magnetic microbubbles to treat malignant pancreatic tumors. In animal models, tumors treated with microbubble-delivered drugs showed dramatic spikes in cell death and also shrank in size, “which can mean the difference between a surgeon being able to remove a tumor or not,” said Stride. Additional experiments have helped hone techniques for external magnetic control of microbubbles within blood vessels to ensure precise, targeted drug delivery—a critical step toward tailoring this method for use in humans. Stride and her collaborators aim to launch a clinical trial in pancreatic cancer patients “in the very near future.”
Insights From Bacteria-Phage Interactions
As the fight against viruses dominates the news cycle, 2020 Blavatnik Awards UK Finalist Edze Westra shared an update from the front lines of a viral war billions of years in duration: the “evolutionary arms race” between bacteria and the viruses that infect them, called phages. The interactions between bacteria and phages—the most abundant biological entities on Earth—have profound implications for the development of phage-based therapies as alternatives to antibiotics.
Phages are often successful killers, but bacteria have evolved sophisticated immune strategies to resist attacks. Understanding how and when bacteria deploy each of these defensive tactics is key to designing phage therapies to treat bacterial infections.
Like humans, bacteria utilize both innate and adaptive immune responses to invading pathogens. In bacteria, innate immunity relies on the modification of surface structures to prevent phages from attaching. This system is effective, yet it creates no “record,” or memory, of which phages it encounters. The adaptive immune system, however, allows bacteria to build a database of previously encountered pathogens in the form of bits of genetic material snipped from invading phages and incorporated into the bacterium’s own DNA. The adaptive immune system, known as CRISPR immunity, forms the basis of CRISPR-Cas genome editing techniques. “There’s a critical balance between these two systems, and both are critical for survival,” said Westra, whose research aims to determine the factors that influence whether a bacterium mounts an innate or adaptive immune defense against a particular phage.
Using Pseudomonas aeruginosa, an antibiotic-resistant pathogen that often infects cystic fibrosis patients, Westra determined that a bacterium’s environment—specifically, the level of available nutrients—determined which defensive strategy was utilized. In high-nutrient environments, almost all bacteria deployed an innate immune response to phage attacks, whereas in lower nutrient settings, CRISPR immunity dominated.
The level of available nutrients influences which immune strategy bacteria use to defend against phage attacks.
In experiments using moth larvae, Westra discovered that infections were more severe when bacteria utilized CRISPR immunity, whereas bacteria that evolved innate immunity often caused less aggressive infections. “If we can manipulate how bacteria evolve resistance to phages, this could potentially revolutionize the way we approach antimicrobial resistance, with major benefits to our healthcare,” Westra said.
Building Models of the World
Computational neuroscientist Timothy Behrens is fascinated with the basic functions and decisions of everyday life—the process of navigating our home or city, the steps involved in completing household tasks, the near-subconscious inferences that inform our understanding of the relationships between people and things. Behrens designs analytical tools to understand how neuronal activity in the brain gives rise to these thought processes and behaviors, and his research is illuminating how knowledge is organized in the brain.
The activities of grid cells and place cells are well understood. By creating spatial maps of the world, grid and place cells allow us to navigate familiar spaces and locate items, such as car keys. Behrens explained that much less is known about how the brain encodes non-spatial, abstract concepts and sequence-based tasks, such as loading, running, and emptying a dishwasher. Over the past several years, Behrens and his collaborators have demonstrated that abstract information is similarly mapped as grid-like codes within the brain. “On some level, all relational structures are the same, and all are handled by the same neural machinery,” he said. This insight helps explain the effects of diseases like Alzheimer’s, which targets grid and place cells first and impacts both spatial and non-spatial knowledge.
Relational information is encoded by the same neural machinery that encodes spatial and navigational maps.
In another line of research, Behrens is probing a phenomenon called replay, during which the brain revisits recent memories as a means to consolidate knowledge about current events and anticipate future ones. Behrens illustrated the concept by showing patterns of neuronal activity as a rat runs around a track, then rests. Even at rest, the rat’s brain displays millisecond-long flashes of neuronal activity that mimic those that take place during running. “He’s not running down the track anymore, but his brain is,” said Behrens. Replay also underlies the human ability to understand a simple story even when it’s told in the wrong order. “Our knowledge of the world tells us…what the correct order is, and replay will rapidly stitch together the events in the correct order.”
Computational tools developed in Behrens’ lab have been shared with thousands of scientists around the globe as they pursue new hypotheses about the neural computations that control cognition and behavior. “It’s an exciting time to be thinking about the brain,” Behrens said.
Exploiting Molecular Shape to Develop Materials and Medicines
Consider the handshake: a greeting so automatic it takes place without thinking. Two right hands extend and naturally lock together, but as Matthew Fuchter explained, that easy connection becomes impossible if one party offers their left hand instead. The fumbling that ensues stems from a type of asymmetry called chirality. Chiral objects, such as hands, are mirror-image forms that cannot be superimposed or overlapped, and when one chiral object interacts with another, their chirality dictates the limits of their interaction. Chirality can be observed throughout nature, from the smallest biological molecules to the structures of skyscrapers.
In organic chemistry, molecular chirality can be exploited to tremendous advantage. Fuchter explained that the shape of molecules “is not only critical for their molecular properties, but also for how they interact with their environment.” By controlling subtle aspects of molecular shape, Fuchter is pioneering new strategies in drug design and devising solutions to technological problems that plague common electronic devices.
The notion of pairing complementary molecular geometries to achieve a specific effect is not unique to drug design—such synchronicities can be found throughout nature, including in the “lock and key” structure of enzymes and their substrates. Fuchter’s work aims to invent new drug molecules with geometries perfectly suited to bind to specific biological targets, including those implicated in diseases such as malaria and cancer.
Only one of these two chiral molecules has the correct orientation, or “handedness” to bind to the receptor site on the target protein.
Fuchter is also exploring applications for chirality in a field where the concept is less prominent—consumer electronics. Organic LED, or OLED, technology has “revolutionized the display industry,” allowing manufacturers to create ultra-thin, foldable screens for smartphones and other displays. Yet these features come at a steep efficiency cost—more than half of the light generated by OLED pixels is blocked by anti-glare filters added to the screens to minimize reflectiveness. A novel solution, in the form of chiral molecules bound to non-chiral OLED-optimized polymers, induces a chiral state of light called circularly polarized light. These circularly polarized, chiral light molecules are capable of bypassing the anti-glare filter on OLED screens. Fuchter noted that displays are far from the only technology that stands to be impacted by the introduction of chiral molecules. “Our research is generating new opportunities for chiral molecules to control electron transport and electron spin, which could lead to new approaches in data storage,” he said.
Making Use of the Mechanical Bond
Most molecules are bound by chemical bonds—strong, glue-like connections that maintain the integrity of molecules, which can be both simple, such as hydrogen, and highly complex, such as DNA. 2020 Blavatnik Awards UK Finalist Stephen Goldup’s work focuses on a less familiar bond. Mechanical bonds join molecules in a manner akin to an interconnected chain of links—the components retain movement, yet cannot separate.
Mechanically interlocked molecules have the potential to yield materials with “exciting properties,” according to Goldup, but in the decades since they were first synthesized, they have largely been regarded as “molecular curiosities.” Goldup’s lab is working to push these molecules beyond the laboratory bench by characterizing the properties of interlocked molecules and probing their potential applications in unprecedented ways. His work focuses on two types of mechanically bound molecules—catenanes, in which components are linked together like a chain, and rotaxanes, which consist of a ring component threaded through a dumbbell-shaped axle.
Goldup’s lab has taken cues from nature to introduce additional elements into rotaxanes, resulting in novel molecules with a variety of potential applications. For example, much as enzymes contain “pockets” within which small molecules can bind, rotaxanes too contain a space that can trap a molecule or ion of interest. Rotaxanes that bind metal ions have unique magnetic and electronic properties that could be used in memory storage devices or medical imaging. Inspired by proteins and enzymes that bind DNA, Goldup’s lab has also designed rotaxanes in which DNA itself is the “axle.” In theory, these molecules can be used to effectively “hide” portions of DNA and alter its biological behavior.
Just as enzymes bind small molecules with their structures, rotaxanes can bind molecules in the cavity between the ring and the axle.
Perhaps most significantly, Goldup’s lab has solved a longstanding obstacle to studying rotaxanes: the difficulty of making them. The problem lies in the fact that rotaxanes can be chiral even when their components are not, making it extremely challenging to synthesize a distinct “hand,” or version, of the molecule. Recalling Matthew Fuchter’s example of how an awkward left-hand/right-hand handshake differentiates the “handedness” of two chiral objects, Goldup explained how his lab developed a technique for synthesizing distinctly “left” or “right” handed rotaxanes by utilizing a chiral axle to build the molecules. “Our insight was that by making the axle portion chiral on its own, when we thread the axle into the ring, the rotaxanes we make are no longer mirror-images of each other. They have different properties, and they can now be separated,” he said. Once separate, the chiral portion of the axle can be chemically removed and replaced with other functional groups.
Goldup’s lab is conducting experiments with new mechanically-locked molecules—including chiral rotaxane catalysts— to determine where they may outperform existing catalysts.
Amino Acids as a Portal to the Past
Scientists have multiple methods for peering into the history of Earth’s climate, including sampling marine sediment and ice cores that encapsulate environmental conditions stretching back millions of years. “But this is an incomplete picture—akin to a musical beat with no notes,” said Kirsty Penkman, the 2020 Blavatnik Awards UK Laureate in Chemistry. The records of life on land—fossil records—provide “the notes to our tune, and if we know the timing, that gives us the whole melody,” she said. Archaeologists, paleontologists, and climate scientists can harmonize fossil records with climate history to understand the past, yet their efforts stall with fossils older than 50,000 years—the limit of radiocarbon dating.
Penkman’s lab is developing dating methods for organic remains that reach far deeper into the history of life on Earth. Their strategy relies not on the decay of carbon, but the conversion of amino acid molecules from one form to another. Continuing the theme of chirality from previous presentations, Penkman explained that amino acids exist in two mirror-image forms. However, the body only synthesizes amino acids in the “left-handed,” or L-form. This disequilibrium shifts after death, when a portion of L-amino acids begins a slow, predictable conversion to the right-handed, or D-form. The older the fossil, the greater the balance between D and L isomers. This conversion process, called racemization, was first proposed as a dating method in the 1960s. Yet, it became clear that some of the fossil amino acids were vulnerable to environmental factors that impact the racemization rate, and therefore the date.
About 15 years ago, Penkman discovered that minute stores of proteins within the remains of snail shells are entrapped in intracrystalline voids. These tiny time capsules are unaffected by environmental factors. Studies have since confirmed that shells found in older horizons, for example deeper underground, contain higher ratios of D-amino acids versus those found at younger sites, thus validating the technique.
Calcitic snail shells found at older horizons have higher ratios of D-amino acids than those found at younger horizons.
Snail shells are often found in archeological sites, a serendipity that has led to astonishing findings about early human migration. Shells found alongside several Paleolithic tools “dated as far back as 700,000 years,” according to Penkman. “We’ve successfully shown that early humans were living in Northern Europe 200,000 years earlier than previously believed,” she said.
Penkman’s team has analyzed remains of ostrich eggshells at some of the earliest human sites in Africa, discovering fully preserved, stable sequences of proteins in shells dating back 3.8 million years. Mammalian remains are the next frontier for Penkman’s lab. They have analyzed amino acids in ancient tooth enamel—including that of a 1.7-million-year-old rhinoceros—and are developing microfluidic techniques to sample enamel from early human remains.
Changing the Game in Physical Sciences and Engineering
Speakers
Amaury Triaud University of Birmingham
Ian Chapman UK Atomic Energy Authority and Culham Centre for Fusion Energy
Claudia de Rham Imperial College London
Worlds Beyond Our Solar System
For millennia, humans have wondered whether life exists beyond our planet. Amaury Triaud, 2020 Blavatnik Awards UK Finalist believes we are closer to answering that question now than at any other time in history. The study of exoplanets—planets that orbit stars other than the Sun—offers what Triaud believes is “the best hope for finding out how often genesis happens, and under what conditions.”
The search for exoplanets has revealed remarkable variety among stars and planets in our galaxy. “The universe is far more surprising and diverse than we anticipated,” said Triaud. Astronomers have identified thousands of exoplanets since 1995, and now estimate that there are more planets in the Milky Way than stars—”something we had no idea about ten years ago,” Triaud said. Many exoplanets orbit stars so much smaller than the Sun that these stars cannot be seen with the naked eye. Yet these comparatively small stars provide “optimal conditions” for exoplanet hunters.
Exoplanets are often detected using the transit method—as an orbiting planet passes in front of a star, its shadow temporarily dims the star’s brightness. The larger the planet relative to the star, the greater its impact on the brightness curve and the easier for astronomers to detect. While monitoring a small star 39 light-years from Earth, TRAPPIST-1, a team of astronomers, including Triaud, discovered an exoplanet system comprised of seven rocky planets similar in size to Earth, Venus, and Mercury.
“The next question is to find out whether biology is happening out there,” said Triaud, joking that the biology of interest is not little green men, but rather green algae or microbes similar to the ones that fill our atmosphere with oxygen. The presence of oxygen “acts like a beacon through space, broadcasting that here on Earth, there is life,” said Triaud, explaining that the only way to gauge the presence of life on exoplanets is through atmospheric analysis. Using transmission spectroscopy, Triaud and other astronomers will look for exoplanets that possess an atmosphere and chemical signatures of life, such as oxygen, ozone, or methane, in the atmospheric composition of exoplanets.
Measurements of spectral signatures in a planet’s atmosphere can reveal the presence of gases associated with life, including oxygen and methane.
Such analyses will begin with the launch of the James Webb telescope in 2021. In the meantime, a land-based mission called Speculoos, based partially in Chile’s Atacama desert, is monitoring 1,400 stars in search of additional exoplanets. “It’s rather poetic that from one of the most inhospitable places on Earth, we are on the path to investigating habitability and the presence of life in the cosmos,” Triaud said.
The Path to Delivering Fusion Power
“There’s an old joke that nuclear fusion is 30 years away and somehow always will be,” said 2020 Blavatnik Awards UK Finalist Ian Chapman, but he insists that the joke will end soon. According to Chapman, the “ultimate energy source” is entering the realm of reality. “We’re now in the delivery era, where fusion lives up to its potential,” he said. Low-carbon, low-waste, capable of producing tremendous amounts of energy from an unlimited fuel source—seawater—and far safer than nuclear fission, fusion power has a long list of desirable qualities. Chapman is the first to acknowledge that fusion is “really hard,” but his work is helping to ease the challenges and bring a future of fusion into focus.
Nuclear fusion relies on the collision of two atoms—deuterium, or “heavy” hydrogen, and tritium, an even heavier isotope of hydrogen. Inside the Sun, these atoms collide and fuse, producing the heat and energy that powers the star. Replicating that process on Earth requires enough energy to heat the fuel. of deutrium and tritium gases to temperatures ten times hotter than the Sun, a feat that Chapman admits “sounds bonkers, but we do it every day.”
Within fusion reactors called tokamaks, this superhot fuel is trapped between arrays of powerful magnets that “levitate” the jet as it spins around a central magnetic core, preventing the fuel from melting reactor walls. Yet this is an imperfect process, explained Chapman, and due to fuel instabilities, eruptions akin to “throwing a hand grenade into the bottom of the machine” happen as often as once per second. Chapman devised a method based on his numerical calculations for preventing these eruptions using additional magnet arrays that induce three-dimensional perturbations, or “lobes” at the edge of the plasma stream. Just as a propped-open lid on a pot of boiling water allows steam to escape, these lobes provide a path to release excess pressure.
An array of magnets near the plasma edge creates perturbations in the fuel stream, allowing pressure to escape safely.
Chapman’s technique has been incorporated into the “the biggest scientific experiment ever undertaken by humankind”—a massive tokamak called ITER, roughly the size of a football stadium and equipped with a central magnet strong enough to lift an aircraft carrier. Scheduled to begin producing power in 2025, ITER aims to demonstrate the commercial viability of nuclear fusion. “We can put 50 megawatts of power into the machine, and it produces 500 megawatts of power out,” said Chapman. “That’s enough to power a medium-sized city for a day.”
Even before ITER’s completion, Chapman and others are setting their sights on designing less expensive fusion devices. Late last year, the UK committed to building a compact tokamak that offers the benefits of fusion with a smaller footprint, and Chapman is the leader of this project.
The Nature of Gravity
Claudia de Rham, the 2020 Blavatnik Awards UK Laureate in Physical Sciences and Engineering, concluded the day’s research presentations with an exploration of nothing less than “the biggest mystery in physics today.” For decades, cosmologists and physicists have grappled with discrepancies between observations about the universe—for example, its accelerated expansion— and Einstein’s general theory of relativity, which dictates that gravity should gradually slow that expansion. “The universe is behaving in unexpected ways,” said de Rham, whose efforts to resolve this question stand to profoundly impact all areas of physics.
Understanding the fundamental nature of gravity is key to understanding the origin and evolution of the universe. As de Rham explained, gravity can be detected in the form of gravitational waves, which are produced when two black holes or neutron stars rotate around each other, perturbing the fabric of spacetime and sending rippling waves outward like a stone tossed into a pond. But gravity can also be represented as a fundamental particle, the graviton, similar to the way light can be considered as a particle, the photon, or an electromagnetic wave. Unlike the other fundamental particles such as the photon, the electron, the neutrino, or even the famously elusive Higgs boson, the graviton has never been observed. In theory, the graviton would, like all fundamental particles, exist even in a perfect vacuum, a phenomenon known as vacuum quantum fluctuation. Unknown in Einstein’s day, vacuum quantum fluctuations, when factored into the general theory of relativity, do predict an accelerated expansion of the universe. “That’s the good news,” said de Rham. “The bad news is that the predicted rate of expansion is too fast by at least 28 orders of magnitude.”
This raises the possibility that “general relativity may not be the correct description of gravity on large cosmological scales,” said de Rham. If the graviton had mass, however, it would impact the behavior of gravity on the largest scales and could explain the observed rate of expansion.
Signal patterns from gravitational wave events can serve as models for estimating the mass of the graviton. By comparing the expected signals produced by either a massless particle or a high-mass particle with actual signal patterns from detected events, physicists can place an upper and lower boundary on the graviton’s potential mass.
The idea of a massive graviton has been considered—and refuted—by physicists as far back as the 1930s. Several years ago, de Rham, along with collaborators Andrew Tolley and Gregory Gabadadze, “realized a loophole that had evaded the whole community.” Together, they derived the first theory of massive gravity. “Through gravity, we can now connect small vacuum fluctuations with the acceleration of the universe, linking the infinitely small with the infinitely large,” de Rham said.
Determining the mass of the graviton requires the most precise scale imaginable, and de Rham believes that gravitational wave observatories are perfectly suited to the task. Whether her theory will hold up in future tests remains to be seen, but when it comes to solving this epic mystery, “the possibility is now open.”
Several Laureates and Finalists of the 2020 Blavatnik Awards in the UK joined BBC science reporter Victoria Gill for the final session of the day, a wide-ranging panel discussion that touched on issues both current and future-looking.
Two themes—fear and opportunity— emerged as powerful forces shaping science and society, especially as it relates to climate change and the threat of emerging infectious disease. Gill noted that climate change is “the biggest challenge ever to face humanity,” and that many efforts to raise awareness of its impacts focus on bleak projections for the future. Asked for insights on shifting the tone of climate change communications, Kirsty Penkman acknowledged that “there needs to be a certain level of fear to get people’s attention.” She then advocated for a solutions-oriented plan rooted in the fast pace of scientific progress in clean energy, among other areas. “This is an amazing opportunity,” she said. “Humans are ingenious….in the last 120 years we’ve moved from a horse-drawn economy to a carbon-based economy, and in 5 or 20 years we could be in a fusion-based economy. We have the potential to open up a whole new world.” Eleanor Stride suggested combatting complacency by emphasizing the power of small changes in mitigating the impact of climate change. “One billion people making a tiny change has a huge impact,” she said.
The specter of a coronavirus pandemic had not yet become a reality at the time of the symposium. But Edze Westra presciently detailed the challenges of containing a highly contagious emerging pathogen in a “tightly connected world.” He commented that detecting and containing emerging diseases hinges on the development of new diagnostics, and that preventing future outbreaks will require cultural shifts to limit high-risk interactions with wildlife. For zoonotic diseases such as the novel coronavirus, “it’s all about opportunity,” Westra said.
Panelists also looked to the future of science, touching on issues of equality, discrimination, and diversity, and emphasizing the importance of raising the bar for science education. Stride noted that children are natural scientists, gravitating toward problem-solving and puzzles regardless of nationality or gender. “But something happens later,” she said, lamenting the drop in interest in science as children progress in school. “One of the things that gets lost is that creativity, which is what science really is—we’re coming up with a guess and trying to gather evidence for it—we’re not just learning a huge number of facts and regurgitating them,” she said.
In the wake of Brexit, panelists expressed concern about potential difficulties in attracting international students to their labs. “Diversity is so important,” said Penkman. “Getting ideas from all around the world from people with different backgrounds is essential to making science in the UK—and the world—the best it can be.” In her closing comments, Penkman said that ultimately, the trajectory of science comes down to the people in the field. “My eternal optimism is in the people I work with and the people I talk to when I visit schools—it’s that innate interest and curiosity. Whenever I see it, I feel that is the future of science,” she said.
Researchers are coming up with creative new ways to make plant-based meat alternatives more appealing to consumers, but what will it take for the public to embrace this seemingly unknown food source?
Vegetarianism and even veganism are not new ideas — in fact one of the first mentions of vegetarianism comes from Pythagoras in 500 BCE. Buddhists and other religious groups have long advocated the practice for humane reasons.
The term vegan was coined more recently in 1944, to distinguish those who do not eat any animal-derived products from those who still consume dairy and eggs. Veganism has long been viewed as an extreme lifestyle choice, however, in recent years, the popularity of plant-based diets has been on the rise.
In 2017, six percent of U.S. consumers identified as vegan. While this is still a tiny percentage of the population, it represents a 600 percent increase over the previous three years.
People may choose not to eat meat due to health reasons or concern over animal welfare, but growing awareness of the contribution of food production to climate change has begun to expand the conversation around the need for the broader adoption of a plant-based diet.
According to the Food and Agriculture Organization of the United Nations, food production is responsible for 14.5 percent of worldwide greenhouse gas emissions. It is estimated that if everyone in the U.S. were to give up eating meat and dairy, it would reduce the country’s carbon emissions by 70 percent.
Reducing the prevalence of meat and animal products in the American diet will not be easy, as ideas and preferences about food are deeply rooted in cultural and societal norms. Even with greater understanding of the health and environmental implications, many people struggle with the idea of replacing their Thanksgiving turkey, or their celebratory steak, with a plant-based alternative.
Meat Diets Associated with Higher Standards of Living
Eating meat is also associated with increasing wealth, and as the standard of living has increased over the last 50 years in countries such as China, so too has their meat consumption, despite government policies advocating for lower intake.
A number of new plant-based meat alternatives have recently been developed that aim to ease the transition for those who want to make the switch. Several of these products have garnered significant media attention, but why all the hype? What makes the Impossible Burger “impossible?” and why would you want to go “Beyond Meat”?
While they take different approaches, companies such as Impossible Foods and Beyond Meat aim to create plant-based products that are almost indistinguishable from the real thing, which they believe will lure even the most die-hard meat eaters away from animal-derived products.
According to Principal Scientist, Dr. Laura Kliman, of Impossible Foods, “You can’t just tell people to stop eating meat, so at Impossible we’re not redesigning the product. We’re just redesigning the process to make it, and we’re delivering all the deliciousness, the nutrition, the versatility, that people expect out of meat but we’re making it from plants, which is inherently more sustainable.”
Impossible has a lofty mission to “replace the need for animal farming by the year 2035”. To do that, they take a rigorous scientific approach to replicate the taste and texture of meat. As Kliman says “taste is only a small part of it, flavor is mostly aroma.” In order to identify and recreate the aroma of meat, she uses the Gas Chromatography-Olfactometry technique, in which beef is broken down into its component chemicals and each of those is associated with a particular smell.
Finding Plant-Based Compounds
The scientists then turn their attention to the plant world to find plant-based compounds with the same characteristics. For Impossible this means they now have a “technology platform, or pipeline” that allows them to do the same for other meat products — for example the recently released Impossible Pork. A similar pipeline approach is used to replicate the texture of meat.
For Impossible, their “secret sauce”, what Kliman says provides the “explosion of meaty flavor” is heme, a chemical found in all plants and animals. In humans, it forms part of hemoglobin, the protein complex that carries oxygen around the body in the bloodstream. To replicate the taste of animal heme, Impossible scientists turned to leghemoglobin, a variant that naturally occurs in soy. They then devised a way to produce it in genetically modified yeast, in order to meet production demands and minimize its environmental impact. According to the company, their process uses 87 percent less water, 96 percent less land, and emits 89 percent less greenhouse gases than it takes to produce traditional beef burgers.
Plant-based alternatives to meat are produced from soy, potato, rice, mung bean, or pea protein and also contain fats to give them the appealing sizzle as they hit the pan. While eating a plant-based diet is often viewed as the healthier option, it is important to realize that eating “Beyond Meat” or an “Impossible Burger” is not necessarily beneficial for health.
Less Cholesterol, More Fiber and Sodium
These products have a similar fat content to beef burgers, and while they have less cholesterol and more fiber than a typical meat patty of the same weight, they do contain more sodium. Professor Kent Kirshenbaum is an organic chemist at New York University, and former scientific advisor to Beyond Meat, who is currently on the board of the Good Food Institute, a non-profit that promotes alternatives to animal food products.
“There is no easy way to answer this question,” he says. “Is it potentially beneficial to move to plant-based sources of food rather than animals? Yes, and I could spend a lot of time telling you why, especially moving away from red meat. However, for those people who are concerned about ultra-processed foods as potentially having deleterious health consequences, they’re absolutely right, this could turn out to be a problem. We don’t know what it is about processed foods that gives rise to health problems, so we really don’t know what the long-term effect is going to be.”
At a Restaurant Near You
From restaurants like David Chang’s Nishi, to Burger King and Dunkin’ Donuts, the Impossible Burger and Beyond Meat products are widely available, and Taco Bell recently announced it will offer plant-based fare within a year. However, not all restauranteurs are so enthusiastic. Chef Silvia Barban, former “Top Chef” competitor and current proprietor of LaRina in Brooklyn, N.Y., offers many vegetarian options on her menu, but none of them contain plant-based meat alternatives. Barban prefers to use her culinary skills to turn locally sourced vegetables into a delicious meal. “I want to sustain the local farmers. I want to try to make great dishes with everything that we have around”, says Barban.
However, in her personal life she finds these plant-based products an easy substitute in dishes like tacos or ramen, when she needs a quick and tasty lunch or late meal after work. While Barban thinks that plant-based meat alternatives are a great addition to fast food, or fast casual restaurant menus, she has no plans to incorporate them in her own menu: “I just use vegetables and I treat them the right way and make it super flavorful. For example, I like to do a beet tartar. It’s vegetarian. It looks like meat, but it’s not — it’s beets and it’s delicious!”
Rethinking How We Eat and Produce Food
It is clear that for our health and the environment, we need to rethink what we eat and how we produce our food. A recent report from EAT-Lancet Commission states that achieving a sustainable and healthy diet worldwide is possible by 2050, but will require a dramatic shift in our approach to eating and agriculture as well as require significant effort and investment from all sectors.
While the report suggests that meat consumption should actually increase in parts of the world where malnutrition is prevalent, in North America, there needs to be a substantial decrease in the amount of meat and dairy consumed. Thus, solutions to the problems of developing a sustainable global food supply chain will take many forms. In western nations, hi-tech plant-based meat alternatives, will almost certainly play a major part in this revolution.
“This is here to stay. Even if part of what’s going on is some element of hype, we don’t have any choice but to drastically reform our food systems, it has to happen,” says Kirshenbaum. “The population is just growing too quickly. Economies around the world are expanding and people are becoming wealthier, which has generally been associated with greater consumption of meat. Just from a global sustainability standpoint, this has to happen.”
The New York Academy of Sciences’ work in nutrition science aims to address global issues such as food security which affects infants, adolescents and the aging population.
According to the United Nations, malnutrition is “a trap from which people cannot easily escape.” And it is a trap that affects every country in the world. In 2015, ending hunger and ensuring access to nutritious food was named one of the U.N.’s 17 Sustainable Development Goals (SDG) for 2030. Efforts to reduce malnutrition stretch back decades and have taken many forms. These include global initiatives that increase access to nutritious foods; government policies that promote healthy diets and set nutrition standards; nonprofit groups that operate food pantries and kitchens; and researchers who study malnutrition and evaluate interventions.
Within the vast landscape of approaches to combat malnutrition, The New York Academy of Sciences Nutrition Science Program has been focusing on where it can make the greatest contributions to nutrition science research. Over the last four years, it has focused on important nutrition science interventions, including the control and prevention of thiamine and micro-nutrient deficiencies and bolstering evidence-based nutrition models.
These activities support a priority for the Academy — addressing global issues such as food security that affect infants, adolescents and the aging population. “Today we can say that the Nutrition Program at the New York Academy of Sciences has become a center of reference on a number of those issues,” said Gilles Bergeron, PhD, Senior Vice President for Nutrition Science at the Academy.
The Academy’s reputation as a neutral convener of experts representing all sides of an issue, makes it the ideal catalyst to assess current scientific evidence writ large. In the case of the Nutrition Program, it also actively evaluates data, and participates in ongoing research needed to design future large-scale programmatic activities.
Filling Knowledge Gaps
For its research on thiamine deficiency, a problem that mainly occurs in low and middle-income countries (LMIC) due to insufficient dietary intake of the B1 vitamin, the Academy’s nutrition science team, together with the Bill & Melinda Gates Foundation, convened a task force in 2017 to take stock of existing data. The team is now collaborating with researchers internationally on several projects to fill in knowledge gaps, determine best solutions to tackle this public health problem, and to assess the prevalence of thiamine deficiency in understudied regions of Africa, such as Madagascar and The Gambia.
Thiamine deficiency can easily go unrecognized, as it did for decades in parts of Asia such as Bhutan and Northern India, because the symptoms are so vague, ranging from the loss of appetite in infants and children, to tingling in hands and feet in adults. But left untreated, thiamine deficiency can rapidly lead to death, and there is increasing evidence that sub-clinical cases — which almost never get detected — can cause long-term cognitive delays and motor skill problems. “We are starting to work on strategies to prevent thiamine deficiency and to raise awareness of its prevalence, which is much, much broader than I think anyone expected,” said Megan Bourassa, PhD, a biochemist and the Academy’s Associate Director of Nutrition Science.
The Academy’s Nutrition Science Program has brought much-needed attention to the issue of thiamine deficiency, according to Frank Wieringa, MD, PhD, senior researcher at the Institut de Recherche pour le Développement (IRD) in Montpellier, France. “In 2012, we knew as much about thiamine deficiency as we did in 1950, there was hardly any progress in those 60, 70 years,” said Wieringa, who served on the Program’s task force and is part of its Scientific Advisory Group.
A High Prevalence of Thiamine Deficiency in Cambodia
Wieringa found a high prevalence of thiamine deficiency in Cambodia, even though the problem has generally been less well recognized by the medical community there than in other parts of Southeast Asia such as Laos. He and his collaborators, including the Academy nutrition team, are currently testing the optimal dose of thiamine to give lactating women in Cambodia. Early data will be available this spring and the hope is to eventually fortify salt with the optimal thiamine dose, much like salt is already iodine-fortified.
On a separate but related front, the Academy has taken on the challenge of trying to improve the myriad of computer models that can guide policy makers, researchers and aid groups in deciding how to tackle malnutrition despite limited resources. The models, which have been developed by academic, governmental and humanitarian groups, can make predictions about important policy questions such as:
Which nutrition issue is the most pressing in a particular setting?
Should attention be directed at certain micronutrient deficiencies or on bigger issues of stunting and underweight populations?
Which intervention(s) would be most cost-effective?
What is the best mix of interventions to achieve multiple concurrent objectives?
With competing models, policy makers may only use the tools that are promoted by the donor they work with (be it The World Bank, USAID or other); and not necessarily the one that is most appropriate for their goals. There needs to be a greater recognition of the diversity of needs and the fit-for purpose of specific modeling tools to the specific task.
The Nutrition Modeling Consortium
Over the last three years, the Academy, with funding from the Bill & Melinda Gates Foundation, has brought together various modelers and launched the Nutrition Modeling Consortium to try to increase awareness of the models in LMIC. Such a partnership was developed to foster collaborations and shared experiences between countries regarding the use of models in decision making.
The Consortium has given modelers the “unique opportunity to sit down and really dig into what these models can do,” said Stephen Vosti, PhD, Adjunct Professor at University of California, Davis, and member of the Consortium. Vosti and his colleagues created MINIMOD, a tool to help plan and manage the most cost-effective micronutrient interventions in LMIC.
So far, the researchers have identified strategies for reducing vitamin A deficiency in Cameroon and plan to deploy the tool to look at other micronutrient deficiencies in countries such as Malawi and Nigeria. MINIMOD could also be used to assess the risk of interventions leading to overconsumption of micronutrients, which is a particular concern in the United States and other developed countries, according to Vosti.
Undernourishment Impacts More than 800 million Globally
With more than 800 million people around the world experiencing undernourishment in 2017, the stakes for the Nutrition Science Program, as well as the many other efforts featured in this issue, could not be higher. Ensuring that all the world’s people have access to adequate nutrition achieves multiple societal objectives. Healthy people are productive people who can work and contribute to long-term economic sustainability.
And a proper diet is foundational in enabling people to fight off disease. It is arguably a gender issue as well. In societies where male children are often more valued than females, girls may not receive adequate nutrition in their formative years, which will impact their ability to bear healthy children of their own.
“Access to nutritious food is a common thread to all population segments,” said Bergeron. “What we do at the Academy is not just about starving children in remote parts of the world, although we recognize the need. Obesity, antibiotics in animal food production, adolescent women nutrition as well as nutrition for the aging, are issues that need to be addressed in developed countries as well.
Here in the United States, it is estimated that one in every 10 adults who are 20 years or older has diabetes. For seniors (65 years and older), that figure rises to more than one in four. The cost of diagnosed diabetes is an estimated $245 billion — money that could go to crucial nutrition programs both in the U.S. and around the world for a healthier society at large.”
Minimizing nutrient deficiencies and ensuring that babies are breastfed optimally are two ways advocates are supporting the healthy development of babies in lower-income countries around the world.
Published May 1, 2020
By Nicholette Zeliadt
About a decade ago, pediatrician Philip Fischer, M.D., began to hear heartbreaking stories about babies in Cambodia who were believed to have “beriberi,” a vitamin deficiency so uncommon in the U.S. that he knew of it only from textbooks as a scourge of the 19th century.
He went to Cambodia to learn more and try to help his colleagues there. They encountered infants so deathly ill, listless, and short of breath that they were often unable to cry and incapable of feeding. And yet miraculously most of them would make a full recovery within thirty minutes of receiving a shot of the vitamin they were lacking: thiamine, also known as vitamin B1.
Fischer and his colleagues found that about six percent of babies in Cambodia don’t live to see their first birthdays, and up to half of those deaths could be attributed to thiamine deficiency.
“That was pretty concerning to us,” said Fischer, professor of pediatrics at the Mayo Clinic in Rochester, Minnesota.
The team is now working to determine the extent of the health problems caused by thiamine deficiency in babies and establishing guidelines for diagnosing it.
The body can’t make its own thiamine, so it has to get it through the diet. Whole grains, nuts, and pork are particularly good natural sources, and today some staples such as wheat flour are typically fortified with it.
In Cambodia, however, as in many countries in Southeast Asia, more than half the diet is made up of white rice, which contains little thiamine, largely due to the processing of the rice, which involves removing the outer layer containing the thiamine. Newborn babies typically get their thiamine through breastmilk, but if their mother is deficient, then the breastmilk is, too.
Philip Fischer, MD Professor of Pediatrics, Mayo Clinic
The most recent estimates suggest that at least 38 percent of infants in Cambodia are thiamine deficient. Similar deficiencies have been found elsewhere across Southeast Asia, parts of India and Bhutan, and several countries in Africa.
“This is more widespread than we thought,” said Kyly Whitfield, Ph.D., assistant professor of applied human nutrition at Mount Saint Vincent University in Halifax, Nova Scotia.
An increased risk of death due to this deficiency is not the only concern: some evidence suggests that having too little thiamine in early childhood may cause lasting impairments in cognitive abilities.
Whitfield foresees a day when families in developing countries can get the thiamine they need through fortified foods, such as salt. She and her colleagues are already testing thiamine supplements in the region to establish how much thiamine a woman needs to consume in order to prevent beriberi in both herself and her infant.
The studies involving Whitfield, Fischer, and their colleagues reflect several initiatives underway that aim to use the latest developments in infant nutrition science to help families in developing nations nurture healthier babies. Prioritizing adequate nutrition for pregnant and lactating women and their babies is critical not only for women’s health, but also for that of future generations and the productivity of these nations.
Multiple Micronutrient Deficiencies
Robert Black, MD Professor of International Health, Johns Hopkins University
Many people in developing countries have deficiencies of multiple vitamins and minerals simply because they don’t have enough food to eat or their diet lacks variety. Pregnant women are especially vulnerable because they require even more nutrients than usual. And it’s not just their own health at stake; their children have an increased likelihood of stillbirth, premature birth, and a variety of birth defects, among other health problems. They also have an increased risk of death before age five and tend to perform more poorly than their peers in school.
It is difficult for a pregnant woman to consume all the nutrients she needs through diet alone. In fact, in most developed countries, pregnant women routinely take prenatal supplements containing multiple micronutrients (sometimes referred to as MMS). By contrast, in most developing countries, pregnant women usually receive a supplement containing only two: iron and folic acid (IFA) — the only two micronutrients that the World Health Organization (WHO) currently recommends that all pregnant women take.
“Women in low- and middle-income countries have many deficiencies that are not currently being addressed,” said Robert Black, M.D., professor of international health at Johns Hopkins University in Baltimore, Maryland.
Clayton Ajello, Dr. PH Senior Technical Advisor, Vitamin Angels Alliance
Indeed, two recent systematic reviews of the scientific literature found evidence that multiple micronutrient supplements are better than supplements of iron and folic acid alone at reducing the risk of a child being born preterm, with low birth weight, or small for gestational age. And the supplements appear to be safe; they do not raise the risk of any adverse events.
“MMS does everything that IFA does, and more,” said Clayton Ajello, Dr. P.H., senior technical advisor for Vitamin Angels Alliance, a nonprofit that provides MMS to mothers and children worldwide.
Because of these added benefits, both Ajello and Black advocate for developing countries with high rates of nutrient deficiencies to replace IFA supplements with MMS, especially in countries where such deficiencies are widespread among women of childbearing age. Progress is slow, in large part because current supplies are nowhere near what is needed to meet the needs of the estimated 206 million women who become pregnant in developing countries each year. However, supplies will increase as more and more countries adopt MMS, Ajello says.
It Takes a Village
Minimizing nutrient deficiencies in pregnant and breastfeeding women is a key part of ensuring the development of healthy babies. Equally important are efforts to ensure that babies are breastfed optimally. The WHO recommends that all babies be breastfed within an hour of birth and continue exclusively for six months. After that, babies should start eating other foods but continue nursing until they are at least two years old.
Melissa E. Glassman, MD, MPH, IBCLC Medical Director, Newborn Clinic and ACN Breastfeeding Support Program in Newborn Clinic Assistant Clinical Professor of Pediatrics Division of Child and Adolescent Health Columbia University Vagelos College of Physicians and Surgeons
Beyond simply providing a baby with its only source of nutrients for the first six months of life, breastmilk protects babies from infections and aids the development of their immune systems. Breastfed infants have lower rates of gastro-intestinal and respiratory infection and lower rates of death from infections overall as compared to non-breastfed infants.
Studies suggest that programs to promote breastfeeding may be an important way to reduce mortality in young children.
“But establishing breastfeeding can be difficult for many women, especially if they don’t have guidance and support,” said Melissa Glassman, M.D., a pediatrician at New York Presbyterian Hospital and Columbia University Irving Medical Center, and the founder and medical director of the hospital’s Newborn Clinic, which provides outpatient care to newborns with Medicaid insurance after they are discharged from the hospital. “It becomes more difficult to raise your baby if you don’t know how to do it and you’re not surrounded by a village that can help you.”
New mothers often do not know what to expect when breastfeeding for the first time. For instance, many have trouble getting a newborn to latch onto the breast properly, causing pain and difficulty with feeding.
And first-time mothers may not immediately recognize cues that their baby is hungry, resulting in too few feeding sessions and weight loss in the infant. What’s more, breastfeeding can be physically exhausting: newborns typically feed at least eight times a day, and each feeding session can last as long as an hour. If women don’t know to expect these feeding patterns, they often assume that they’re not making enough milk and their baby is going hungry. All of these factors may prompt women to give up on breastfeeding too soon.
“There’s nothing worse than a woman wanting to breastfeed, then developing problems with breastfeeding that she doesn’t know how to fix, and not having the support she needs to address these problems,” said Glassman, who provides breastfeeding support to women from a wide range of socioeconomic backgrounds — from those with commercial insurance who visit her at a ColumbiaDoctors practice — to the primarily immigrant population with public insurance who visit the Newborn Clinic. “If we can get women comfortable and on the right foot early with breastfeeding, that will get moms on the path for long-term successful breastfeeding and all the associated health benefits for both mom and baby.”
Enter any drugstore, vitamin chain, big box store, e-commerce site, gas-station convenience store or street corner bodega and you’ll find CBD products — in shampoos, oils, vapes, gummies and even treats for people and pets. Many of these products come with creative claims of the therapeutic benefits of CBD, true or not.
Such mass market hype and wishful thinking aside, Epidiolex®, an FDA-approved breakthrough treatment for rare drug-resistant epilepsies, is currently the only CBD product (cannabidiol) demonstrated to be effective by controlled studies in people.
CBD was previously known as the non-intoxicating sibling of the psychoactive intoxicant THC (tetrahydrocannabinol) — both cannabinoids produced in the marijuana plant. Traditional medicines have used cannabis for millennia, yet the United States first placed legal restrictions on its use in the 1920s and 1930s. In 1970, marijuana became illegal under Schedule I of the U.S. Controlled Substances Act.
CBD, though, received an enormous boost when the Farm Act of 2018 allowed the legal growth and sale of hemp products which include CBD. However, THC remained illegal, along with CBD produced from marijuana. These changes have only added to the ambiguity of CBD’s status from the perspectives of both law and science.
Imagine You’re a Caveman: The Human Endocannabinoid System
In the 1980s and 1990s, researchers identified cannabinoid receptors in humans (CB1 for THC and CB2 for CBD). What they were uncovering was the human body’s own endocannabinoid system (ECS).
“It’s a system as ancient as our immune system and our central nervous system. They co-evolved and our endocannabinoid system acts as a bridge between the two,” says Yuval Cohen, CEO and Director of Corbus Pharmaceuticals. “It’s designed to help us recover from trauma and is absolutely essential to life.”
To illustrate his point, Cohen said: “Imagine you’re a caveman and you just got mauled by a saber-toothed tiger. You are injured, you’re bleeding, you’re going into shock, you’re scared, you’re in a ton of pain; the wound is swollen and tender. You’re a hot mess. And that is where your endocannabinoid system kicks in. Without it, you’re going to die in that cave. It’s that simple.”
He is describing what many CBD promoters claim as general benefits of CBD in any form: pain management, seizure control, physical and psychological trauma relief, and tissue healing. Cohen, himself, sees the endocannabinoid system as an increasingly more explored therapeutic target for new treatments of disease.
Corbus is rationally designing synthetic signaling molecules to target the human ECS receptor molecule CB2 more selectively than a plant molecule could. Corbus’ lead product candidate, lenabasum, is designed to resolve chronic inflammation and fibrotic processes without interfering with the central nervous system.
Patient-Driven Advances
Yuval Cohen, Ph.D. CEO and Director, Corbus Pharmaceuticals, Inc. Photo: Corbus Pharmaceuticals
Elizabeth Thiele, M.D., Ph.D., Director of the Pediatric Epilepsy Program at Massachusetts General Hospital, has firsthand experience with the pain and courage of parents who have exhausted existing medical options for treating extremely ill children. “I think what has really set this whole CBD story apart is that it was the patient community that drove the interest. It wasn’t big pharma saying ‘Here’s this drug we had in trials’,” she said.
Dr. Thiele has direct knowledge of a couple of related cases. One family moved from Maine to Colorado so they could access a CBD product for their daughter’s debilitating, treatment-resistant
epilepsy. A second family, from California, became interested in medical marijuana when their son had trouble with the restrictions of dietary therapy. But they encountered the same difficulty many experience with extracts: consistency of the product. Eventually, the California boy became patient one for Epidiolex in the United States.
“When I first got involved with this, one of my colleagues told me I was risking my career and another that I was wasting my time,” said Thiele. “But my approach has always been that I get parents who are desperate for treatments for their child and I need to support them.”
Still, Thiele firmly warns against trying CBD products whose contents you cannot confirm: “Right now, the only data we have is that purified CBD can be effective in helping children with refractory epilepsy. Parents should be very leery of claims of CBD curing or being good for everything.”
Above and Beyond Caveat Emptor
Margaret Haney, Ph.D. Professor of Neurobiology at Columbia University Medical Center
When states legalize something, people assume it is safe. But experts at government agencies and university-affiliated research institutes continue to seek accurate data about potential health risks associated with cannabinoids, especially for people who may be more vulnerable because of age, neurological development, pregnancy, or interactions with other medications.
THC can affect fetal and adolescent neurological development, but CBD’s effects are still being determined. Data collected during studies of Epidiolex, for example, revealed that CBD affected availability levels of the antiepileptic clobazam, requiring dosage adjustments.
Scientists are actively studying the therapeutic potential of CBD with the removal of hemp from Schedule I.
Among her responsibilities, Susan Weiss, Ph.D., National Institute on Drug Abuse, Director, Division of Extramural Research, represents NIDA in talks on cannabis, marijuana and CBD. “Our goal is to get a better understanding, to get more knowledge and to be able to present evidence in an unbiased fashion,” she said. “We are also interested in developing therapeutics for cannabis use disorder.”
The Legal Hurdles
But NIDA research is not immune to legal ambiguity, jurisdictional conflicts, and their consequential impact on science. “Our researchers can’t actually purchase products from dispensaries because they would be in violation of federal law,” Weiss said. “As a result, NIDA must depend on people self-reporting what they’re using. But we don’t have access to those products to get a good sense of their dangers.”
Margaret Haney, Ph.D., Professor of Neurobiology, Columbia University Medical Center, is a leading researcher on cannabis use disorder but also explores the science behind specific areas of therapeutic value for THC and CBD. “I feel like there’s an anti-science moment right now where people are just believing,” she said. “They’re distrustful of pharma but not of the person selling them CBD at the farmer’s market. People aren’t aware that it’s just snake oil all over again.”
According to Haney, what most stands in the way of large-scale rigorous clinical studies is the DEA Schedule I status for cannabis and cannabinoids, which essentially shuts down the ability to conduct these studies. “If scientists could treat cannabis and its constituents as Schedule II, that would open things up tremendously,” she said.
The Entourage Effect
Ziva Cooper, Ph.D., Research Director of the UCLA Cannabis Research Initiative and Associate Professor in the Jane and Terry Semel Institute for Neuroscience and Human Behavior, understands the strong arguments for the purity, precision and predictability that synthesized THC or CBD molecules can provide in a rationalized drug design approach. But as a pharmacologist she wonders if potential benefits may be lost the further away a drug molecule moves from the whole plant.
“You want to know what the individual constituents do, but then there is this idea that the whole plant can offer greater therapeutic potential because it has all these different chemical components — some call this the entourage effect,” said Cooper.
“This hypothesis hasn’t really been tested in the clinic yet. We’re hoping to begin studying that very soon to determine if these different molecules in the plant work together to improve the potential therapeutic effects of cannabis. Will the combination of these chemicals be effective? What can we expect it will do? What are the risks we should be aware of? I’m confident that over the next 10 to 15 years we’ll actually be able to answer some of these questions,” said Cooper.
Dan Zenowich, a freelance health writer, contributed to this story.
According to the EPA, organic waste is the largest component of landfills. Researchers are working with businesses to develop innovative ways to reduce this problem.
Published May 1, 2020
By Charles Ward
Bertha Jimenez wasn’t a beer drinker when she came across spent grain for the first time.
A mechanical engineer by training and now the CEO of Rise Products, Jimenez recounted her tour of Brooklyn Brewery, a craft beer brewery located in the Williamsburg section of Brooklyn, N.Y.
“I’m interested in how waste from one industrial activity is usable in another,” she said. “So as we walked around the plant, I wanted to know what happened to the source grains after the beer was made.”
Within a year, Jimenez founded Rise, a start-up that converts spent grain into specialty flours sold directly to bakeries. Rise developed a proprietary conversion process, slogged through prototypes and proof-of-concepts, and learned about food safety standards. She built a regional B2B customer base, secured grants, raised private capital, and signed a Service Provider Agreement with Anheuser-Busch.
“People like to feel like they’re doing something sustainable, something good,” she said. “But at the end of the day we don’t eat ideology, you know?”
The Challenge of Food Waste
Jimenez is just one example of the way the scientific community has deeply engaged with the challenge of food waste: as entrepreneurs, researchers, academics, regulatory policy specialists, or NGO advisors.
The U.S. Department of Agriculture (USDA) estimates 31 percent of food produced in the U.S. is loss, with an annual economic value of $161.6 billion. Globally, the U.N. Food and Agricultural Organization (FAO) estimates 1.3 billion tons of food are lost every year in agricultural production, post-harvest storage, processing and distribution, and consumption.
New policy priorities reflect an emerging consensus among food production experts that these are unacceptable numbers for a global food system already stressed by a growing population and climate change. Goal number 12 of the U.N.’s Sustainable Development Agenda is to “ensure sustainable food consumption and production patterns.” Targets include cutting per-capita global food waste in half at the retail and consumer level by 2030, and reducing food loss from production and supply chains. The U.S. Environmental Protection Agency (EPA) and USDA share a similar goal, to cut food loss and waste in half, also by 2030.
Multiple Missions
Upcycling spent grain from breweries. Photo credit: Rise Products, Inc
For Elise Golan, Ph.D., Director of Sustainable Development for the USDA, food waste is a resource efficiency challenge. She works closely with colleagues at the EPA, and references the EPA’s well-known “Food Recovery Hierarchy” inverted pyramid, which visually represents the flow of food from “upstream” agriculture source to “downstream” table, and the parallel opportunities to conserve resources at every stage of the chain.
“We look at reasons for waste, and ask if there are cost-effective ways to reduce it,” she explained. “If we’re producing food that is wasted, [by reducing it] we can conserve the land, water, chemical- and non-chemical inputs that go into that food.”
The USDA’s more active food recovery interventions, Golan notes, are prompted by opportunities to create efficiency all along the value chain. As one relatively upstream example, she points to a pilot collaboration between the USDA’s Agricultural Research Service and The Wonderful Company, a California-based producer of pistachios. The project has the potential to turn mountains of discarded pistachio shells into “carbon black” for use in plastics as an alternative to petroleum-based compounds.
“They’ve done it in a very cost-effective, energy saving way,” said Golan. “It is really is a big win for the environment.”
Food Waste as an Economic Catalyst
If the USDA is working on food waste from the top down, Juan Guzman, Ph.D., is working from the bottom up. Guzman is the head of Capro X, a Cornell University spin-off that uses bioconversion technology to turn the acid whey left over from Greek yogurt production into specialty chemicals. In commercial terms, Capro X is what is classically called a “category creator.”
Guzman thinks of himself first as an entrepreneur, and speaks in terms of business cases: return-on-investments, stakeholder buy-in, and use of science-based innovation to create entirely new markets. When he started Capro X, the commercial imperatives were self-evident: New York yogurt manufacturers needed cheaper ways to get rid of large quantities of acid whey, which they had to truck long-distance for waste-water treatment.
Alternative Sourcing for Industrial Products
At the same time, dairy farmers, generally, were under pressure to develop new products as milk consumption declined. And global agribusiness giants, like Nestlé, Archer Daniels Midland and Cargill, are always seeking alternative sourcing for industrial products, like commercially farmed palm oil, which Capro X intends to produce.
“I just see so much opportunity in using biology to extract value out of things that people are willing to pay to get rid of,” said Guzman, pointing to the historic precedent of ethanol, which made the planting of corn on previously surplus or marginal farm acreage a hugely viable commercial proposition. “For yogurt manufacturers, we’re talking about waste streams measured in the millions of pounds, with one facility alone generating a quarter of a million pounds a day of pure lactose sugar for conversion,” Guzman continued. “And there are hundreds of plants in the U.S.“
For the market to scale, investor interests will have to see the opportunity, and put in capital. In the meantime, Guzman is building his new market one customer at a time. Capro X’s value proposition includes installing the acid whey treatment equipment at dairy farms. He keeps the specialty products, and farmers are spared the expense of trucking away waste. Guzman said he has learned that farmers like the idea of sustainable waste practices, but they are not necessarily willing to pay a price premium for them.
Identify, Measure, Attempt to Solve
Mary Muth, Ph.D., is an agricultural economist who serves as the Director of Food, Nutrition, and Obesity Policy Research at RTI, a not-for-profit organization dedicated to using science for good. Muth has conducted food waste research from every angle: malnutrition, resource efficiency, economic impact, and ethical imperative. She believes that scientific interest in the problem of food-waste is still cresting.
She also points out that that commercial application of food-waste research is still largely voluntary. Some companies see it as a reputation management opportunity, a way to promote corporate social responsibility. A few others have developed niche products. Seismic economic incentives for waste-aware practice don’t yet exist.
“It will probably take some significant disruption in the food supply to bring around big scale change,” Muth said.
Christine Beling, a project engineer and New England regional director of Brownfields and Sustainable Materials Management at the EPA, is as good a witness as any to what seems to be an incremental and steady advance towards reduced food waste. The EPA prefers composting as an alternative to landfills for food waste, and Beling says that a sign of progress is landfill bans of organic waste by four of the six New England states in her region. She notes that in 2015, the EPA calculated that just 5.3 percent of 39 million tons of food waste was diverted for composting; two years later, the figure was 6.3 percent.
“That’s a relatively big jump,” she observed. “If you go back to the late ’90s or early 2000s, it was one percent. I think you can see the trend.”
Entering the Mainstream Conversation
Beling points to a variety of legislative, academic, and NGO attention on food waste and recovery. In 1996, President Bill Clinton signed the Bill Emerson Good Samaritan Food Donation Act, which provides liability protections to nonprofit organizations when they donate food. In 2019, Harvard University launched its Food Law & Policy Clinic, which trains students in the use of legal and policy tools to address food system issues.
Beling also calls attention to the birth of new NGOs like ReFed, founded in 2015, to bring data- and economics-driven tools to help solve food waste problems. And in 2016, the Ad Council and the Natural Resources Defense Council co-sponsored the “Save the Food” national public service campaign.
“The emphasis may be different depending on what part of the world you’re in, but overall there’s a whole shift,” said Beling. “Ten years ago, people didn’t want to deal with food waste. Now, everybody’s dealing with it because it’s in the mainstream conversation.”
Inflammation in the nervous system plays a key role in many acute health problems including Alzheimer’s disease and chronic pain — both of which affect millions of people globally and lack effective treatments. This eBriefing will explore how the body’s failure to resolve chronic neuro-inflammation contributes to disease, as well as highlight opportunities to develop pro-resolving compounds as novel therapies.
In This Webinar, You’ll Learn:
The role of neuro-inflammation as a key component of severe global health problems including Alzheimer’s disease and chronic pain conditions.
How new research suggests that the failure to resolve neuro-inflammation may be a major contributor to the pathology of these diseases.
The latest advances in targeting resolution pathways to develop effective drugs for neurological diseases of high unmet need.
Resolving Neuro-Inflammation to Treat Alzheimer’s Disease and Pain
Speakers
Ru-Rong Ji, PhD Duke University School of Medicine
Marianne Schultzberg, PhD Karolinska Institutet
Video Chapters 04:38 Marianne Schultzberg, PhD 28:13 Ru-Rong Ji, PhD
Marianne Schultzberg, PhD
Karolinska Institutet
Marianne Schultzberg has been Professor of Clinical Neuroscience at the Department of Neurobiology, Care Sciences and Society at the Karolinska Institutet since 2005. Her research focuses on the role of neuroinflammation in neurodegenerative disorders such as Alzheimer’s disease (AD) and in recent years has focused on the potential roles of pro-resolving mediators in AD pathogenesis. She received her PhD in 1980, carried out post-doctoral research at Liverpool University and became Docent (Associate Professor) at the Karolinska Institutet in 1983.
Ru-Rong Ji, PhD
Duke University School of Medicine
Ru-Rong Ji is the chief of pain research within Duke Anesthesiology, co-director of the Center for Translational Pain Medicine, and a professor of anesthesiology and neurobiology. He research focuses on understanding the molecular and cellular mechanisms of chronic pain, such as inflammatory pain, neuropathic pain, and cancer pain. He earned a PhD in neurobiology at Shanghai Institute of Physiology and completed postdoctoral training at Peking (Beijing) University Medical School, Karolinska Institute, and Johns Hopkins University School of Medicine. He was associate professor at Harvard Medical School, before joining the Duke faculty in 2012.
It’s important to focus on evidence-based information about the disease, and their remedies.
Published March 19, 2020
By Roger Torda
As the new coronavirus continues its spread in the United States and worldwide, elected officials, healthcare providers, and private citizens are grappling with the wide-reaching implications of the pandemic. In uncertain times, it’s important to focus on evidence-based information about the disease, efforts to mitigate its spread, and prospects for a vaccine or treatments.
In an effort to provide a topline view of what the public needs to know about the virus, the Academy brought together Julie Gerberding, MD, MPH, Executive Vice President and Chief Patient Officer, Strategic Communications, Global Public Policy, and Population Health at Merck & Co. and former Director of the Centers for Disease Control and Prevention, and Michael Osterholm, PhD, MPH, Director of the Center for Infectious Disease Research and Policy at the University of Minnesota, to share insights from their extensive experience, as well as from the latest research.
In a webinar held on March 12, 2020, both Gerberding and Osterholm addressed the challenges ahead and the opportunities for action.
Perspective and Preparedness
Key Takeaways
The global health community has successfully addressed multiple pandemics over the past two decades, including the coronaviruses SARS and MERS, H1N1 influenza, and Zika virus.
The new coronavirus is highly transmissible and challenging to contain. Public health efforts are focused on slowing the spread within communities.
Julie Gerberding
Dr. Gerberding began the webinar with a reminder that while this strain of coronavirus is new, it is not the first disease to threaten the global population. “We have a lot to learn about how this virus spreads and how we can intervene in that process…but we have a foundation of experience in previous outbreaks,” Gerberding said. “Each time we have one of these new outbreaks, we learn things, our preparedness takes a step forward, and we need to…develop some confidence that we’re going to figure this one out too.”
Limits to Testing
While the new coronavirus was detected quickly in China and reported to global health authorities, limited access to testing, both in China and around the world—including in the United States—have hampered efforts to understand the scope of infections worldwide. Gerberding explained that China’s “extraordinary measures” to contain the virus limited spread within the country and delayed transmission to other countries.
Despite these containment efforts, the new coronavirus has spread to more than 110 countries in just three months, a fact Gerberding deems “unsurprising” given its high transmissibility.
With containment no longer a priority, countries and communities worldwide are enacting measures to slow the spread of the virus.
The New Coronavirus: Origin, Transmission, Vulnerable Populations
Key Takeaways
The new coronavirus spreads primarily through person-to-person contact.
Most cases are mild. Older individuals and those with underlying medical conditions are at greatest risk of developing serious complications.
Much remains unknown about the new coronavirus. The case fatality rate is likely to evolve as the disease spreads, and these numbers may vary by country.
Origin and Transmission
Coronaviruses, named for the characteristic “crown” of protein spikes that jut from the viral surface, commonly infect humans, causing mild cold symptoms. The new coronavirus strain, SARS-CoV2 (commonly referred to now as the “new coronavirus” or “COVID-19″), originated in bats, evolved to infect small mammals, and ultimately “spilled over” into the human population. Because the virus is not native to humans, “we have no reason to believe anyone is immune to this,” Gerberding said.
Michael Osterholm
The new coronavirus is highly transmissible. Dr. Osterholm explained that the reproduction number, or the R0, is estimated to be between 2 and 3—meaning that without precautionary measures, each infected person will pass the infection to at least two others. Comparatively, pandemic influenza has a R0 of about 1.2.
The new coronavirus spreads primarily from person-to-person through aerosolized droplets released when an infected person coughs or sneezes. Masks can help prevent spread when worn only by sick individuals, as can isolation and covering sneezes and coughs. Osterholm noted that “we have very little data” on the viability of the new coronavirus on surfaces.
“I don’t want to downplay the importance of handwashing…but surface contamination is not something people should be preoccupied with,” he said. [Update: According to a March 17, 2020, study by the NIH, “Scientists found that severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) was detectable in aerosols for up to three hours, up to four hours on copper, up to 24 hours on cardboard and up to two to three days on plastic and stainless steel.”]
Vulnerable Populations
Approximately 80 percent of coronavirus infections are mild, causing fever, dry cough, and fatigue that resolve with no complications. However, older patients, and those with pre-existing medical conditions including cardiovascular disease, diabetes, or lung disease are at higher risk of potentially severe complications. These include shortness of breath and pneumonia, which may require medical intervention and intensive respiratory support.
The World Health Organization (WHO) estimates the case fatality rate of the new coronavirus at 3.4 percent, although some studies found fatality rates between 1 and 2 percent. “That’s still 10 to 20 times higher than seasonal flu,” Osterholm said. He noted that case fatality varies among countries, a trend he anticipates will evolve as the disease spreads worldwide. Factors such as the overall age of the population, along with rates of cigarette smoking and comorbidities such as obesity, are likely to influence the fatality rate.
Slowing the Spread in Communities
Key Takeaways
Slowing the spread of the new coronavirus is critical for minimizing impacts on the healthcare system and protecting vulnerable populations.
Common sense measures can significantly impact community spread, including minimizing large group gatherings and staying home when ill.
Testing is critical for understanding the extent of community spread; prevalence of testing will increase in the coming weeks.
Drastic Action
Osterholm emphasized that coronavirus will be a concern for months, rather than days or weeks. “It’s very important that we understand what we’re talking about today is a long haul,” he said. He also cast doubt on the prospect that that the new coronavirus may decrease in prevalence as the weather warms, noting that the earlier coronavirus MERS emerged in the Middle East, in temperatures as high as 110°F. “Of the previous 10 pandemics, 2 started in the winter, 3 started in the spring, 2 started in the summer, and 3 started in the fall,” he said.
Widespread closures and social distancing measures enacted in China did help to slow disease spread, and other countries are enacting similar restrictions, such as cancelling large gatherings, limiting travel, closing schools and houses of worship, and encouraging telecommuting when possible. Although, Osterholm did note that little is known about the potential for the disease to resurface once restrictions are eased, and such measures are deeply disruptive to everyday life, often having downstream consequences for families, businesses, and essential services. Osterholm explained that while children appear to be largely unaffected by the new coronavirus, little is known about the role of children in spreading the illness.
Gerberding acknowledged the difficulties of balancing disease suppression efforts with maintenance of basic services. “We also have to concentrate on keeping our societies functioning—people need goods and services,” she said.
Reducing Healthcare Burden
Slowing disease spread is essential to reducing the burden on healthcare systems, which have neither space, staff, nor equipment to manage large numbers of critically ill patients. “If 100 cases of infection occur today, and they need high-intensity medical care, that’s a very stressful situation for any healthcare system,” Osterholm said. “If you are able to stretch them out, 10 new cases every week for 10 weeks…that may very well have a big impact on the overall outcome for patients.” Shortages of personal protective equipment, including respirator masks, contribute to the urgency surrounding moves to stanch spread of coronavirus.
Testing Availability
Gerberding addressed the lack of widespread testing in the United States, noting that in addition to large medical diagnostics companies, some medical institutions are also developing coronavirus tests. “Over the next few days, we’re no longer going to see testing as the bottleneck that it was in the early phase,” she said.
Increased testing access is likely to usher in a “catch-up period,” where, according to Gerberding, the public may “feel like the outbreak is moving faster than it really is.” Widespread testing is critical to “filling the gaps” in understanding both the prevalence of the virus in communities as well as the range of disease presentations. “The important thing…is that we get the broadest understanding of who is infected with disease, who is infected with mild symptoms, who is exposed and infected but not symptomatic, and who has been exposed but didn’t get sick,” Gerberding said.
Both Gerberding and Osterholm believe it’s likely that community spread is more prevalent than current testing has indicated, mainly because testing has focused on patients with severe disease. “We’re looking at the tip of an iceberg, but we really don’t know how big the iceberg is,” she said.
The Future: Vaccines and Treatment
Key Takeaways
More than 40 companies are working on a coronavirus vaccine and treatments.
Treatment options will likely emerge before a vaccine, which is expected to take 1-2 years.
A vaccine to prevent the new coronavirus is “the holy grail,” said Osterholm, but it’s a vision unlikely to be realized in the near term. Since the SARS outbreak in 2003, “biotech and biopharmaceutical capabilities have moved ahead by light years,” Gerberding said, and more than 40 companies are working to develop a coronavirus vaccine and treatments. Despite a strong start to the vaccine development process—Gerberding said there are “many more candidate vaccines than we’ve ever had at the beginning of a new infectious disease outbreak”—experts anticipate that development, testing, and widespread vaccine availability will take 1-2 years.
Treatment options are likely to emerge in the near-term, although Gerberding doesn’t expect “anything to miraculously come into the medicine chest” to impact the sickest patients. “Once people have pneumonia caused by this virus, what’s going on isn’t due to the virus per se… but to the inflammatory response and the damage that creates,” she said. Gerberding hopes to see treatments emerge that prevent severe complications in patients already exposed to the virus. Recovered patients, who are believed to have some immunity to the disease, may offer clues to guide the search for antibody-based coronavirus treatments.
Gerberding concluded with a note of hope and resilience. “It’s normal to be concerned and frightened about something this new and potentially this serious,” she said. “Concentrate on how you can protect yourself, how you can prepare yourself and your family, and convert that energy and concern into action, not panic. We can work together to slow down the spread of this virus and I’m confident, based on what I’ve seen through many outbreaks in the past, that we’re up to this as Americans and as global citizens.”
The Academy, Mount Sinai and Sweden’s Sana Labs team up to “upskill” nurses volunteering to treat COVID-19 patients in New York City.
Published April 16, 2020
By Roger Torda
The New York Academy of Sciences (the Academy) has helped launch a transformational artificial-intelligence-based online learning program to increase the number of Registered Nurses able to handle the explosion of COVID-19 patients in New York City’s Intensive Care Units (ICUs).
Leveraging its global network of expertise, the Academy identified a cutting-edge online learning company, Sweden’s Sana Labs, that was willing to donate its team pro bono to meet New York’s need. The world-renowned Mount Sinai Health System, one of the largest in New York with eight hospital campuses, jumped at the chance to “upskill” their heroic nurses and provided Sana with curricula drawn from the American Association of Clinical Care Nurses and Mount Sinai itself. In record time, this material was transformed into a 16-hour course that can be taken in short batches during break time or at home on personal computers.
So far, about 100 nurses in a pilot program at Mount Sinai Hospital System have used this innovative learning platform. As many as an additional two thousand Mount Sinai nurses may take the training in weeks ahead, according to Sana Labs.
Says Mt. Sinai’s Jane Maksoud, Senior Vice President and Chief Human Resources Officer for Mount Sinai Health System: “The profound shortage of intensive care healthcare workers and other ICU staff available to operate mechanical ventilators during a pandemic will be one of the most significant hurdles facing U.S. hospitals treating critically ill COVID-19 patients. I cannot express my gratitude enough for the work that this team is doing.”
Expanding the Program
Now that this pilot is up and running, Sana and the New York Academy of Sciences are working to expand the program to other hospitals in the New York City metropolitan area, and across the United States. Ultimately, an even more crucial need may arise if cases of COVID-19 explode in the world’s Developing countries.
“Project Florence is designed to deliver personalized learning at scale and we’re making it available for free to any hospital or emergency care unit in the U.S. in need of quickly upskilling nurses for work in the ICU,” said Joel Hellermark, founder and CEO of Sana Labs. The project honors Florence Nightingale, the nursing pioneer. Sana Labs’ platform uses Artificial Intelligence to customize learning for individuals, improve retention of knowledge, and increase flexibility in training.
The Academy’s Ellis Rubinstein played a central role in bringing Sana and Mt. Sinai together for this initiative. “We recognized the important contribution Sana’s learning platform could make as the healthcare system in New York mobilized against COVID-19,” said Rubinstein. “As healthcare systems throughout the city, country, and world face scarcities of trained talent, we are prepared to use the global network of The New York Academy of Sciences to link the Sana Labs team to those in need.”
“I’m very excited to bring this innovative approach to Mount Sinai hospitals to help advance the skillset of our nurses,” said Diane Adams, Chief Learning Officer at Mount Sinai Health System. “Not only are we advancing learning for our health care system, but we are also meeting the needs of our community during a particularly critical time across New York City, the United States and the rest of the world.”
A Proud History of Advancing Medicine and Healthcare
The Academy has a strong background in rapid response to new developments in medicine and healthcare. As early as the mid-1940s, the Academy held a ground-breaking conference on antibiotics. Events hosted at the Academy as early as the 1960s focused on the carcinogenic threat of asbestos, a popular building material at that time. In 1983, the Academy hosted the world’s first major conference on AIDS, just as the scientific community identified the virus that causes the disease.
When the world became aware of a mysterious pneumonia called SARS in early 2003, the Academy quickly convened the first multi-sectoral meeting of scores of the world’s expert scientists and physicians from academia, government and the pharmaceutical industry. Six years later, in 2009, the Academy mounted a similar response to H1N1, the so-called swine influenza outbreak. In 2012, the Academy used its ability to convene diverse stakeholders to sponsor a conference exploring conflicts between scientists and biosecurity officials over research on the H5N1 influenza virus.
“We are very proud that the Academy can leverage its experience in the Life Sciences to make important contributions to world-wide efforts to address the COVID-19 pandemic,” Rubinstein said, referring to the upskilling initiative as well as the Academy’s robust series of programs for sharing scientific developments on the novel coronavirus.

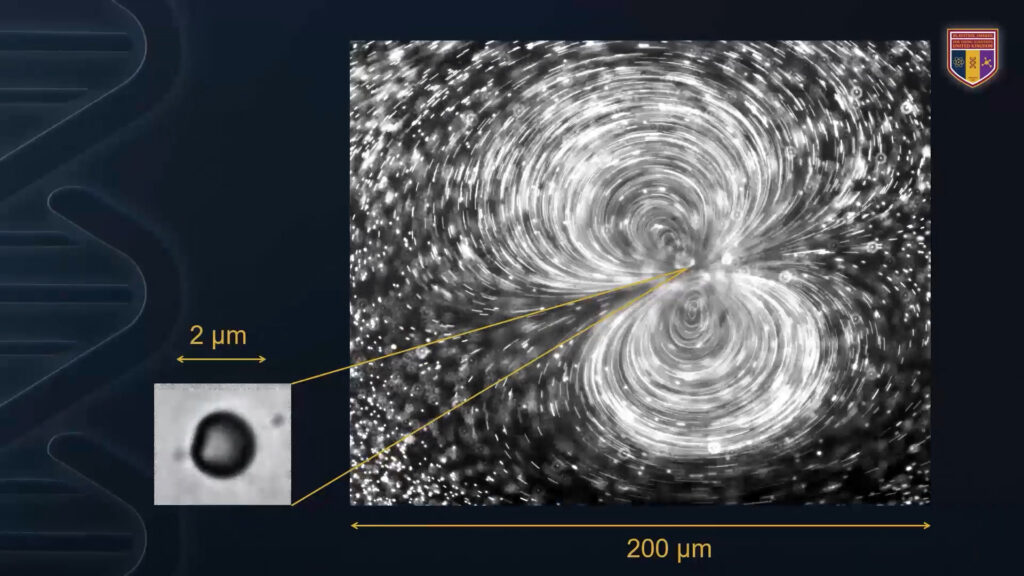
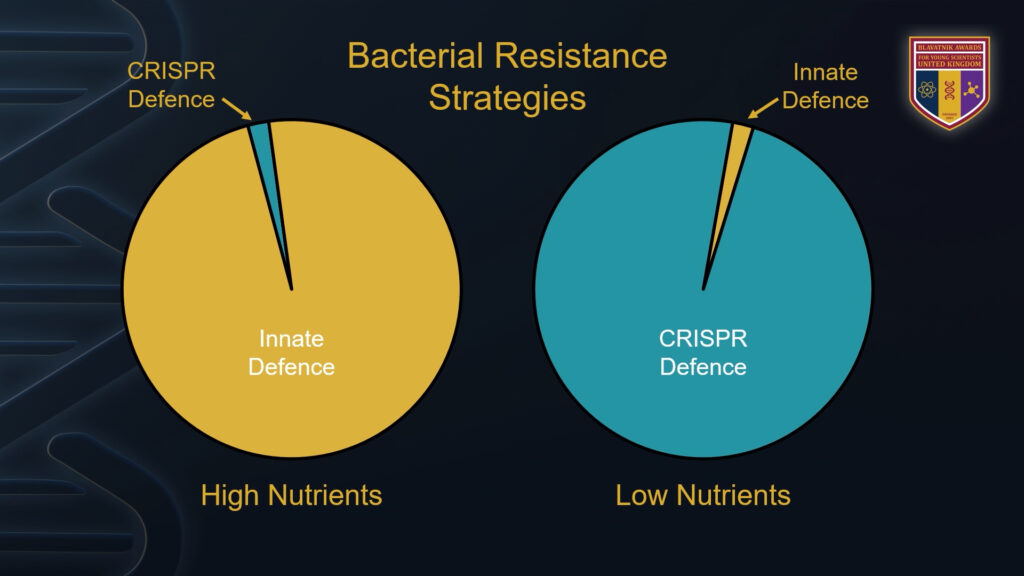
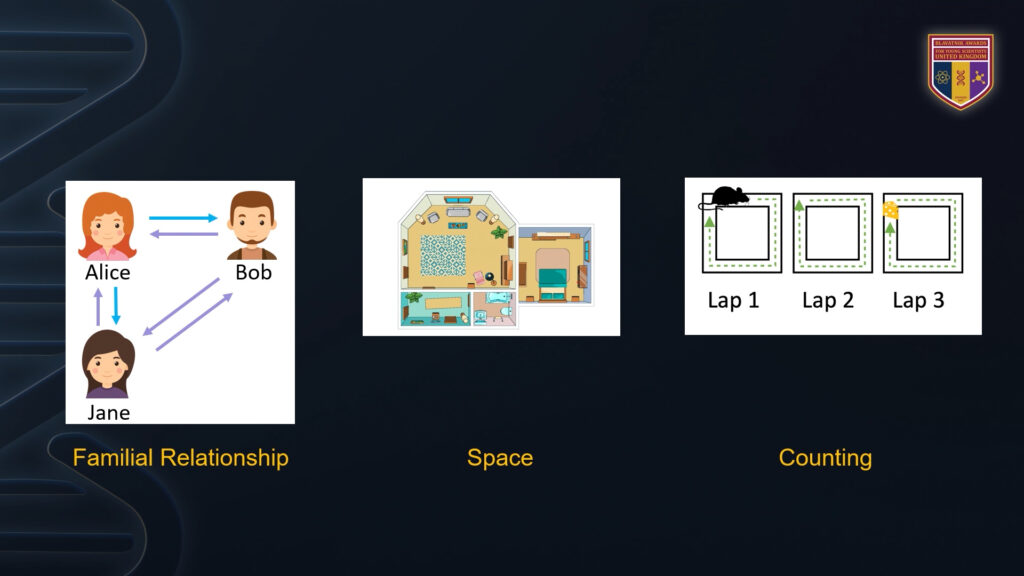
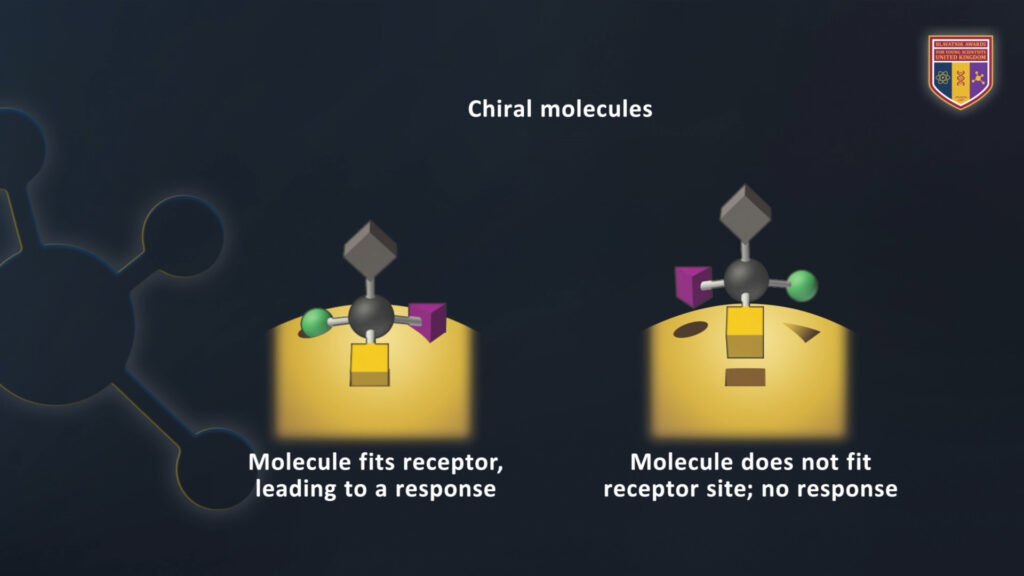
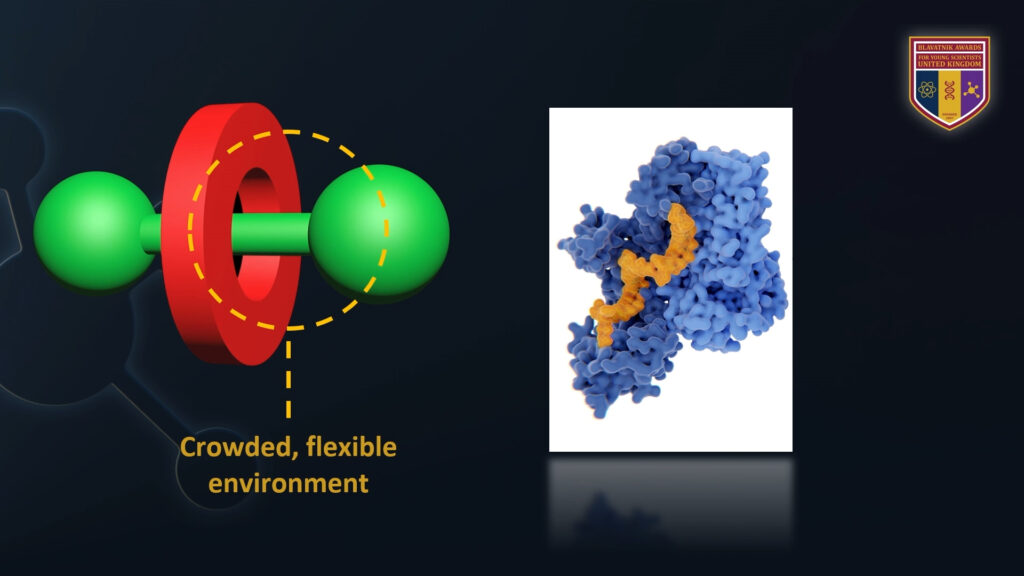
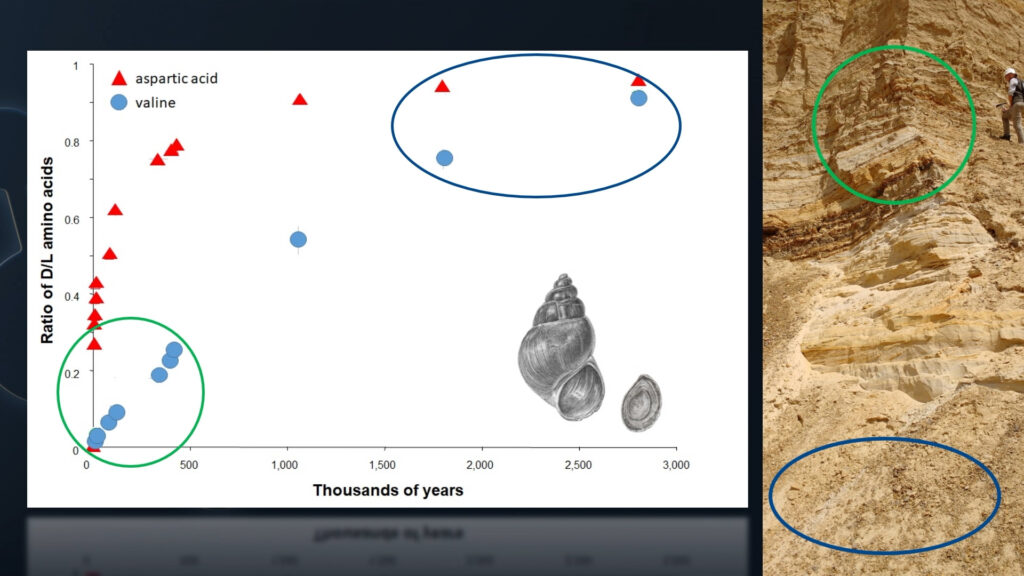
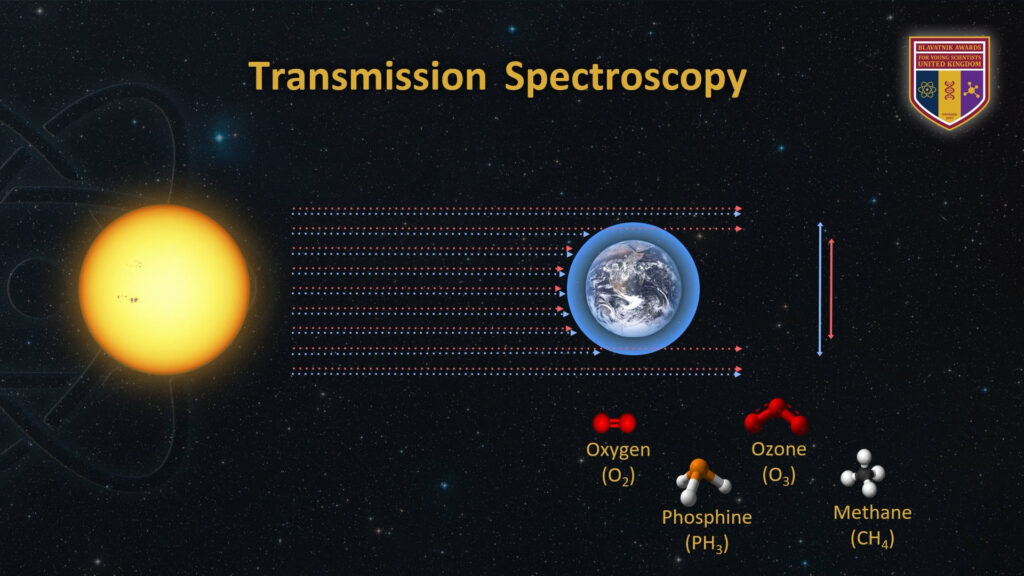
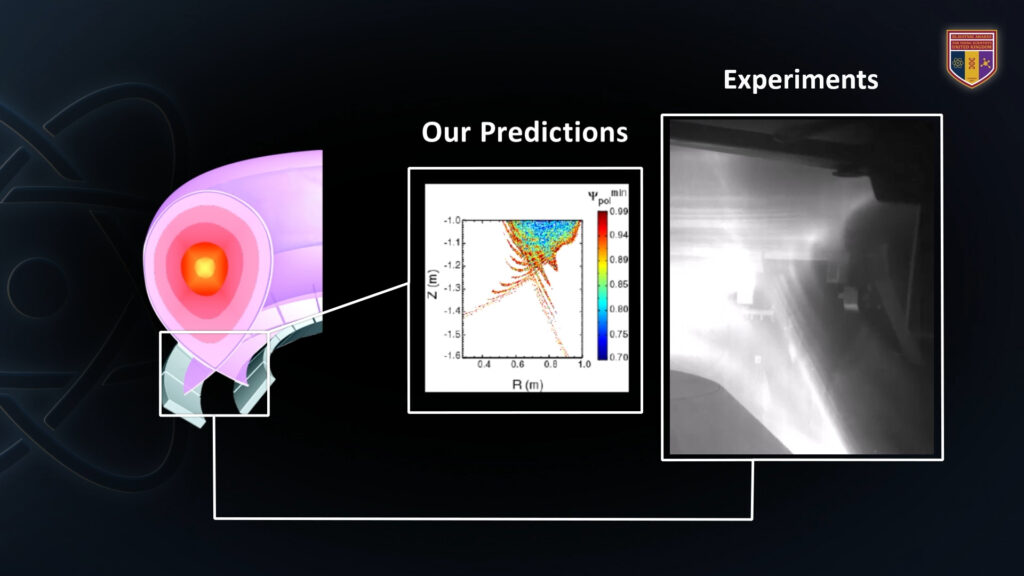
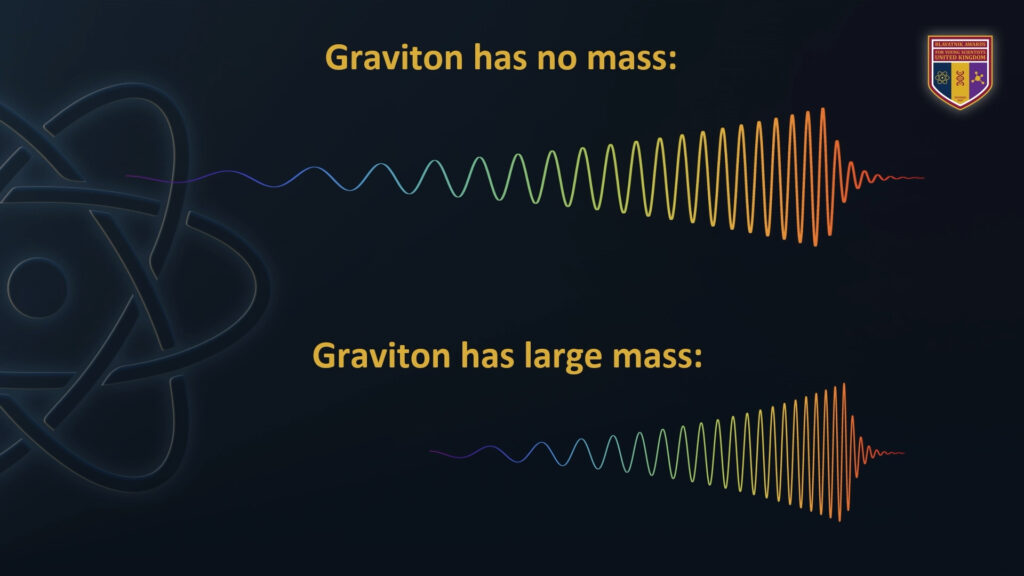













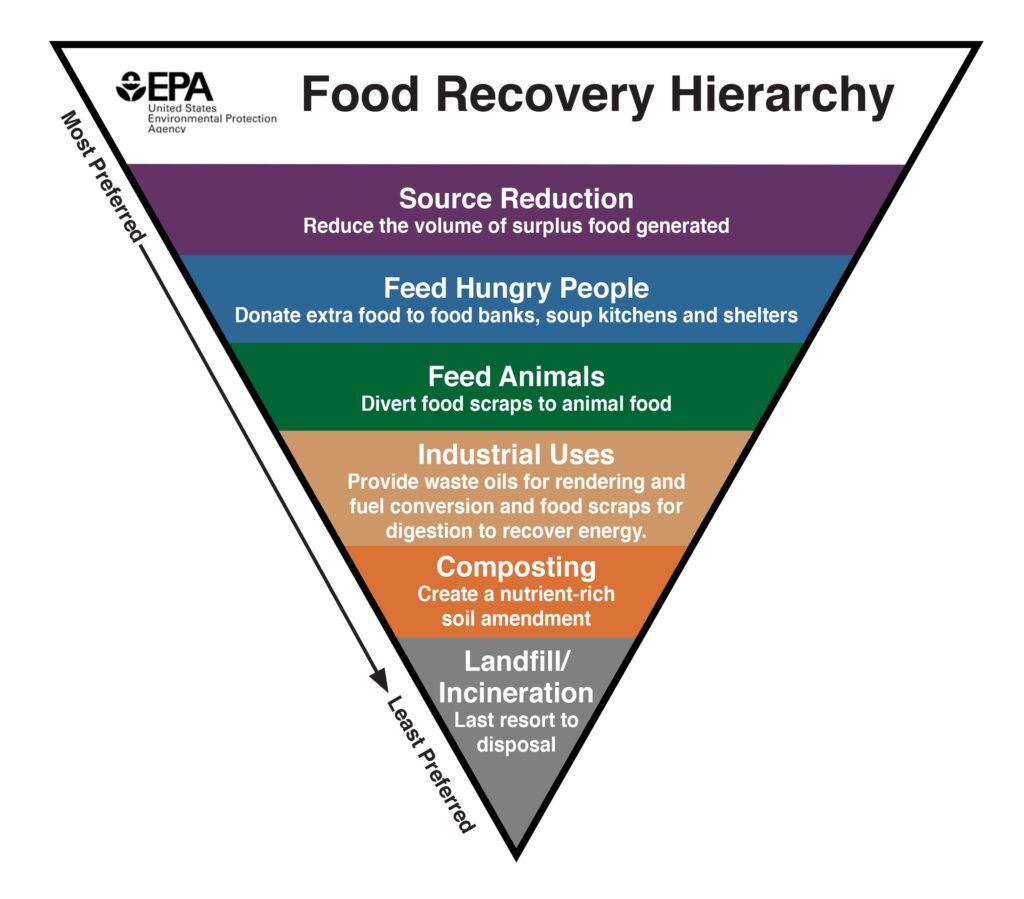





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}