Researchers explore the physiological mechanisms of aging with the ultimate goal of improving health.
Published March 11, 2020
By Hallie Kapner
When mechanical engineer Carlotta Mummolo, neurobiologist Eleni Gourgou, and neuroscientist Teppei Matsui were teamed up in the Interstellar Initiative — an international mentorship program for early-career investigators — their first task was finding common ground.
Eleni Gourgou, PhD University of Michigan
“We have such diverse backgrounds that I initially joked we were speaking different languages,” Mummolo said. “Overcoming that challenge was fun and exciting, and with the help of our mentors, we found a research direction that unites our expertise.”
Organized around the theme of Healthy Longevity, the workshops challenged researchers to develop a plan for exploring the physiological mechanisms of aging, with the ultimate goal of using their findings to improve healthspan, or the time during which a person is healthy.
We spoke with the winning team about their forthcoming grant proposal, the importance of international collaboration, and their advice for young scientists.
Describe the area of research your team is pursuing.
Carlotta Mummolo, PhD New Jersey Institute of Technology
Teppei Matsui, PhD, University of Tokyo: We chose to focus on age-dependent changes in the relationship between motor behavior and cognitive behavior.
Eleni Gourgou, PhD, University of Michigan: Carlotta is an engineer and roboticist whose work mostly focuses on humans, Teppei is an expert in brain imaging in rodents, and I study neurobiology using roundworms as a model system. These organisms are very different when it comes to the complexity of the nervous system, behavior, and how they experience aging. We looked at the questions we’re addressing in our own research, then tried to find a common thread that allows us to use three different organisms as three different approaches to address the same target. That thread turned out to be locomotion and cognition.
TM: By bringing this problem to the abstract level— motor behavior versus cognitive behavior as a function of age—we can study different animals within the same framework.
Carlotta Mummolo, PhD, New Jersey Institute of Technology: This is the novelty of our project, because assessments of motor and cognitive performance are usually done separately. But we wanted to integrate them and look for a methodology that translates across species.
EG: The final research proposal is still taking shape. We will continue to work on it, then submit it to an international funding agency.
Mentorship by senior scientists is central to the Interstellar Initiative–how have your team’s mentors shaped this experience?
Teppei Matsui, PhD University of Tokyo
CM: For early-career scientists, mentorship is everything, and that’s true even more so in this case. Our mentors—Frank Kirchhoff of the University of Saarland and Haruhiko Bito of the University of Tokyo Graduate School of Medicine—pushed us to broaden our mindsets and step out of our comfort zone to find a unified approach. We’d also like to thank mentors Lawrence Hunter, Sofiya Milman, Mahendra Rao, Ikue Mori, and Meng Wan for helping shape our research idea.
TM: Mentorship is very important, and Interstellar Initiative mentors are prominent researchers who have experience with both obtaining competitive grants and reviewing grants. In the first meeting, we received valuable advice about to make our project more appealing and convincing to grant reviewers.
CM: One of our mentors told us something that I’ve kept in mind throughout this project—she told us to focus on integration, innovation, and impact. That was very helpful.
How can international collaborations help further scientific careers and scientific discovery?
TM: Biology is becoming a “big science” these days, and it is necessary to form a big team of experts to do cutting-edge science. For small countries like Japan, it can be difficult to find experts within the country.
EG: International collaboration isn’t new to most of us, but the way we collaborate in the context of the Interstellar Initiative is very different. Many of us have different professional backgrounds and training, and the concept of collaboration doesn’t have the same meaning for everyone. There are cultures of collaboration that you have to integrate in order to work together, and this is something I may not have experienced if it wasn’t for the Interstellar Initiative. It was a great, eye-opening experience for me.
CM: When you exchange ideas with people from different backgrounds, you never know what could come from the conversation. Sometimes that’s how very interesting scientific ideas come about.
What advice can you offer to young scientists?
CM: Step out of your comfort zone! Don’t be afraid, and don’t hold back when you have opportunities to do things outside of your field or your usual mindset.
EG: There’s always something to learn from people—from peers and mentors, of course, but also from people in earlier stages of their careers. Their perspective might shed light on a different aspect of our own work.
TM: I’d encourage young scientists to apply for the Interstellar Initiative.
Organic chemist Steven Townsend of Vanderbilt University explains his research on human milk oligosaccharides (HMOs) and their role in developing babies’ microbiome and preventing infection.
Published January 30, 2020
By Marie Gentile and Roger Torda
It is well understood that human milk provides numerous benefits to babies as they develop, particularly in its ability to help protect babies from a variety of infections. But what is the mechanism that is doing the work to help keep babies healthy?
Organic chemist Professor Steven Townsend of Vanderbilt University speaks to us about his research on human milk oligosaccharides (HMOs) and their role in developing babies’ microbiome and preventing infection. He also discusses the importance of sharing his science with the general public.
Your work has focused on human milk oligosaccharides. Can you explain what these are and why they are important for an infant’s health?
Oligosaccharide is the scientific term for sugar. Human milk oligosaccharides (HMOs) are the complex sugars that are present in human milk, but not in cow’s milk. In human milk, there are about 200 oligosaccharides. By analogy, cow’s milk only contains small quantities of about 30 to 40 oligosaccharides.
HMOs increase the health of the infant in a number of ways. These molecules selectively feed commensal (good bacteria) over bad bacteria. They also protect against bacterial infection by mimicking molecules that pathogenic bacteria use to attach to the gut – the HMOs bind to these pathogens instead and remove them from the system. Recently my group has discovered that these compounds also have intrinsic antimicrobial activity – they actually inhibit the growth of pathogenic bacteria.
Steven D. Townsend, PhD Assistant Professor of Chemistry Vanderbilt University
Together, these factors mean that the microbiome of a breastfed infant is selectively engineered to have more commensal species present, outnumbering pathogens and potential pathogens.
How did you become interested in the biology of human milk?
My interest in human milk first struck when my wife and I were walking through Harlem one day. We saw some advertisements for infant formula. In many parts of the world it’s actually illegal to advertise formula, but here in a poor neighborhood in New York City, were formula advertisements. If you go downtown to the East 50s, a more affluent neighborhood, you don’t see any formula advertisements, you see advertisements for breastfeeding. I wanted to know why breastfed babies are typically healthier.
How does human milk differ from formula?
When it comes to milk broadly, the main constituent macromolecule is typically lactose, a sugar (carbohydrate). Most bigger animals also have a lot of protein in their milk, usually one third of the macromolecules, but human milk is different, as only about 6% of the macromolecules are proteins. For human babies and primate babies, it’s more important for our brains to develop faster than our body, which requires more carbohydrates.
Primate milk has a large quantity of complex sugars with a variety of activities – some of the sugars are involved in brain development and some of them are involved in the development of the immune system. Interestingly, we know that for many of these sugars, the baby does not get calories from them, even though they consume grams of them per day. It turns out that the sugars are actually fermented by bacteria in the gut. These sugars are selectively consumed by good bacteria to give them a growth advantage over bad bacteria. Therefore, if they are not present in formula, then formula-fed babies are going to be at a slight health disadvantage.
Are there any other uses for HMOs besides in the development of an infant’s biome?
There are a lot of companies attempting to put HMOs into different food products, for both infants and adults. For example – some companies are trying to develop products for irritable bowel syndrome and other illnesses that are related to a screwed up microbiome.
In my group, we are investigating if HMOs can help antibiotics work more effectively. Many antibiotics have been mis- and over-used and a lot of them are no longer effective. Our research is finding that co-dosing certain antibiotics with human milk sugars results in a synergistic effect – they work together, which means that you can ultimately use less of the antibiotic to kill a bacteria. That’s cool because antibiotics have a lot of negative side effects, but HMOs don’t have side effects.
You often describe yourself as a humanist. How does this inform your scientific research?
When I say I’m a humanist, I mean I care about people’s day-to-day wellbeing.
The humanist part of me is enhanced by communicating the results of our research with the public and getting feedback on different directions that we could pursue. We’re getting a lot of good project ideas from talking to a broad range of people. It’s very important to me that the general public understand the science we’re doing at a fundamental level because they fund it—I think we owe it to them to explain the research we’re doing and get their feedback.
Mammalian cells can make up to 20,000 different proteins, which are responsible for a wide range of cellular functions, including structure, catalysis, transport, and signaling. Proteins are synthesized as linear chains, but to carry out their myriad roles, they must then fold into complex three-dimensional configurations.
Franz-Ulrich Hartl, MD, of the Max Planck Institute of Biochemistry and Arthur Horwich, MD, of Yale School of Medicine and Howard Hughes Medical Institute, have dedicated their careers to better understanding the molecular machinery that drives protein folding, and the implications when a protein misfolds. In doing so, they discovered a new class of proteins, part of the chaperone family, responsible for protein folding.
Chaperones bind to peptide chains as they are being transcribed to prevent them from aggregating and to give them an isolated, quiet space, shielded from the hubbub of the crowded cytoplasm, in which to fold properly. This process is essential to human biology and health, because misfolded proteins are associated with aging and diseases including Alzheimer’s disease, Parkinson’s disease, Huntington’s disease, and prion disease.
On October 4, 2019, prominent scientists gathered at the New York Academy of Sciences to grant the 2019 Dr. Paul Janssen Award to Hartl and Horwich for their groundbreaking insights into chaperone-mediated protein folding. The symposium included award lectures from the honorees, as well as presentations on several aspects of protein folding, from basic biology to the implications for human disease.
Symposium Highlights
While studying mitochondrial protein import, Horwich and Hartl hypothesized that the process may not be spontaneous but dependent on cellular machinery. They discovered a new class of proteins responsible for protein folding.
Hsp60, its bacterial homolog GroEL, and its eukaryotic homolog TRiC have a double ring structure that forms a chamber in which a peptide substrate can fold into its proper shape.
The unfolded protein response of the endoplasmic reticulum responds to the presence of misfolded proteins, which accrue with age. The response itself declines with age.
Hsp70 is a diverse family of monomeric chaperones that binds to polypeptide chains as they’re being translated or when they misfold from mutation or stress and prevents them from collapsing into aggregates.
Clinically relevant receptors that have been difficult to treat require specific chaperones that may provide more easily druggable targets for neurological and psychiatric disorders.
Honorees
Franz-Ulrich Hartl, MD Max Planck Institute of Biochemistry
Arthur Horwich, MD Yale School of Medicine and Howard Hughes Medical Institute
Speakers
David S. Bredt, MD, PhD Janssen Pharmaceutical Companies of Johnson & Johnson
Andrew Dillin, PhD University of California, Berkeley and Howard Hughes Medical Institute
Judith Frydman, PhD Stanford University
Lila M. Gierasch, PhD University of Massachusetts Amherst
Event Sponsors
This symposium was made possible with support from:
Dr. Paul Janssen Award Lectures
Speakers
Franz-Ulrich Hartl Max Planck Institute of Biochemistry
Arthur Horwich Yale School of Medicine and Howard Hughes Medical Institute
Highlights
Chaperones prevent the formation of toxic protein aggregates, and failure of the chaperone system is associated with numerous age-dependent proteopathies and neurodegenerative diseases.
GroEL mediates two key actions on a substrate polypeptide: binding in the open ring forestalls aggregation and can exert unfolding, while binding in the closed ring holds the polypeptide in “solitary confinement,” giving it a chance to fold on its own and alleviating the risk of aggregation.
Molecular Chaperones — Central Players of the Proteostasis Network
“Protein folding is the final step in the information transfer from gene to functional protein, and as such is of fundamental biological importance,” began Franz-Ulrich Hartl.
In the 1950s, biochemist Christian Anfinsen showed that denatured proteins could refold spontaneously in vitro, thus revealing that all of the information required for a protein to attain its final structure is contained in its amino acid sequence. The study was somewhat misleading, however, as it only used small proteins — under 100 amino acids long — and it started with a completely synthesized amino acid chain. This hardly recapitulates the conditions under which proteins must fold in the cell, where many proteins are large, have multiple domains, fold as they are being synthesized on the ribosome, and are in the very crowded cytoplasm.
In the late 1980s, growing evidence showed that cellular machines were required to help proteins fold “at biologically relevant timescales.” These machines were deemed molecular chaperones, as they help proteins achieve their final active conformations but are not themselves part of the final structure. Hartl and Horwich initially discovered chaperones using mitochondria as a model system.
Mitochondria import about 1,000 proteins from the cytoplasm, and these proteins must be unfolded to get across the mitochondrial membranes. Based on Anfinsen’s experiments, it was thought that they would then spontaneously fold properly once inside the mitochondria. But proteins in yeast with mutant Hsp60 got into the mitochondria but failed to fold, identifying Hsp60 as a required chaperone.
Chaperones like Hsp60 prevent the formation of protein aggregates. Aggregation can occur in the intermediate stages of multidomain protein folding when hydrophobic regions might become exposed; chaperones protect these hydrophobic regions through multiple rounds of binding and releasing the partially folded proteins.
ATP binding and hydrolysis often mediate these bind-and-release cycles. The chaperones provide a safe space for the proteins to fold, sequestered away from the hubbub of the cytoplasm. Proteins revisit the quiet chambers that chaperones provide throughout their lifetimes, not only as they are being synthesized.
In the current model, while an amino acid chain is being translated, it interacts with a nascent-chain-binding protein like Hsp70, a type of chaperone that binds to hydrophobic peptide segments. Hsp70 prevents premature misfolding, only allowing the protein to fold when enough structural information for productive folding becomes available — when the protein chain gets long enough.
Most proteins only require this type of chaperone to fold efficiently. But some have more complicated structures and need to fold in the isolated, constrained cage of a cylindrical chaperonin complex like Hsp60, the chaperone that Hartl and Horwich first isolated from mitochondria. Bacterial GroEL and its cofactor GroES are the most well-studied of this class of chaperones; the eukaryotic cytoplasmic versions are called TRiC or CCT.
Chaperones are only one facet of cellular regulation of proteostasis, or protein quality control. They prevent proteins from misfolding, and the degradation machinery eliminates proteins that do not misfold.
There is an age-dependent decline in chaperone function, though. Since chaperones are required for protein maintenance, this decline can lead to a buildup of protein aggregates — which then further strains the already declining chaperones.
These protein aggregates lead to neurodegenerative diseases like Alzheimer’s disease and Huntington’s disease. Aggregates of different disease proteins have the same amyloid fibrillar structure, which suggests that a basic pathological mechanism may underlie all of these diseases. Hartl found that the aggregates interfere with almost every aspect of cellular machinery — transcription, translation, nuclear translocation, DNA maintenance, protein degradation, cytoskeletal organization, and vesicle transport —not only chaperones. But as they overwhelm the chaperone system, toxic aggregates build up until they cause cell death.
Thus, he suggests that rebalancing the proteostasis network may be a means of treating these neurodegenerative diseases.
Chaperonin-mediated Protein Folding
Arthur Horwich described how, in a classic bedside-to-bench approach, he discovered that chaperonin ring machines function to mediate protein folding. He studied the lethal X linked inherited metabolic disease caused by the mutant mitochondrial enzyme OTC. OTC is the second step in the urea cycle; when it is defective, cells can’t clear urea.
Since it is X linked, baby boys with nonfunctional OTC die. Horwich isolated the OTC cDNA and found its mitochondrial transport signal, then looked for a yeast mutant that could transport unfolded human OTC into the mitochondria but in which the transported OTC would not then fold. The yeast mutant he found lacked Hsp60.
Mitochondrial Hsp60, and its bacterial counterpart GroEL, performs two vital functions: they bind to polypeptides to prevent the formation of protein aggregates, and they help polypeptides achieve their functional state. In 1994 and 1997, the X-ray structures of both GroEL alone and in complex with its cochaperonin single ring GroES were presented along with structure-function studies in collaborative work with the late Paul Sigler, providing insight into how the machinery works.
The Binding of GroES to one end of the GroEL cylinder widely expands the folding chamber, giving the substrate space to fold in isolation from the busy cytosolic environment.
GroEL is a cylinder made of 14 identical subunits arranged into two back-to-back 7-membered rings. Each of the subunits is folded into: an equatorial domain, at the waistline of the cylinder, the collective of which hold the assembly together via side-by-side contacts within a ring and contacts of subunits between the two rings; a hinge like “intermediate” domain interconnecting the equatorial and apical domain; and a terminal “apical” domain at an end of the cylinder.
The equatorial domains each house an ATP binding pocket at the inside aspect and the cooperative binding of 7 ATP’s in a GroEL ring causes the terminal GroEL apical domains, attached to the equatorial domains through the slender intermediate domains, to open up like flower petals. In their “unopened” position the apical domains surround an open central cavity of 45 Angstrom diameter and each apical domain proffers sticky “hydrophobic” surface at its cavity-facing aspect.
The continuous hydrophobic surface around the ring specifically captures an unfolded protein species via its own exposed hydrophobic surface (that will become buried to the interior in the final folded “native” form). Thus the binding of a non-native protein by an open GroEL ring serves to capture the protein’s sticky hydrophobic surfaces, masking them, and preventing them from interacting with other unfolded proteins which can lead to aggregation.
When a polypeptide-bound ring of GroEL binds the cochaperonin ring, GroES, a smaller 7-membered single ring of identical subunits, in the presence of ATP, now a large movement of the apical domains occurs, both clockwise rotation and further elevation (see Figure; GroES is colored gold and the GroEL ring undergoing large movements is green). The large movements remove the hydrophobic polypeptide binding surface from facing the cavity, and the lining of the now GroES-encapsulated GroEL cavity becomes watery (hydrophilic) in character.
The large twisting apical domain movements strip the polypeptide off of the cavity wall into the now encapsulated and watery (hydrophilic) cavity where the protein folds in “solitary confinement,” as Horwich phrased it, without any chance of aggregation. Subsequently, after this longest step of the reaction cycle (~10 sec), ATP hydrolyzes, GroES releases, and out from the cavity comes the polypeptide whether properly folded or not. If it has not reached native form, it can make another try at proper folding, either by entering another GroEL cavity, or becoming bound to a different chaperone.
Andrew Dillin University of California, Berkeley and Howard Hughes Medical Institute
Highlights
There are a considerable variety of chaperones that are structurally and functionally different from recognizing and binding nonnative proteins in all of their various stages and processes.
The endoplasmic reticulum unfolded protein response evolved to protect the organism from infection. In the nervous system, it can act in a non-autonomous manner to promote transcription in response to stress.
The TRiCKy Business of Folding Proteins in the Cell
“Proteins are astoundingly complex,” said Judith Frydman. As an example, she pointed to the mammalian respiratory complex I, the 45-subunit complex that drives protons across the inner mitochondrial membrane. Thus, the potential problems with protein folding are not limited to the folding process.
Chaperones bind unfolded polypeptides to help them achieve their native state. Still, much more than that, they engage polypeptides at every stage of their existence in the cell, waiting to receive them as they’re translated and monitoring for damage throughout their lifespans.
TRiC, or CCT, is the stacked chaperone in eukaryotic cells — the equivalent of GroEL. However, unlike GroEL, it does not have a separate cap. It requires ATP hydrolysis, which closes the lid to allow folding; but ATP binding is not sufficient. TRiC binds nascent chains when they are almost complete, while they are still on the ribosome but after they have interacted with Hsp70.
The complex only binds precise types of folding intermediates — notably those with complex topologies like p53, tubulin, actin, telomerase, F box proteins, and others — and then comes off once that folding intermediate has resolved into its properly folded domain. It also suppresses amyloid aggregation, but is overexpressed in many cancers and has been linked to poor prognosis in lung and breast cancer.
Subunit diversity confers unique molecular features to TRiC-mediated folding.
TRiC descends from the chaperone in archaea, which only has one type of subunit. The heteromeric nature of eukaryotic TRiC allows it to form an asymmetrical complex. TRiC has eight subunits, and each subunit has a different affinity for ATP; these subunits are arranged with high-affinity subunits around one side of the ring and low-affinity subunits around the other side.
The subunits have varying degrees of affinity for substrates as well, with each subunit’s binding site presenting a distinct and evolutionarily conserved surface of polar and hydrophobic residues. Their combination thus broadens TRiC’s binding specificity.
Once the binding chamber is closed, one hemisphere is positively charged and the other is negatively charged, further orienting how the substrate can bind and influencing its folding trajectory. Frydman called it a “chaperone with an opinion,” rather than a cage, “that guides the substrate where it needs to go.”
Prefoldin is a cofactor for TRiC, so named because it was thought to facilitate substrate transfer to TRiC before the substrate folded. It binds to TRiC in TRiC’s open state, and, like TRiC, it has a charge asymmetry and a specific pattern of polar and hydrophobic residues that contribute to the inner surface of TRiC’s binding chamber. Prefoldin seems to enhance both the yield and the rate of folding. In vivo, it must bind to TRiC, or else massive protein aggregation builds up in the cell.
Perceiving ER Stress
As many as thirteen million proteins fold and mature in the endoplasmic reticulum (ER) every minute. It is no wonder then that defects in ER function are strongly associated with metabolic and age-related disorders. The unfolded protein response in the ER (UPRER) responds to the presence of unfolded proteins by inducing the transcription of chaperones, and it declines with age. Andrew Dillin wondered how this UPRER works in multicellular organisms.
Are unfolded proteins detected in each individual cell by its own machinery, in a stochastic manner? Or might there be a higher order of regulation, coordinating protein folding mechanisms across the whole system? He turned to C. elegans to figure it out. Since all of the cells in the adult C. elegans are post mitotic, the worm provides a great model system for studying proteome maintenance.
The Dillin lab demonstrated that the neuronal transcription factor XBP-1 could rescue the age-dependent decline in ER proteostasis. Overexpression of XBP-1 extends the worm’s life. XBP-1 — which has the very unusual property that its mRNA is spliced in the cytoplasm instead of the nucleus — senses unfolded proteins and induces the UPRER in nerve cells. These nerves then send signals to peripheral and distal cells, causing them to activate their own UPRER.
Only neuronal cells, both neurons and glia, respond to XBP by inducing the UPR. The peripheral cells don’t sense the unfolded proteins and respond to them; they respond to the signal from the brain. Neurons require small, clear vesicles to send this signal, indicating that neurotransmitters are involved. Unlike neurons, glia need dense core vesicles, suggesting that they signal through neuropeptides or biologic amines rather than neurotransmitters. The neuronal and glial effects are synergistic, and the mechanism is conserved in mice.
XBP-1 induces the UPR from both neurons and glia, but uses different pathways to signal from the different cell types.
The UPRER “only deals with the challenge after the damage has occurred” said Dillin. Wouldn’t a protective system be preferable?
Thus, he conducted a CRISPR screen to find such a system, of UPRER regulators that would identify and protect the organism from ER stress instead of just responding after it happens. In doing so, Dillin found TMEM2, a transmembrane hyaluronidase that had not been previously implicated in ER stress. It does not activate the UPRER, which can induce apoptosis. Rather, it acts through the MAP kinase pathway to promote stress resistance in the ER and survival of the organism.
By breaking down extracellular hyaluronan, it generates a smaller product that increases ER stress resistance. TMEM2 is conserved from worms all the way through humans; it senses the stress from outside the plasma membrane of brain cells, before the stress hits, and then sends the signal to the periphery. Dillin does not yet know how TMEM protects the ER from stress, but he knows that it is not through chaperones.
Franz-Ulrich Hartl Max Planck Institute of Biochemistry
Arthur Horwich Yale School of Medicine and Howard Hughes Medical Institute
Lila M. Gierasch University of Massachusetts Amherst
David S. Bredt Janssen Pharmaceutical Companies of Johnson & Johnson
Seema Kumar (Moderator) Johnson & Johnson
Highlights
The Hsp70 allosteric cycle involves major conformational changes, alternating between a docked state with bound ATP and low affinity for unfolded protein substrates and an undocked state in which the α-helical lid rotates out of the way to allow substrate binding and ATP hydrolysis.
Receptors implicated in neuronal and psychiatric disorders often require specific chaperones to help them fold; these chaperones are often expressed only in specific areas of the brain, and thus may provide appropriate drug targets.
The Versatile Hsp70 Molecular Chaperones Machine
Lila Gierasch introduced Hsp70 as the “early greeting committee” for nascent polypeptide chains. It can maintain the chains in an unfolded state for transport across membranes and meet them on the other side. Hsp70 can also give them a second chance to fold if things don’t go right the first time around. Like all chaperones, it prevents aggregation. It acts as a monomer, but that hardly makes it simple.
Hsp70 activities depend on intramolecular allostery controlled by ligand modulation of an energy landscape. The C-terminal substrate-binding domain (SBD) binds to short hydrophobic stretches of a polypeptide chain. ATP binding to the N-terminal nucleotide-binding domain (NBD) reorients the NBD actin fold. It decreases the affinity of the SBD for the substrate, and the substrate activates the NBD ATPase activity. The α-helical lid can rotate, allowing access to either the SBD or the NBD.
Hsp70 shifts between a docked, ATP bound state with low substrate affinity and an undocked, ADP bound state with high substrate affinity.
Hsp70 allosteric landscapes can be shaped by the strength of interdomain interfaces and as well as ligand binding, making them “tunable molecular machines.” They must have promiscuous selectivity because they bind an immense number of substrates with varying affinities.
There are Hsp70 molecules bound approximately every 40 amino acids throughout the proteome, and there is evidence that more than one Hsp70 molecule can bind to one substrate, mainly to keep it unfolded as it is translocated. And there are many isoforms of eukaryotic Hsp70 with different allosteries. These could have evolved through interactions with co-chaperones, post-translational modifications like phosphorylation, and even the sequence of the substrate.
Gierasch suggested that tweaking its allostery might modulate Hsp70 activity, or one class of Hsp70 could be targeted over another to treat particular diseases. It is tempting to think of activating the chaperone network to prevent neurodegeneration, but it is risky, too, since cancer cells often rely on mutant chaperones.
Getting a Handle on Neuropharmacology by Targeting Receptor Chaperones
Abnormalities in psychiatric diseases are heterogeneous across brain regions, with increased activity in some areas and decreased activity in others. It has been very difficult to find small molecules that can affect synaptic transmission in these different regions.
Stargazer mutant mice, that constantly look up because they have epilepsy, don’t have functional AMPARs (a type of glutamate receptor) on their cerebellar granule cells. David Brendt found that the receptors didn’t work because the mice lacked a chaperone he named stargazin. Stargazin is a Transmembrane AMPAR Regulatory Protein, or TARP, a family of proteins that Bredt said, “act more like escorts than chaperones.”
TARPs take the AMPARs from the endoplasmic reticulum to the cell surface at the synapse of cerebellar granule cells. Different TARPs are distributed to different brain regions, making them attractive drug targets. A molecule that disrupts the interaction between TARP-γ8 and AMPAR has been shown to inhibit neurotransmission in the hippocampus.
Thus, TARPs could be key to treating epilepsy without the terrible side effects of current anticonvulsants, and could possibly be used to treat bipolar disorder, schizophrenia, and anxiety.
Clinically relevant receptors that have been difficult to treat pharmacologically, like AMPAR and nAChRs, have specific required chaperones — TARPS and NACHO, in this case — that may provide more easily druggable targets.
Acetylcholine receptors are the site of action for a number of Alzheimer’s drugs that induce modest but reproducible improvements in cognition. These pentameric receptors have been very difficult to study in the lab, though, because they only fold properly in neuronal cells.
Bredt recognized this as an opportunity in addition to a challenge. His lab cotransfected a library of 4,000 transmembrane proteins along with the acetylcholine receptor into HEK cells and screened for any that would help the receptors fold. Only one did, a novel transmembrane protein with no homology to anything, found in one copy in mammals and Drosophila and not found in worms or yeast at all. They named it NACHO. It resides in the membrane of the endoplasmic reticulum in neuronal cells, and it mediates the folding of nicotinic acetylcholine receptors.
Panel Discussion
Highlights
We don’t know why protein aggregates are toxic, or why chaperones’ ability to prevent their formation wanes with age.
Future research should focus on understanding the proteostasis network in a physiological context and figuring out if, and how, it is an appropriate clinical target.
The day ended with a panel discussion in which Hartl and Horwich fielded questions. Many of them focused on the role misfolded proteins play in disease, why they accumulate with age, and if, when, and how the proteostasis machinery can be targeted therapeutically.
Moderator Seema Kumar began the panel by asking about the greatest challenges and limitations in the field. Horwich replied that we don’t understand the toxicity of misfolded proteins; we don’t even know if they themselves are toxic, or if they are recruiting other toxic mediators. He speculated that it would be great if we could monitor single polypeptide chains as they fold, to see which ones go astray and how that makes them toxic.
Since antibodies against amyloid plaques have been ineffective in Alzheimer’s disease, enhancing multiple parts of the proteostasis network might be a better strategy than targeting specific misfolded proteins or chaperones. Horwich also pointed out that we don’t know why aging thwarts chaperones: does their ability to handle their task decline, or are there genomic or proteomic issues? Hartl added that we don’t understand neurodegenerative diseases nearly well enough to know the role that protein folding plays in their development; Parkinson’s disease, for instance, is likely more than one monolithic disease.
As for how the field will unfold in the future, Horwich noted that most of what we know about protein folding mechanisms comes from in vitro studies with purified components. So we need to know more about how the cellular milieu affects binding affinities and folding. It would be helpful to determine how many times a particular ligand comes back to a particular chaperone. Hartl explained the importance of figuring out who the first responders are, who the next responders are, and if we can develop small molecules to affect the proteostasis machinery.
By Marie Gentile, Richard Birchard, and Mandy Carr
Speakers from left to right: Sam Parnia, MD, PhD (Director of Critical Care & Resuscitation Research at the NYU School of Medicine), Sarah Perman, MD (University of Colorado School of Medicine), Tom Aufderheide, MD, MS, FACEP, FACC, FAHA (Medical College of Wisconsin), Sonja Lyubomirsky, PhD (University of California, Riverside), and Stephan Mayer, MD, FCCM (Wayne State School of Medicine)
We see it in television dramas all the time—a patient in cardiac arrest is rushed into the ER after a severe traumatic injury or medical emergency, with a staff of medical professionals frantically performing CPR. Tension is high and doctors have to figure out how to save the person’s life. Beyond the theatrics of primetime drama, the field of medicine has been making major strides to reverse cardiac arrest and death.
In this video you’ll hear directly from top physicians and researchers who are at the cutting edge of resuscitation science. Moderated by Sam Parnia, this discussion brought together internationally-recognized researcher in emergency cardiac care, Tom Aufderheide; distinguished happiness research psychologist, Sonja Lyubomirsky; world expert in neurological intensive care Stephan Mayer; and Sarah Perman, a leader in resuscitation science and post-cardiac arrest care.
Meet the winning team of the 2019 Junior Academy Genomics Challenge.
Published October 18, 2019
By Marie Gentile, Richard Birchard, and Mandy Carr
According to the World Health Organization, there are 5,000 to 8,000 rare diseases, most of them with a genetic basis. But errors in diagnosis can delay the implementation of proper treatments, especially for those in poor areas of the world where access to healthcare is limited.
Now, six high school students who participated in the Junior Academy’s Genomics Challenge, sponsored by Regeneron and Medidata, have developed a prototype for a better way to test the genetic code and thereby improve the diagnosis of rare diseases.
The students (Evangelos Kassos, 18, from Karditsa Greece; Ana Stratan, 18, from Bucharest, Romania; Aditi Gupta, 18, from Delhi, India; Monish Singhal, 14, from Bengaluru, India; Athena Yao, 17, from Wantagh, New York, USA; and Ana Bonavides-Aguilar, 17, from Cuernavaca, Morelos, México) impressed the Challenge judges with their comprehensive four-step approach, which addressed rare disease diagnosis, access to consultation, patient privacy, and knowledge distribution.
An Innovative Approach
Their innovative “iDNA Protocol” utilizes blockchain technology to ensure patient privacy, while increasing data sharing across research entities through their Doc2Doc platform model. Better data sharing facilitates collaboration between researchers, doctors, and patients, leading to more efficient and personalized diagnosis and treatment.
A “Prion Detection Kit” will help patients identify neurodegenerative disorders through at-home urine tests. This early detection kit complements the “GenePack” testing and treatment protocol, which tests newborns for genetic diseases and connects people living in isolated areas with research centers.
For their solution, the team received an all-expenses-paid trip to New York City to attend the 2019 Global STEM Alliance Summit.
Here, the students share their thoughts on the project and why they’re excited about its potential impact on medically underserved communities:
“Most of all, we thought about who we could help. We fashioned our project to cater to the needs of underserved communities.”
Ana Stratan
Diverse Perspectives
“I had no idea what was waiting for me when I posted ‘Wanna be the next Watson?’ on Launchpad. Five amazing people from around the world joined me in taking on the Genomics Challenge,” explains Evangelos Kassos. “Along with our mentor, we created a fantastic space full of creativity, where we could all thrive.”
Multidisciplinary Focus
“All of us had a focus—biology, technology, informatics—and we thought about the Challenge through these different lenses. Most of all, we thought about who we could help. We fashioned our project to cater to the needs of underserved communities,” says Ana Stratan. “Periodically we asked for input from people outside of the project to better understand our target audience.”
People Aren’t Numbers
“Our mentor explained to us how dire situations could get. We realized that while everyone was looking at the numbers, no one was realizing that these numbers are people,” laments Aditi Gupta. “I have lived in both a first world country and a third world country. I’m thankful for having access to the American healthcare system because India is still developing theirs.”
A Diagnosis-Focused Solution
”We realized that treatment is a different problem. The mere diagnosis of the disease can be troublesome,” says Monish Singhal. “We spoke with Prasanna Shirol, the co-founder and board director of the Organization for Rare Diseases India (ORDI), whose daughter suffers from Pompe disease. His daughter was diagnosed inaccurately several times. This example led to our diagnosis-focused solution, which emphasizes early identification of a disease.”
“We realized that while everyone was looking at the numbers, no one was realizing that these numbers are people.”
A Unified Approach
“Our solution has the potential to improve lives and be implemented effectively in existing communities globally, in a cost-effective manner,” says Athena Yao. “Our approach involves changes in the rare disease diagnosis and treatment process, addressing the different aspects of the problem. We employed our knowledge, resources, and understanding of global perspectives to create a solution that is viable for various areas.”
Achievable Impact
”The ideas we are proposing are groundbreaking, innovative, and achievable,” concludes Ana Bonavides-Aguilar. “Even though some are more challenging to attain (like creating the iDNA Protocol) there are others that if research begins, they could change the way genetic diseases are being detected, like the Antibody Testing Kit. Therefore, people suffering from rare diseases could—and will—have a chance at a high quality of life.”
Want to tackle global problems like this one? Learn more about the Junior Academy.
Adequate intake of essential vitamins and minerals is critical for a healthy pregnancy. Unfortunately, many women in low- and middle-income countries (LMICs) struggle to meet the increased dietary demands for a healthy pregnancy through diet alone. Inadequate nutritional intake frequently leads to poor maternal health and adverse birth outcomes, such as maternal mortality; preeclampsia; insufficient gestational weight gain; stunting; low birth weight (LBW); small for gestational age (SGA); and neonatal mortality. Currently, the World Health Organization (WHO) recommends iron-folic acid supplements (IFA) as the routine standard of care in antenatal care programs. However, strong evidence is now available demonstrating the superiority of multiple micronutrient supplements (MMS) over IFA. To help countries determine if they should transition from IFA to MMS in antenatal care, the New York Academy of Sciences assembled a task force. Charged with taking a closer look at MMS, the task force considered several factors, including benefits, risks, and cost-effectiveness. On June 25, 2019, the task force’s findings were presented at the launch of the Special Issue, published in the Annals of the New York Academy of Sciences.
Highlights
Data from the 2019 Cochrane Review and the 2017 individual patient data (IPD) meta-analysis demonstrate that MMS has significant added benefits to birth outcomes compared with IFA.
The task force concluded that countries where nutritional deficiencies are prevalent should consider MMS, as it is a cost-effective and safe alternative to IFA.
The MMS technical advisory group is translating this evidence into practice by assisting in the rollout of MMS demonstration projects in several countries.
When compared to IFA, routine MMS supplementation does not increase the risk of adverse effects.
During pregnancy, the risk of exceeding the UL with a micronutrient-rich diet and daily micronutrient supplementation is very low.
Speakers
Robert E. Black, MD, MPH Johns Hopkins University
Megan Bourassa, PhD The New York Academy of Sciences
Gilles Bergeron, PhD The New York Academy of Sciences
Emily R. Smith, ScD, MPH The Bill & Melinda Gates Foundation and Harvard T.H. Chan School of Public Health
Alison Gernand, PhD Penn State University
Reina Engle-Stone, PhD University of California, Davis
Sponsors
For Policy Makers and Program Implementers
Speakers
Robert E. Black, MD, MPH Johns Hopkins University
Gilles Bergeron, PhD The New York Academy of Sciences
Megan Bourassa, PhD The New York Academy of Sciences
Micronutrient Status and the Benefits of MMS on Birth Outcomes
Robert Black discussed the benefits of MMS on birth outcomes. While the 2016 WHO antenatal care guidelines recommend IFA for routine use, the guidelines also state that countries “might consider the benefits of MMS on maternal health to outweigh the disadvantages and may choose to give MMS that include iron and folic acid.” New evidence on MMS has since emerged, and after a thorough review, the Academy’s task force found strong research in support of prenatal MMS. The data showed a high prevalence of multiple micronutrient deficiencies in women of reproductive age (WRA) and pregnant women in LMICs, suggesting that these women could significantly benefit from MMS during pregnancy. A Cochrane review (updated in 2019) demonstrated that MMS was superior to IFA in reducing important adverse birth outcomes, including small for gestational age (SGA) and low birth weight (LBW).
Micronutrient deficiencies among WRA not only exist in LMIC, but in women around the world.
An IPD meta-analysis of several MMS trials conducted in pregnant women provides additional evidence in support of prenatal MMS. Published after the WHO antenatal care guidelines, the analysis showed that women receiving MMS, compared with those receiving IFA, had a significant reduction of SGA and LBW births, very low birth weight (VLBW) births, preterm births, and very preterm births. It also identified a number of subgroups that benefitted from MMS. Additionally, women who were underweight at the onset of pregnancy had a greater reduction in preterm births. Given that complications from preterm births are the leading cause of death in children under five years of age in LMICs, Black stressed the significance of these findings that highlight the potential benefits of MMS and the substantive effects that it can have on birth outcomes. Ultimately, Black concluded that the data from both systematic reviews suggest that countries with high rates of nutritional deficiencies should consider the switch from prenatal IFA to MMS.
Task Force Conclusions and Guidance on MMS in Pregnancy
Megan Bourassa explained that during their review of the evidence, the task force took a closer look at the prevalence of micronutrient deficiencies, cost-effectiveness, and the safety of MMS. They concluded that populations with a high prevalence of nutritional deficiencies might have a greater benefit from MMS. The task force also found that MMS is highly cost-effective in comparison to other antenatal care interventions, such as micronutrient fortification or balanced protein energy supplementation for pregnant women. And after examining the safety considerations, they found no serious side effects associated with the use of MMS. Thus, they concluded that MMS is a cost-effective and safe alternative to IFA, and should especially be considered by countries where nutritional deficiencies are prevalent.
The task force outlined a few questions for countries to consider when making their decision on whether or not to switch from IFA to MMS. The first question is whether the country has a high prevalence of nutritional deficiencies, said Bourassa. Since the WHO did not explain how to define a nutrient deficiency, the task force suggested a list of indicators that might be useful to consider, such as dietary intake, underweight prevalence, and biomarker data, among others. Countries can use these indicators to compile and assess available data to decide whether there is sufficient evidence to make the switch.
To successfully transition from IFA to MMS, countries should consider several factors during the planning process. First, MMS should be built into the existing antenatal care program rather than creating a standalone intervention. Second, policymakers should consider taking the opportunity to assess and strengthen their respective antenatal care programs, including the coverage and adherence to supplementation. If the current program has inadequate coverage, MMS likely will not reach the target population, thus yielding insubstantial results. Countries may also want to consider taking on a small demonstration project to test this in a smaller region to identify any potential issues with the supply and distribution chain. Lastly, as with all public health interventions, it is essential to develop a monitoring and evaluation system to ensure the continued coverage and success of a prenatal MMS intervention.
The Future Direction of the Task Force
Since the release of the Special Issue, the task force has made strides in translating evidence into policy and practice in real world-settings, said Gilles Bergeron. For example, a Technical Advisory Group (TAG) on MMS was formed this year to spearhead the development of a series of technical reference materials. The materials are designed to provide countries with more information on MMS and assist interested countries with the transition from IFA to MMS, and much more. Currently, the TAG is in the process of using the Child Health and Nutrition Research Initiative (CHNRI) methodology to inform the direction of research and investments needed to support the implementation of MMS interventions for pregnant women in LMICs. Bergeron also discussed future directions of the TAG, specifically its partnership with UNICEF and multiple stakeholders, to promote the rollout of MMS through demonstration activities in four countries—Bangladesh, Madagascar, Tanzania, and Burkina Faso—as well as in other potential countries considering the switch.
For Research Scientists and Clinicians
Speakers
Emily R. Smith, ScD, MPH The Bill & Melinda Gates Foundation and Harvard T.H. Chan School of Public Health
Reina Engle-Stone, PhD University of California, Davis
Alison Gernand, PhD Penn State University
Clinical Trials, MMS Adherence, and Adverse Birth Outcomes
The second session focused primarily on information for researchers and clinicians. Emily Smith took a closer look at the results of the clinical trials and discussed the available evidence on side effects and adherence. Her presentation aimed to answer a key question: Is MMS is better than IFA alone for ensuring a positive pregnancy experience? Smith shared results from the most recent and comprehensive reviews on MMS, specifically the 2019 Cochrane Review and the 2017 IPD meta-analysis. The recently updated Cochrane Review evaluated the effects of MMS compared with IFA on pregnancy outcomes, using a total of 20 clinical trials with data from over 140,000 women. Findings showed that MMS resulted in a 12% reduction in LBW and an 8% reduction in SGA births, compared with IFA. While the Cochrane review focused on the overall effects of all available trials, the IPD meta-analysis was primarily aimed at conducting subgroup analyses. This meta-analysis included data from 17 randomized controlled trials from over 100,000 pregnancies in LMICs and found that MMS not only reduces the risk of SGA and LBW, but also reduces the risk of stillbirth, very LBW, early preterm birth, and preterm birth when compared with IFA. The findings from the IPD meta-analysis—26 subgroup analyses were conducted to identify individual characteristics that may further modify the effect of MMS—also showed specific subgroups have a greater benefit from MMS. When compared with IFA, the effects of MMS resulted in a more significant benefit for undernourished women, specifically those who were anemic or underweight (BMI <18.5 kg/m2) or women who gave birth to female infants.
The WHO antenatal care guidelines raised an important point of concern regarding the potential risk of increased neonatal mortality. This concern arose from a subgroup analysis comparing those receiving MMS with 30mg of iron to those in the control group receiving IFA with 60mg of iron. When reviewing the analysis, it was apparent that a few errors and omissions were made. A recent reanalysis of these data, performed by Sudfeld and Smith, included all eligible studies and corrected point estimates and found no increased risk of neonatal mortality associated with MMS. Though limited evidence was available, six of the seven clinical trials (which reported on this outcome) showed no significant differences in the side effects between IFA and MMS. Similarly, differences in adherence rates between IFA and MMS were minimal, with no more than a 2% difference between the intervention groups in 10 trials that reported on adherence. Smith concluded that routine MMS supplementation does not increase the risk of adverse effects, and has a number of additional benefits for mortality and birth outcomes compared with IFA, especially in areas where nutritional deficiencies exist.
The Upper Level: Antenatal Supplements and the Risk of Excess Micronutrient Intake
While understanding the global prevalence of micronutrient deficiencies in LMICs and the substantial benefit MMS can provide to alleviate the burden, there can be health risks when intake regularly exceeds a high amount of nutrients, otherwise known as the upper intake level (UL). Alison Gernand outlined what is known about these risks in pregnancy. The WHO defines UL as the “maximum intake from food, water, and supplements that is unlikely to pose the risk of adverse health effects”. It is important to note that the UL values are set for healthy people with good baseline micronutrient status, not for those with deficiencies or medical conditions. Since the prevalence of deficiencies is high in LMICs countries, an intake higher than the UL may be warranted for a limited timeframe to correct the deficits. Little is known about pregnancy-specific risks, so the ULs are the same for pregnant and non-pregnant women, except vitamin A, due to the possibility of birth defects. In general, there is little to no risk of excessive intake for several vitamins—including thiamin, riboflavin, vitamin B12, and vitamin C—from large supplemental doses. Potential adverse effects from excess micronutrients such as niacin, folate, and iron are only due to supplement intake.
Potential adverse effects from daily supplement intake include an excess of niacin, folic acid, and iron.
To assess the risk of reaching the UL with an adequate diet, Gernand compared the Reference Daily Intake (RNI) or Recommended Dietary Allowance (RDA), and compared the amount in the UNIMMAP supplement to both the Institute of Medicine (IOM) and WHO UL values. The results showed that folate intake reached the UL, while iron and niacin slightly exceeded it, with known risks of each nutrient to be mild. For folate, an excess can mask vitamin B12 deficiency; otherwise, toxicity due to excess intake has not been known. Risks due to excess iron intake, specifically nausea and vomiting, can be eliminated if the supplement is taken with food. Finally, for niacin, the risk of flushing resulting in skin reddening and itchiness is due to nicotinic acid, found only in supplements, not in food. Gernand said that limited information on pregnancy-specific risk from excess intake is available, stressing the urgency for more published data. Overall, the risks of exceeding the UL during pregnancy from a micronutrient rich diet and daily MMS are very low and should not result in adverse effects.
Cost Analyses: Replacing IFA with MMA During Pregnancy
According to new evidence compiled by the task force, MMS has additional benefits over IFA, but the tablets are more costly. While there is sufficient evidence to support the transition of IFA to MMS, policymakers need to consider not just the benefits, but also the associated costs. In her presentation, Reina Engle-Stone asked if MMS is a worthwhile investment. With her team at UC Davis, Engle-Stone developed a model to estimate the effects, cost, and cost-effectiveness of replacing IFA with MMS within the context of a supplementation distribution program in Bangladesh and Burkina Faso. A hypothetical one-year scenario with 100% coverage was also applied to both countries using their current national levels of IFA coverage, assuming complete adherence to the recommended regimen (i.e., consumption of 180 supplements per pregnancy). The model used baseline demographic characteristics from the Lives Saved Tool (LiST) and effect sizes from the IPD meta-analysis to generate the marginal effects of replacing IFA with MMS on mortality, adverse birth outcomes, and disability-adjusted life years (DALYs) averted, in both rural and urban settings.
A team at UC Davis created a model structure to calculate the cost effectiveness of MMS in the context of an ongoing supplement distribution program.
The results showed replacing IFA with MMS could avert over 15,000 deaths and 30,000 cases of preterm birth annually in Bangladesh, and over 5,000 deaths and 5,000 cases of preterm birth in Burkina Faso, assuming 100% coverage and adherence. The cost per death averted was estimated to be $175-$185 in Bangladesh and $112-$125 in Burkina Faso. Lastly, the cost per DALY averted ranged from $3-$15, depending on the country and consideration of sub-groups. Engle-Stone noted that the estimate is very sensitive to the cost of the tablet. For one, the costs associated with shifting from IFA to MMS will be significant, given that MMS are approximately 35% more costly than IFA tablets. Based on the hypothetical scenario, a complete switch to MMS in Bangladesh given current coverage levels (50% nationally) would cost approximately $1.7 million. In a scenario assuming 100% coverage, where all women receive and consume 180 tablets, the additional cost to replace the IFA with MMS would increase to $2.7 million. A complete switch in Burkina Faso with current coverage levels (10.2% nationally) would cost approximately $60,000 and would rise to $600,000 for 100% coverage.
In sum, the switch would come at an added cost, and if the cost of the supplement rises, so will the cost-effectiveness. However, an increase in demand of MMS with improvements in program delivery and supplement adherence could improve the cost-effectiveness. Engle-Stone noted that further research is needed to provide a more realistic scenario for the transition from IFA to MMS, specifically on the delivery platform performance and supplement adherence. Nonetheless, the cost-effectiveness of this short, one-year analysis suggests that policymakers should consider adopting the underlying model with necessary modifications to fit their context and use it to better inform policy discussions around the shift from IFA to MMS.
The New York Academy of Sciences and the Blavatnik Family Foundation hosted the annual Blavatnik Science Symposium on July 15–16, 2019, uniting 75 Finalists, Laureates, and Winners of the Blavatnik Awards for Young Scientists. Honorees from the UK and Israel Awards programs joined Blavatnik National and Regional Awards honorees from the U.S. for what one speaker described as “two days of the impossible.” Nearly 30 presenters delivered research updates over the course of nine themed sessions, offering a fast-paced peek into the latest developments in materials science, quantum optics, sustainable technologies, neuroscience, chemical biology, and biomedicine.
Symposium Highlights
Computer vision and machine learning have enabled novel analyses of satellite and drone images of wildlife, food crops, and the Earth itself.
Next-generation atomic clocks can be used to study interactions between particles in complex many-body systems.
Bacterial communities colonizing the intestinal tract produce bioactive molecules that interact with the human genome and may influence disease susceptibility.
New catalysts can reduce carbon emissions associated with industrial chemical production.
Retinal neurons display a surprising degree of plasticity, changing their coding in response to repetitive stimuli.
New approaches for applying machine learning to complex datasets is improving predictive algorithms in fields ranging from consumer marketing to healthcare.
Breakthroughs in materials science have resulted in materials with remarkable strength and responsiveness.
Single-cell genomic studies are revealing some of the mechanisms that drive cancer development, metastasis, and resistance to treatment.
Speakers
Emily Balskus, PhD Harvard University
Chiara Daraio, PhD Caltech
William Dichtel, PhD Northwestern University
Elza Erkip, PhD New York University
Lucia Gualtieri, PhD Stanford University
Ive Hermans, PhD University of Wisconsin – Madison
Liangbing Hu, PhD University of Maryland, College Park
Jure Leskovec, PhD Stanford University
Heather J. Lynch, PhD Stony Brook University
Wei Min, PhD Columbia University
Seth Murray, PhD Texas A & M University
Nicholas Navin, PhD, MD MD Anderson Cancer Center
Ana Maria Rey, PhD University of Colorado Boulder
Michal Rivlin, PhD Weizmann Institute of Science
Nieng Yan, PhD Princeton University
Event Sponsor
Technology for Sustainability
Speakers
Heather J. Lynch Stony Brook University
Lucia Gualtieri Stanford University
Seth Murray Texas A & M University
Highlights
Machine learning algorithms trained to analyze satellite imagery have led to the discovery of previously unknown colonies of Antarctic penguins.
Seismographic data can be used to analyze more than just earthquakes—typhoons, hurricanes, iceberg-calving events and landslides are reflected in the seismic record.
Unmanned aerial systems are a valuable tool for phenotypic analysis in plant breeding, allowing researchers to take frequent measurements of key metrics during the growing season and identify spectral signatures of crop yield.
Satellites, Drones, and New Insights into Penguin Biogeography
Satellite images have been used for decades to document geological changes and environmental disasters, but ecologist and 2019 Blavatnik National Awards Laureate in Life Sciences, Heather Lynch, is one of the few to probe the database in search of penguin guano. She opened the symposium with the story of how the Landsat satellite program enabled a surprise discovery of several of Earth’s largest colonies of Adélie penguins, a finding that has ushered in a new era of insight into these iconic Antarctic animals.
Steady streams of high quality spatial and temporal data regularly support environmental science. In contrast, Lynch noted that wildlife biology has advanced so slowly that many field techniques “would be familiar to Darwin.” Collecting information on animal populations, including changes in population size or migration patterns, relies on arduous and imprecise counting methods. The quest for alternative ways to track wildlife populations—in this case, Antarctic penguin colonies—led Lynch to develop a machine learning algorithm for automated identification of penguin guano in high resolution commercial satellite imagery, which can be combined with lower resolution imagery like that coming from NASA’s Landsat program. Pairing measurements of vast, visible tracts of penguin guano—the excrement colored bright pink due to the birds’ diet—with information about penguin colony density yields near-precise population information. The technique has been used to survey populations in known penguin colonies and enabled the unexpected discovery of a “major biological hotspot” in the Danger Islands, on the tip of the Antarctic Peninsula. This Antarctic Archipelago is so small that it is doesn’t appear on most maps of the Antarctic continent, yet it hosts one of the world’s largest Adélie penguin hotspots.
Satellite images of the pink stains of Antarctic penguin guano have been used to identify and track penguin populations.
Lynch and her colleagues are developing new algorithms that utilize high-resolution drone and satellite imagery to create centimeter-scale, 3D models of penguin terrain. These models feed into detailed habitat suitability and population-tracking analyses that further basic research and can even influence environmental policy decisions. Lynch noted that the discovery of the Danger Island colony led to the institution of crucial environmental protections for this region that may have otherwise been overlooked. “Better technology actually can lead to better conservation,” she said.
Listening to the Environment with Seismic Waves
The study of earthquakes has dominated seismology for decades, but new analyses of seismic wave activity are broadening the field. “The Earth is never at rest,” said Lucia Gualtieri, 2018 Blavatnik Regional Awards Finalist, while reviewing a series of non-earthquake seismograms that show constant, low-level vibrations within the Earth. Long discarded as “seismic noise,” these data, which comprise more than 90% of seismograms, are now considered a powerful tool for uniting seismology, atmospheric science, and oceanography to produce a holistic picture of the interactions between the solid Earth and other systems.
In addition to earthquakes, events such as hurricanes, typhoons, and landslides are reflected in the seismic record.
Nearly every environmental process generates seismic waves. Hurricanes, typhoons, and landslides have distinct vibrational patterns, as do changes in river flow during monsoons and “glacial earthquakes” caused by ice calving events. Gualtieri illustrated how events on the surface of the Earth are reflected within the seismic record—even at remarkably long distances—including a massive landslide in Alaska detected by a seismic sensor in Massachusetts. Gualtieri and her collaborators are tapping this exquisite sensitivity to create a new generation of tools capable of measuring the precise path and strength of hurricanes and tropical cyclones, and for making predictive models of cyclone strength and behavior based on decades of seismic data.
Improving Crop Yield Using Unmanned Aerial Systems and Field Phenomics
Plant breeders like Seth Murray, 2019 Blavatnik National Awards Finalist, are uniquely attuned to the demands a soaring global population places on the planet’s food supply. Staple crop yields have skyrocketed thanks to a century of advances in breeding and improved management practices, but the pressure is on to create new strategies for boosting yield while reducing agricultural inputs. “We need to grow more plants, measure them better, use more genetic diversity, and create more seasons per year,” Murray said. It’s a tall order, but one that he and a transdisciplinary group of collaborators are tackling with the help of a fleet of unmanned aerial systems (UAS), or drones.
Drones facilitate frequent measurement of plant height, revealing variations between varietals early in the growth process.
Genomics has transformed many aspects of plant breeding, but phenotypic, rather than genotypic, information is more useful for predicting crop yield. Using drones equipped with specialized equipment, Murray has not only automated many of the time-consuming measurements critical for plant phenotyping, such as tracking height, but has also identified novel metrics that can accelerate the development of new varietals. Spectral signatures obtained via drone can be used to identify top-yielding varietals of maize even before the plants are fully mature. Phenotypic features distilled from drone images are also being used to determine attributes such as disease resistance, which directly influence crop management. Murray’s team is modeling the influence of thousands of phenotypes on overall crop performance, paving the way for true phenomic selection in plant breeding.
Quantum mechanics underlies the technologies of modern computing, including transistors and integrated circuits.
Most quantum insights are derived from studies of single quantum particles, but understanding interactions between many particles is necessary for the development of devices such as quantum computers.
Atoms cooled to one billionth of a degree above absolute zero obey the laws of quantum mechanics, and can be used as quantum simulators to study many-particle interactions.
Atomic Clocks: From Timekeepers to Quantum Computers
The discovery of quantum mechanics opened “a new chapter in human knowledge,” said 2019 Blavatnik National Awards Laureate in Physical Sciences & Engineering, Ana Maria Rey, describing how the study of quantum phenomena has revolutionized modern computing, telecommunications, and navigation systems. Transistors, which make up integrated circuits, and lasers, which are the foundation of the atomic clocks that maintain the precision of satellites used in global positioning systems, all stem from discoveries about the nature of quantum particles.
The next generation of innovations—such as room temperature superconductors and quantum computers—will be based on new quantum insights, and all of this hinges on our ability to study interactions between many particles in quantum systems. The complexity of this task is beyond the scope of even the most powerful supercomputers. As Rey explained, calculating the possible states for a small number of quantum particles (six, for example) is simple. “But if you increase that by a factor of just 10, you end up with a number of states larger than the number of stars in the known universe,” she said.
Calculating the number of possible states for even a small number of quantum particles is a task too complex for even the most powerful supercomputer.
Researchers have developed several experimental platforms to clear this hurdle and explore the quantum world. Rey shared the story of how her work developing ultra-precise atomic clocks inadvertently led to one experimental platform that is already demystifying some aspects of quantum systems.
Atomic clocks keep time by measuring oscillations of atoms—typically in cesium atoms—as they change energy levels. Recently, Rey and her collaborators at JILA built the world’s most sensitive atomic clock using strontium atoms instead of cesium and using many more atoms that are typically found in these clocks. The instrument had the potential to be 1,000 times more sensitive than its predecessors, yet collisions between the atoms compromised its precision. Rey explained that by suppressing these collisions, their clock became “a window to explore the quantum world.” Within this framework, the atoms can be manipulated to simulate the movement and interactions of quantum particles in solid-state materials. Rey reported that this clock-turned-quantum simulator has already generated new findings about phenomena including superconductivity and quantum magnetism.
The human gut is colonized by trillions of bacteria that are critical for host health, yet may also be implicated in the development of diseases including colorectal cancer.
For over a decade, chemists have sought to resolve the structure of a genotoxin called colibactin, which is produced by a strain of E. coli commonly found in the gut microbiome of colorectal cancer patients.
By studying the specific type of DNA damage caused by colibactin, researchers found a trail of clues that led to a promising candidate structure of the colibactin molecule.
Gut Reactions: Understanding the Chemistry of the Human Gut Microbiome
The composition of the trillions-strong microbial communities that colonize the mammalian intestinal tract is well characterized, but a deeper understanding of their chemistry remains elusive. Emily Balskus, the 2019 Blavatnik National Awards Laureate in Chemistry, described her lab’s hunt for clues to solve one chemical mystery of the gut microbiome—a mission that could have implications for colorectal cancer (CRC) screening and early detection.
Some commensal E. coli strains in the human gut produce a genotoxin called colibactin. When cultured with human cells, these strains cause cell cycle arrest and DNA damage, and studies have shown increased populations of colibactin-producing E. coli in CRC patients. Previous studies have localized production of colibactin within the E. coli genome and hypothesized that the toxin is synthesized through an enzymatic assembly line. Yet every attempt to isolate colibactin and determine its chemical structure had failed.
Balskus’ group took “a very different approach,” in their efforts to discover colibactin’s structure. By studying the enzymes that make the toxin, the team uncovered a critical clue: a cyclopropane ring in the structure of a series of molecules they believed could be colibactin precursors. This functional group, when present in other molecules, is known to damage DNA, and its detection in the molecular products of the colibactin assembly line led the researchers to consider it as a potential mechanism of colibactin’s genotoxicity.
In collaboration with researchers at the University of Minnesota School of Public Health, Balskus’ team cultured human cells with colibactin-producing E. coli strains as well as strains that cannot produce the toxin. They identified and characterized the products of colibactin-mediated DNA damage. “Starting from the chemical structure of these DNA adducts, we can work backwards and think about potential routes for their production,” Balskus explained.
A proposed structure for the genotoxin colibactin, which is associated with colorectal cancer, features two cyclopropane rings capable of interacting with DNA to generate interstrand cross links, a type of DNA damage.
Further studies revealed that colibactin triggers a specific type of DNA damage that requires two reactive groups—likely represented by two cyclopropane rings in the final toxin structure—a pivotal discovery in deriving what Balskus believes is a strong candidate for the true colibactin structure. Balskus emphasized that this work could illuminate the role of colibactin in carcinogenesis, and may lead to cancer screening methods that rely on detecting DNA damage before cells become malignant. The findings also have implications for understanding microbiome-host interactions. “These studies reveal that human gut microbiota can interact with our genomes, compromising their integrity,” she said.
The chemical industry is a major producer of carbon dioxide, and efforts to create more efficient and sustainable chemical processes are often stymied by cost or scale.
Boron nitride is not well known as a catalyst, yet experiments show it is highly efficient at converting propane to propylene—one of the most widely used chemical building blocks in the world.
Two-dimensional polymers called covalent organic frameworks (COFs) can be used for water filtration, energy storage, and chemical sensing.
Until recently, researchers have struggled to control and direct COF formation, but new approaches to COF synthesis are advancing the field.
Boron Nitride: A Surprising Catalyst
Industrial chemicals “define our standard of living,” said Ive Hermans, 2019 Blavatnik National Awards Finalist, before explaining that nearly 96% of the products used in daily life arise from processes requiring bulk chemical production. These building block molecules are produced at an astonishingly large scale, using energy-intensive methods that also produce waste products, including carbon dioxide.
Despite pressure to reduce carbon emissions, the pace of innovation in chemical production is slow. The industry is capital-intensive — a chemical production plant can cost more than $2 billion—and it can take a decade or more to develop new methods of synthesizing chemicals. Concepts that show promise in the lab often fail at scale or are too costly to make the transition from lab to plant. “The goal is to come up with technologies that are both easily implemented and scalable,” Hermans said.
Catalysts are a key area of interest for improving chemical production processes. These molecules bind to reactants and can boost the speed and efficiency of chemical reactions. Hermans’ research focuses on catalyst design, and one of his recent discoveries, made “just by luck,” stands to transform production of one of the most in-demand chemicals worldwide—propylene.
Historically, propylene was one product (along with ethylene and several others) produced by “cracking” carbon–carbon bonds in naphtha, a crude oil component that has since been replaced by ethane (from natural gas) as a preferred starting material. However, ethane yields far less propylene, leaving manufacturers and researchers to seek alternative methods of producing the chemical.
Boron nitride catalyzes a highly efficient conversion of propane to propylene.
Enter boron nitride, a two-dimensional material whose catalytic properties took Hermans by surprise when a student in his lab discovered its efficiency at converting propane, also a component of natural gas, to propylene. Existing methods for running this reaction are endothermic and produce significant CO2. Boron nitride catalysts facilitate an exothermic reaction that can be conducted at far cooler temperatures, with little CO2 production. Better still, the only significant byproduct is ethylene, an in-demand commodity.
Hermans sees this success as a step toward a more sustainable future, where chemical production moves “away from a linear economy approach, where we make things and produce CO2 as a byproduct, and more toward a circular economy where we use different starting materials and convert CO2 back into chemical building blocks.”
Polymerization in Two Dimensions
William Dichtel, a Blavatnik National Awards Finalist in 2017 and 2019, offered an update from one of the most exciting frontiers in polymer chemistry—two-dimensional polymerization. The synthetic polymers that dominate modern life are comprised of linear, repeating chains of linked building blocks that imbue materials with specific properties. Designing non-linear polymer architectures requires the ability to precisely control the placement of components, a feat that has challenged chemists for a decade.
Dichtel described the potential of a class of polymers called covalent organic frameworks, or COFs—networks of polymers that form when monomers are polymerized into well-defined, two-dimensional structures. COFs can be created in a variety of topologies, dictated by the shape of the monomers that comprise it, and typically feature pores that can be customized to perform a range of functions. These materials hold promise for applications including water purification membranes, energy and gas storage, organic electronics, and chemical sensing.
Dichtel explained that COF development is a trial and error process that often fails, as the mechanisms of their formation are not well understood. “We have very limited ability to improve these materials rationally—we need to be able to control their form so we can integrate them into a wide variety of contexts,” he said.
Two-dimensional polymer networks can be utilized for water purification, energy storage, and many other applications, but chemists have long struggled to understand their formation and control their structure.
A breakthrough in COF synthesis came when chemist Brian Smith, a former postdoc in Dichtel’s lab, discovered that certain solvents allowed COFs to disperse as nanoparticles in solution rather than precipitating as powder. These particles became the basis for a new method of growing large, controlled crystalline COFs using nanoparticles as structural “seeds,” then slowly adding monomers to maximize growth while limiting nucleation. “This level of control parallels living polymerization, with well-defined initiation and growth phases,” Dichtel said.
More recently, Dichtel’s group has made significant advances in COF fabrication, successfully casting them into thin films that could be used in membrane and filtration applications.
Further Readings
Hermans
Zhang Z, Jimenez-Izal E, Hermans I, Alexandrova AN.
The 80 subtypes of retinal ganglion cells each encode different aspects of vision, such as direction and motion.
The “preferences” of these cells were believed to be hard-wired, yet experiments show that retinal ganglion cells can be reprogrammed by exposure to repetitive stimuli.
Sodium ion channels control electrical signaling in cells of the heart, muscles, and brain, and have long been drug targets due to their connection to pain signaling.
Cryo-electron microscopy has allowed researchers to visualize Nav 7, a sodium ion channel implicated in pain syndromes, and to identify molecules that interfere with its function.
Retinal Computations: Recalculating
The presentation from Michal Rivlin, the Life Sciences Laureate of the 2019 Blavatnik Awards in Israel, began with an optical illusion, a dizzying exercise during which a repetitive, unidirectional pattern of motion appeared to rapidly reverse direction. “You probably still perceive motion, but the image is actually stable now,” Rivlin said, completing a powerful demonstration of the action of direction-sensitive retinal ganglion cells (RGCs), whose mechanisms she has studied for more than a decade. The approximately 80 subtypes of RGCs each encode a different aspect, or modality of vision—motion, color, and edges, as well as perception of visual phenomena such as direction. These modalities are hard-wired into the cells and were thought to be immutable—a retinal ganglion cell that perceived left-to-right motion was thought incapable of responding to visual signals that move right-to-left. Rivlin’s research has challenged not only this notion, but also many other beliefs about the function and capabilities of the retina.
Rather than simply capturing discrete aspects of visual information like a camera and relaying that information to the visual thalamus for processing, the cells of the retina actually perform complex processing functions and display a surprising level of plasticity. Rivlin’s lab is probing both the anatomy and functionality of various types of retinal ganglion cells, including those that demonstrate selectivity, such as a preference for movement in one direction or attunement to increases or decreases in illumination. By exposing these cells to various repetitive stimuli, Rivlin has shown that the selectivity of RGCs can be reversed, even in adult retinas.
Direction-selective retinal ganglion cells that prefer left-to-right motion (Before) can change their directional preference (After) following a repetitive visual stimulus.
These dynamic changes in cells whose preferences were believed to be singular and hard-wired have implications not just for understanding retinal function but for understanding the physiological basis of visual perception. Stimulus-dependent changes in the coding of retinal ganglion cells also have downstream impacts on the visual thalamus, where retinal signals are processed. This unexpected plasticity in retinal cells has led Rivlin and her collaborators to investigate the possibility that the visual thalamus and other parts of the visual system might also display greater plasticity than previously believed.
Targeting Sodium Channels for Pain Treatment
Nature’s deadliest predators may seem an unlikely inspiration for developing new analgesic drugs, but as Nieng Yan, 2019 Blavatnik National Awards Finalist, explained, the potent toxins of some snails, spiders, and fish are the basis for research that could lead to safer alternatives to opioid medications.
Voltage-gated ion channels are responsible for electrical signaling in cells of the brain, heart, and skeletal muscles. Sodium channels are one of many ion channel subtypes, and their connection to pain signaling is well documented. Sodium channel blockers have been used as analgesics for a century, but they can be dangerously indiscriminate, inhibiting both the intended channel as well as others in cardiac or muscle tissues. The development of highly selective small molecules capable of blocking only channels tied to pain signaling seemed nearly impossible until two breakthroughs—one genetic, the other technological—brought a potential path for success into focus.
A 2006 study of families with a rare genetic mutation that renders them fully insensitive to pain turned researchers’ focus to the role of the gene SCN9A, which codes for the voltage-gated sodium ion channel Nav 1.7, in pain syndromes. Earlier studies showed that overexpression of SCN9A caused patients to suffer extreme pain sensitivity, and it was now clear that loss of function mutations resulted in the opposite condition.
A powerful natural toxin derived from corn snails blocks the pore of a voltage-gated sodium channel, halting the flow of ions and inhibiting the initiation of an action potential.
As Yan explained, understanding this channel required the ability to resolve its structure, but imaging techniques available at that time were poorly suited to large, membrane-bound proteins. With the advent of cryo-electron microscopy, Yan and other researchers have not only resolved the structure of Nav 1.7, but also characterized small molecules—mostly derived from animal toxins—that precisely and selectively interfere with its function. Developing synthetic drugs based on these molecules is the next phase of discovery, and it’s one that may happen more quickly than expected. “When I started my lab, I thought resolving this protein’s structure would be a lifetime project, but we shortened it to just five years,” said Yan.
A novel approach to developing machine learning algorithms has improved applications for non-linear datasets.
Neural networks can now be used for complex predictive tasks, including forecasting polypharmacy side effects.
5G wireless networks will expand the capabilities of internet-connected devices, providing dramatically faster data transmission and increased reliability.
Tools used to design wireless networks can also be used to understand vulnerabilities in the design of online platforms and social networks, particularly as it pertains to user privacy and data anonymization.
Machine Learning with Networks
“For the first time in history, we are using computers to process data at scale to gain novel insights,” said Jure Leskovec, a Blavatnik National Awards Finalist in 2017, 2018, and 2019, describing one aspect of the digital transformation of science, technology, and society. This shift, from using computers to run calculations or simulations to using them to generate insights, is driven in part by the massive data streams available from the Internet and internet-connected devices. Machine learning has catalyzed this transformation, allowing researchers to not only glean useful information from large datasets, but to make increasingly reliable predictions based on it. Just as new imaging techniques reveal previously unknown structures and phenomena in biology, astronomy, and other fields, so too are big data and machine learning bringing previously unobservable models, signals, and patterns to the surface.
This “new paradigm for discovery” has limitations, as Leskovec explained. Machine learning has advanced most rapidly in areas where data can be represented as simple sequences or grids, such as computer vision, image analysis, and speech processing. Analysis of more complex datasets—represented by networks rather than linear sequences—was beyond the scope of neural networks until recently, when Leskovec and his collaborators approached the challenge from a different angle.
The team considered networks as computation graphs, recognizing that the key to making predictions was understanding how information propagates across the network. By training each node in the network to collect information about neighboring nodes and aggregating the resulting data, they can use node-level information to make predictions within the context of the entire network.
Each node within a network collects information from neighboring nodes. Together, this information can be used to make predictions within the context of the network as a whole.
Leskovec shared two case studies demonstrating the broad applicability of this approach. In healthcare, a neural network designed by Leskovec is identifying previously undocumented side effects from drug-drug interactions. Each network node represents a drug or a protein target of a drug, with links between the nodes emerging based on shared side effects, protein targets, and protein-protein interactions. This type of polydrug side effects analysis is infeasible through clinical trials, and Leskovec is working to optimize it as a point-of-care tool for clinicians.
A similar system has been deployed on the online platform Pinterest, where Leskovec serves as Chief Scientist. It has improved the site’s ability to classify users’ preferences and suggest additional content. “We’re generalizing deep learning methodologies to complex data types, and this is leading to new frontiers,” Leskovec said.
Understanding and Engineering Communications Networks
Elza Erkip has never seen a slide rule. In two decades as a faculty researcher and electrical and computer engineer, Erkip, 2010 Blavatnik Awards Finalist, has corrected her share of misconceptions about her field, and about the role of engineering among the scientific disciplines. She joked about stereotypes portraying engineers—most of them men—wielding slide rules or wearing hard hats, but emphasized the importance of raising awareness about the real-life work of engineers. “Scientists want to understand the universe, but engineers use existing scientific knowledge to design and build things,” she explained. “We contribute to discovery, but mostly we want to solve problems, to find solutions that work in the real world.”
Erkip focuses on one of the most impactful areas of 21st century living—wireless communication—and the ever-evolving suite of technologies that support it. She reviewed the rapid progression of wireless device capabilities, from phones that featured only voice calling and text messaging, through the addition of Wi-Fi capability and web browsing, all the way to the smartphones of today, which boast more computing power than the Apollo 11 spacecraft that landed on the moon. She described the next revolution in wireless—5G networks and devices—which promises higher data rates and significant increases in speed and reliability. Tapping the millimeter-wave bands of the electromagnetic spectrum, 5G will rely on different wireless architectures featuring massive arrays of small antennae, which are better suited to propagating shorter wavelengths. The increased bandwidth will enable many more devices to come online. “It won’t just be humans communicating—we’ll have devices communicating with each other,” Erkip said, describing the future connectivity between robots, autonomous cars, home appliances, and sensors embedded in transportation, manufacturing, and industrial equipment.
Despite efforts to anonymize data, many social media sites and online databases remain vulnerable to efforts to match users’ identities across platforms.
Erkip also discussed the application of tools used to understand and build wireless networks to gain insight into privacy issues within social networks. De-anonymization of user data has long plagued online platforms. Studies have shown that it’s often possible to identify and match users across multiple social platforms or databases using publicly available information—a breach that has greater implications for a database of health or voting records than it does for a consumer-oriented site such as Netflix. Erkip is working to understand the fundamental properties of these networks to elucidate the factors that predispose them to de-anonymization attacks.
IEEE International Symposium on Information Theory. 2018.
Materials Science
Speakers
Chiara Daraio Caltech
Liangbing Hu University of Maryland, College Park
Highlights
Computer-aided manufacturing is enabling researchers to design materials with precisely tuned properties, such as responsiveness to light, temperature, or moisture.
Structured materials can mimic robots or machines, changing shape and form repeatedly in the presence of various stimuli.
Ultra-strong, lightweight wood-based materials made of nanocellulose fibers may one day resolve some of the world’s most pressing challenges in water, energy and sustainability, replacing transparent plastic packaging, window glass, and even steel and other alloys in vehicles and buildings.
Mechanics of Robotic Matter
Chiara Daraio’s work challenges the traditional definition of words like material, structure, and robot. Working at the intersection of physics, materials science, and computer science, she designs materials with novel properties and functionalities, enabled by computer-aided design and 3D fabrication. Rather than considering a material as the foundation for assembling a structure, Daraio, 2019 Blavatnik National Awards Finalist, designs materials with intricate structures in unique and complex geometries.
Daraio demonstrated a series of responsive materials—those that morph in the presence of stimuli such as temperature, light, moisture, or salinity. In their simplest forms, these materials change shape—a piece of heat-responsive material folds and unfolds as air temperature changes, or a leaf-shaped hydro-sensitive material opens and closes as it transitions from wet to dry. In more complex forms, materials can display time-dependent responses, as shown in a video demonstration of a row of polymer strips changing shape at different rates, depending on their thickness. Daraio showed how computer-graphical approaches allow researchers to design a single material with different properties in different regions, allowing complex actuation in a time-dependent manner, such as a polymer “flower” with interconnecting leaves taking shape and a polymer “ribbon” slowly interweaving a knot.
A thin foil elastomer comprised of materials with alternating temperature-sensitivity (heat and cold) folds up and “walks” across a table as the temperature varies.
Conventional ideas dictate that a robot is a programmable machine capable of completing a task. “But what if the material is the machine?” asked Daraio, showing the remarkable capabilities of a thin liquid crystal elastomer foil composed of one heat-sensitive and one cold-sensitive material. At room temperature, the foil is flat. Heat from a warm table causes it to curl upward, turn over, and “walk” forward. “As long as there’s some kind of external environmental stimulus, we can design a material that can repeatedly perform actions in time,” Daraio said. Similar responsive materials have been used in a self-deploying solar panel that [remove folds and] unfolds in response to heat.
Materials have been “the seeds of technological innovation” throughout human history, and Daraio believes that structured materials will enable new functionalities at the macroscale—for use in wearables such as helmets as well as in smart building technologies—and at the microscale, where responsive materials could be used for medical diagnostics or drug delivery.
Sustainable Applications for Wood Nanotechnologies
Wood, glass, plastic, and steel are among the most ubiquitous materials on Earth, and Liangbing Hu, 2019 Blavatnik National Awards Finalist, is rethinking them all. Inspired by the global need to develop sustainable materials, Hu turned to the most plentiful source of biomass on Earth— trees—to create a new generation of wood-based materials with astonishing properties. Hu relies on nanocellulose fibers, which can be engineered to serve as alternatives to commonly used unsustainable or energy-intensive materials.
Hu introduced a transparent film that could pass for plastic and can be used for packaging, yet is ten times stronger and far more versatile. This transparent nanopaper, made of nanocellulose fibers, could also be used as a display material in flexible electronics or as a photonic overlay that boosts the efficiency of solar cells by 30%.
Hu has also tested transparent wood—a heavier-gauge version of nanopaper made by removing lignin from wood and injecting the channels with a clear polymer—as an energy-saving building material. More than half of home energy loss is due to poor wall insulation and leakage through window glass. By Hu’s calculations, replacing glass windows with transparent wood would also provide a six-fold increase in thermal insulation. Pressed, delignified wood has also proven to be a superior material for wall insulation. Used on roofs, it is a highly efficient means of passive cooling—the material absorbs heat and then re-radiates it, cooling the surface below it by about ten degrees.
White delignified wood is pressed to increase its strength. It can be used on roofs to passively cool homes by absorbing and re-radiating light, cooling the area below it by about ten degrees.
Comparisons of mechanical strength between wood and steel are almost laughable, unless the wood is another of Hu’s creations—the aptly named “superwood.” Delignified and compressed to align the nanocellulose fibers, even inexpensive woods become thinner and 10-20 times stronger. Superwood rivals steel in strength and durability, and could become a viable alternative to steel and other alloys in buildings, vehicles, trains, and airplanes. Sustainable sourcing would eliminate pollution and carbon dioxide associated with steel production, and its lightweight profile could drastically improve vehicle fuel efficiency.
Tumor cells are genetically heterogeneous, complicating efforts to sequence DNA from tumor tissue samples.
Techniques for isolating and sequencing single-cell samples have transformed the study of cancer genetics.
Stimulated Ramen scattering, a non-invasive imaging technique, can visualize processes including glucose uptake and fatty acid metabolism within living cells.
Single Cell Genomics: A Revolution in Cancer Biology
Nicholas Navin, 2019 Blavatnik National Awards Finalist, doesn’t use the word “revolution” lightly, but when it comes to the field of single-cell genomics and its impact on cancer research, he stands by the term. Over the past ten years, DNA sequencing of single tumor cells has led to major discoveries about the progression of cancer and the process by which cancer cells resist treatment.
Unlike healthy tissue cells, tumor cells are characterized by genomic heterogeneity. Samples from different areas of the same tumor often contain different mutations or numbers of chromosomes. This diversity has long piqued researchers’ curiosity. “Is it stochastic noise generated as tumor cells acquire different mutations, or could this diversity be important for resistance to therapy, invasion, or metastasis?” Navin asked.
Answering that question required the ability to do comparative studies of single tumor cells, a task that was long out of reach. DNA sequencing technologies historically required a large sample of genetic material—a tricky proposition when sampling a highly diverse population of tumor cells. Some mutations, which could drive invasion or resistance, may be present in just a few cells and thus not be represented in the results. Navin was part of the first team to develop a method for excising a single cancer cell from a tumor, amplifying the DNA, and producing an individualized genetic sequence. As amplification and sequencing methods have improved, so too have the insights gleaned from single-cell genomic studies, which Navin likens to “paleontology in tumors”—the notion that a sample taken at a single point in time can allow researchers to make inferences about tumor evolution.
Single-cell genomic studies reveal that some cancer cells have innate mechanisms of resistance to chemotherapy, and undergo further transcriptional changes that enhance this resistance.
Single-cell studies have contradicted the idea of a stepwise evolution of cancer cells, with one mutation leading to another and ultimately tipping the scales toward malignancy. Instead, Navin’s studies reveal a punctuated evolution, whereby many cells simultaneously become genetically unstable. Longitudinal studies of single-cell samples in patients with triple-negative breast cancer are beginning to answer questions about how cancer cells evade treatment, showing that cells that survive chemotherapy have innate resistance, and then undergo further transcriptional changes during treatment, which increase resistance.
Translating these findings to the clinic is a longer-term process, but Navin envisions single-cell genomics will significantly impact strategies for targeted therapy, non-invasive monitoring, and early cancer detection.
Chemical Imaging in Biomedicine
Wei Min, a Blavatnik Awards Finalist in 2012 and 2019, concluded the session with a visually striking glimpse into the world of stimulated Raman scattering (SRS) microscopy. This noninvasive imaging technique provides both sub-cellular resolution and chemical information about living cells, while transcending some of the limitations of fluorescence-based optical microscopy. The probes used to tag molecules for fluorescent imaging can alter or destroy small molecules of interest, including glucose, lipids, amino acids, or neurotransmitters. Rather than using tags, SRS builds on traditional Raman spectroscopy, which captures and analyzes light scattered by the unique vibrational frequencies between atoms in biomolecules. The original method, first pioneered in the 1930s, is slow and lacks sensitivity, but in 2008, Min and others improved the technique.
SRS has since become a leading method for label-free visualization of living cells, providing an unprecedented window into cellular activities. Using SRS and a variety of custom chemical tags—“vibrational tags,” as Min described them—bound to biomolecules such as DNA or RNA bases, amino acids, or even glucose, researchers can observe the dynamics of biological functions. SRS has visualized glucose uptake in neurons and malignant tumors, and has been used to observe fatty acid metabolism, a critical step in understanding lipid disorders. Imaging small drug molecules is notoriously difficult, but Min reported the results of experiments using SRS to tag therapeutic drug molecules and study their activity within tissues.
Stimulated Raman scattering microscopy uses chemical tags to image small biological molecules in living cells. The technique can visualize cellular processes including glucose uptake in healthy cells and tumor cells.
A recent breakthrough in SRS technology involves pairing it with Raman dyes to break the “color barrier” in optical imaging. Due to the width of the fluorescent spectrum, labels are limited to five or six colors per sample, which prevents researchers from imaging many structures within a tissue sample simultaneously. Min has introduced a hybrid imaging technique that allows for super-multiplexed imaging—up to 10 colors in a single cell image—and utilizes a dramatically expanded palette of Raman frequencies that yield at least 20 distinct colors.
Dr. Kastner brings people together to leverage complementary strengths and achieve a common goal.
Published October 1, 2019
By Marie Samanovic Golden, PhD
Daniel L. Kastner, MD, PhD, Scientific Director for the Intramural Research Program at the National Human Genome Research Institute (NHGRI), received the 2019 Ross Prize in Molecular Medicine — an honor established by The Feinstein Institutes for Medical Research and the Springer Nature journal Molecular Medicine — for his pioneering work on the genomics of auto-inflammatory diseases.
Dr. Daniel Kastner (right) with colleague Dr. David Beck (left)
“The Ross Prize is the most memorable, exciting, rewarding prize that I have ever received,” declared Kastner.
In the 1990s, Dr. Kastner led an international consortium that identified the gene responsible for familial Mediterranean fever (FMF), a rare inherited disorder characterized by recurrent fevers and severe inflammation.
What makes Dr. Kastner unique is that he is a master in bringing people together, helping them to leverage complementary strengths and achieve a common goal. This manifested in the international FMF consortium, comprising six groups with a total of 46 collaborators located in Israel, Australia and four centers around the United States.
“Ideal collaborations are win-win propositions,” said Kastner, and “trust is the currency of the realm.”
Advances in Autoinflammatory Disease Research
The endeavor was a resounding success. It also laid the groundwork for the identification of the tumor necrosis factor receptor-associated periodic syndrome (TRAPS), a second periodic fever syndrome beside FMF, which led to the novel concept of an emerging family of autoinflammatory diseases.
Inflammation is now thought to play an important role in a number of rare monogenic diseases akin to FMF and TRAPS, as well in more common and genetically complex diseases like gout.
Colleagues of Dr. Kastner, like Dr. Luke O’Neil from Trinity College Dublin, take the bold position that addressing inflammation could impact any number of ailments. Certainly it is the case that inflammation plays an important role in several common diseases such as atherosclerosis and cancer. However, “the inflammatory process is a double-edged sword” warned Kastner.
Indeed, dampening patients’ autoinflammatory diseases with anti-inflammatory agents brings them to a normal, base-level of immunity — and may even be protective against other inflammation-mediated disorders. But in most individuals, a blanket prescription of anti-inflammatories could prevent their immune systems from performing its most basic and necessary function: fighting off microbial infections.
Developing the Clinical Infrastructure
Looking ahead, Dr. Kastner developed a clinical infrastructure at the National Institutes of Health (NIH) to examine patients with undiagnosed inflammatory diseases, using genetics to identify the cause of rare diseases and autoinflammatory disorders. As of 2019, the inflammatory diseases section has seen over 2,000 patients, referred from around the world. This prolific program led to the identification of more than 15 new diseases, and over half of them now have effective therapies.
Treatments for these diseases, such as cytokine inhibitors or JAK-kinase inhibitors, target the molecular pathways involved, but are only effective for as long as patients take them. Thus, curative measures such as bone-marrow transplants, or potentially gene therapy, are attractive to patients and their families. But these are not without risk, advised Kastner.
For inflammatory diseases caused by mutations in white blood cells, bone marrow transplants are appealing and logical in lieu of a lifetime of treatment. However, depending on the clinical circumstances, this measure may come with a significant mortality rate, he explained.
Weighing the Risk-Benefits
It is difficult to justify such risk if patients are responding to effective drugs such as colchicine (for the control of FMF), with no reported long-term side effects in the last 50 years. Dr. Kastner is constantly working to weigh these risk-benefits with his patients.
Dr. Kastner shared that he owes a debt of gratitude to Dr. Robert Rich, his first research mentor at Baylor College of Medicine, who not only allowed him, but also expected him to follow his interests independently as a young scientist. Dr. Rich also urged him to go back to medical school after his PhD, to apply his new knowledge to the care of patients.
Kastner continues this tradition, constantly moving between the bench and the bedside in his continued quest to understand inflammatory disease.
Sam Parnia, a leading expert in resuscitation science research, explains how death is not an absolute, but a process, and what happens when patients experience death.
Sam Parnia MD, PhD
Published September 30, 2019
By Robert Birchard
Across time and cultures, people have been conditioned to view death as an endpoint to the experience of life. However, advances in resuscitation science and critical care medicine have challenged assumptions about the finality of death. Sam Parnia, Director of the Critical Care & Resuscitation Research Division of Pulmonary, Critical Care & Sleep Medicine at New York University Langone Medical Center, recently spoke to The New York Academy of Sciences about his resuscitation science research. Dr. Parnia’s work illuminates how death is not an absolute, but a process, and what happens when patients experience death — sharing insights from his research in his own words:
What is death?
Death occurs when the heart stops beating. We call this death by cardiopulmonary criteria and it is how death is defined for more than 95 percent of people. A person stops breathing and their brain shuts down, causing all life processes to cease. More recently with the birth of modern intensive care medicine and the ability to artificially keep people’s hearts beating, doctors like myself can keep a patient’s heart beating longer.
Where people may have suffered irreversible brain damage and brain death, this leads to a situation where the brain has died, but the person’s heart is still beating, so legally, they are declared dead based upon irreversible brain death, or death by brain death criteria. This happens in a small fraction of the cases where people are declared dead.
For millennia death was considered an irreversible event and nothing could restore life. During the last decade, we’ve realized it’s only after a person has died that the cells inside their body, including the brain, begin their own death process. We used to think that you had five or 10 minutes before brain cells died, from a lack of oxygen, but we now know that’s wrong.
You have hours, if not days, before the brain and other organs in the body are irreversibly damaged after death. It’s actually the restoration of oxygen and blood flow back into organs after a person’s heart stops, but is then resuscitated that paradoxically leads to accelerated cell death. So, this accelerated secondary injury process is what we need to combat in medicine now.
Why is the term “near-death” experience inaccurate?
The problem with this term is that it is inconsistent with what people actually experience. It is undefined and imprecise. If I said ‘an airplane was involved in a near-miss incident,’ what does that mean? Did you have another plane come in within an inch of another plane, or were they a mile away? The term is ill-defined, and, it doesn’t take into consideration the fact that a lot of people have biologically died and returned.
What is a death experience?
I call it an “experience of death” because that’s what it is. People report a unique cognitive experience in relation to death. They may have a perception of seeing their body and the doctors and nurses trying to revive them, yet feel very peaceful while observing. Some report a realization that they may have actually died.
Later they develop a perception or a sensation of being pulled towards a type of destination. During the experience, they review their life from birth, until death, and interestingly this review is based upon their humanity.
They don’t review their lives based on what people strive for, like a career, promotions, or an amazing vacation. Their perspective is focused on their humanity. They notice incidents where they lacked dignity, acted inappropriately towards others, or conversely, acted with humanity and kindness.
They re-experience and relive these moments, but also, what’s fascinating, which sort of blows me away because I can’t really explain it, is they also describe these experiences from the other person’s perspective.
If they caused pain, they experience the same pain that other person felt, even if they didn’t realize it at the time. They actually judge themselves. They suddenly realize why their actions were good or bad, and many claim to see the downstream consequences of their actions.
How do studies of cardiac arrest inform the debate on the nature of consciousness?
Traditionally, researchers had proposed that mind or consciousness – our self – is produced from organized brain activity. However, nobody has ever been able to show how brain cells, which produce proteins, can generate something so different i.e. thoughts or consciousness. Interestingly, there has never been a plausible biological mechanism proposed to account for this.
Recently some researchers have started to raise the question that maybe your mind, your consciousness, your psyche, the thing that makes you, may not be produced by the brain. The brain might be acting more like an intermediary. It’s not a brand new idea. They have argued that we have no evidence to show how brain cells or connections of brain cells could produce your thoughts, mind or consciousness.
The fact that people seem to have full consciousness, with lucid well-structured thought processes and memory formation from a time when their brains are highly dysfunctional or even nonfunctional is perplexing and paradoxical.
I do agree that this raises the possibility that the entity we call the mind or consciousness may not be produced by the brain. It’s certainly possible that maybe there’s another layer of reality that we haven’t yet discovered that’s essentially beyond what we know of the brain, and which determines our reality.
So, I believe it is possible for consciousness to be an as of yet undiscovered scientific entity that may not necessarily be produced by synaptic activity in the brain.
The human body regenerates itself constantly, replacing old, worn-out cells with a continuous supply of new ones in almost all tissues. The secret to this perpetual renewal is a small but persistent supply of stem cells, which multiply to replace themselves and also generate progeny that can differentiate into more specialized cell types. For decades, scientists have tried to isolate and modify stem cells to treat disease, but in recent years the field has accelerated dramatically.
A major breakthrough came in the early 21st century, when researchers in Japan figured out how to reverse the differentiation process, allowing them to derive induced pluripotent stem (iPS) cells from fully differentiated cells. Since then, iPS cells have become a cornerstone of regenerative medicine. Researchers can isolate cells from a patient, produce iPS cells, genetically modify them to repair any defects, then induce the cells to form the tissue the patient needs regenerated.
On April 26, 2019, the New York Academy of Sciences and Takeda Pharmaceuticals hosted the Frontiers in Regenerative Medicine Symposium to celebrate 2019 Innovators in Science Award winners and highlight the work of researchers pioneering techniques in regenerative medicine. Presentations and an interactive panel session covered exciting basic research findings and impressive clinical successes, revealing the immense potential of this rapidly developing field.
Symposium Highlights
New cell lines should reduce the time and cost of developing stem cell-derived therapies.
The body’s microbiome primes stem cells to respond to infections.
iPS cell-derived therapies have already treated a deadly genetic skin disease and age-related macular degeneration.
Polyvinyl alcohol is a superior substitute for albumin in stem cell culture media.
A newly isolated type of stem cell reveals the stepwise process driving early embryo organization.
Speakers
Shinya Yamanaka Kyoto University
Shruti Naik New York University
Michele De Luca University of Modena and Reggio Emilia
Masayo Takahashi RIKEN Center for Biosystems Dynamics Research
Hiromitsu Nakauchi Stanford University and University of Tokyo
Brigid L.M. Hogan Duke University School of Medicine
Emmanuelle Passegué Columbia University Irving Medical Center
Hans Schöler Max Planck Institute for Molecular Biomedicine
Austin Smith University of Cambridge
Moderator: Azim Surani University of Cambridge
Sponsors
Recent Progress in iPS Cell Research Application
Speakers
Shinya Yamanaka Kyoto University
Highlights
Current protocols for using induced pluripotent stem (iPS) cells clinically are slow and expensive.
HLA “superdonor” iPS cell lines can be used to treat multiple patients, reducing costs.
A unique academic-industry partnership is helping iPS cell therapies reach the clinic.
Faster, Cheaper, Better
Shinya Yamanaka of Kyoto University, gave the meeting’s keynote presentation, summarizing his laboratory’s recent work using induced pluripotent stem (iPS) cells for regenerative medicine. The first clinical trial using iPS cells to treat age-related macular degeneration started five years ago. In his clinical trial, physicians isolated somatic cells from a patient, then used developed culture techniques to derive iPS cells from them. iPS cells can proliferate and differentiate into any type of cell in the body, which can then be transplanted back into the patient. Experiments over the past five years have shown that this approach has the potential to treat diseases ranging from age-related macular degeneration to Parkinson’s disease.
However, this autologous transplantation strategy is slow and expensive. “It takes up to a year just evaluating one patient, [and] it costs us almost one million US dollars,” said Yamanaka. Before transplanting the differentiated cells, the researchers evaluated the entire iPS cell derivation and iPS cell differentiation processes, adding to time and cost. As another strategy, Yamanaka’s team is working on the iPS Cell Stock for Regenerative Medicine. Here, iPS cells are derived from blood cells of healthy donors, not the patients, and are stocked. The primary problem with this approach is the human leukocyte antigen (HLA) system, which encodes multiple cell surface proteins. Each person has a specific combination of HLA genes, or haplotype, defining the HLA proteins expressed on their own cells. The immune system recognizes and eliminates any cell expressing non-self HLA proteins. Because there are millions of potential HLA haplotypes, cells derived from one person will likely be rejected by another.
The homozygous “superdonor” cell line has limited immunological diversity, allowing it to match multiple patients.
The homozygous “superdonor” cell line has limited immunological diversity, allowing it to match multiple patients.
To address that, Yamanaka and his colleagues are collaborating with the Japanese Red Cross to develop “superdonor” iPS cells. These cells carry homozygous alleles for different human lymphocyte antigen (HLA) genes, limiting their immunological diversity and making them match multiple patients. So far, the team has created four “superdonor” cell lines, allowing them to generate cells compatible with 40% of the Japanese population. Those cells are now being used in clinical trials treating macular degeneration and Parkinson’s disease, with more indications planned.
“So far so good,” said Yamanaka, but he added that “in order to cover 90% of the Japanese population we would need 150 iPS cell lines, and in order to cover the entire world we would need over 1,000 lines.” It took the group about five years to generate the first four lines, so simply repeating the process that many more times isn’t practical.
Instead, Yamanaka hopes to take the HLA reduction a step further, knocking out most of the major HLA genes to generate cells that will survive in large swaths of the population. However, simply knocking out entire families of genes isn’t enough. Natural killer cells attack cells that are missing particular cell surface antigens, so the researchers had to leave specific markers in the cells, or reintroduce them transgenically. Natural killer and T cells from various donors ignore leukocytes derived from these highly engineered iPS cells, proving that the concept works. With this approach, just ten lines of iPS cells should yield a range of donor cells suitable for any human HLA combination. Yamanaka expects these gene-edited iPS cells to be available in 2020.
By 2025, Yamanaka hopes to announce “my iPS cell” technology. This technology will reduce the cost and time for autologous transplantation to about $10,000 and one month per patient.
While preclinical and early clinical trials on iPS cells have yielded promising results, the new therapies must still cross the “valley of death,” the pharmaceutical industry’s term for the unsuccessful transition and industrialization of innovative ideas identified in academia to routine clinical use. In an effort to make that process more reliable, Yamanaka and his colleagues have begun a unique collaboration with Takeda Pharmaceutical Company Limited, Japan’s largest drug maker. The effort involves 100 scientists, 50 each from the company and academic laboratories. The corporate researchers gain access to the latest basic science developments on iPS cell technology, while the academics can use the company’s cutting-edge R&D know-how equipment and vast chemical libraries.
In one project, the collaborators used iPS cells to derive pancreatic islet cells, and then encapsulated the cells in an implantable device to treat type 1 diabetes. The system successfully decreased blood glucose in a mouse model, and the team is now scaling up cell production to test it in humans in the future. Another effort identified chemicals in Takeda’s compound library that speed cardiomyocyte maturation, which the researchers are now using to improve iPS cell-derived treatments for heart failure. In a third project, the team has modified iPS cell-derived T cells to identify and attack tumors, again showing promising results in a mouse model.
Inflammation causes persistent changes in epithelial stem cells, priming them for subsequent immune responses.
Modified iPS cells can be used to cure a patient with a deadly genetic skin defect.
A small population of self-renewing stem cells maintains human skin cells.
Sparring Partners
Shruti Naik, Early-Career Scientist winner of the 2019 Innovators in Science Award, discussed her work on epithelial barriers. These barriers, which include skin and the linings of the gut, lungs, and urogenital tract, exhibit nuanced responses to the many microbes they encounter. Injuries and pathogenic infections trigger prompt inflammatory responses, but the millions of harmless commensal bacteria that live on these surfaces don’t. How does the epithelium know the difference?
To ask that question, Naik first studied germ-free mice, which lack all types of bacteria. These animals have defective immune responses against pathogens that affect epithelia, so commensal bacteria are clearly required for developing normal epithelial immunity. Naik inoculated the germ-free mice with bacterial strains found either on the skin or in the guts of normal mice, then assessed their immune responses in those two compartments.
“When you gave gut-tropic bacteria, you were essentially able to rescue immunity in the gut but not the skin, and conversely when you gave skin-tropic bacteria, you were able to rescue immunity in the skin and not the gut,” said Naik. Even though the commensal bacteria caused no inflammation, they did activate certain T cells in the epithelia they colonized, apparently preparing those tissues for subsequent attacks by pathogens.
Next, Naik took germ-free mice inoculated with Staphylococcus epidermidis, a normal skin commensal bacterium, and challenged them with an infection by Candida albicans, a pathogenic yeast. The bacterially primed mice produced a much more robust immune response against the yeast infection than control animals that hadn’t gotten S. epidermidis. Naik confirmed that this immune training effect operates through the T cell response she’d seen before. “You essentially develop an immune arsenal to your commensals that helps protect against pathogens,” Naik explained, adding that each epithelial barrier requires its own commensal bacteria to trigger this response.
Augmented wound repair in post-inflammation skin reveals that naive and inflammation-educated skin stem cells respond differently to subsequent stresses.
Augmented wound repair in post-inflammation skin reveals that naive and inflammation-educated skin stem cells respond differently to subsequent stresses.
The response to epithelial commensals is remarkably durable; Naik found that the skin T cells in the inoculated mice remained on alert a year after their initial activation. That led her to wonder whether non-hematopoietic cells, especially epithelial stem cells, contribute to immunological memory in the skin.
To probe that, Naik and a colleague used a mouse model in which the topical drug imiquimod induces a temporary psoriasis-like skin inflammation. By tracing the lineages of cells in the animals’ skin, the researchers found that epithelial stem cells expand during this inflammation, and then persist. Challenging the mice with a wound one month after the inflammation resolves leads to faster healing than if the mice hadn’t had the inflammation. Several other models of wound healing yielded the same result. The investigators concluded that naive and inflammation-educated skin stem cells respond differently to subsequent stresses.
Naik’s team found that inflammation causes persistent changes in skin stem cells’ chromatin organization. Using a clever reporter gene assay, they demonstrated that the initial inflammation leaves inflammatory gene loci more open in the chromatin, making them easier to activate after subsequent insults. “What was really surprising to us was that this change never fully resolved,” said Naik. Even six months after the acute inflammation, skin stem cells retained the distinct post-inflammatory chromatin structure and the ability to heal wounds quickly. This chronic ready-for-action state isn’t always beneficial, though. Naik noticed that the mice that had had the inflammatory treatment were more prone to developing tumors, for example.
In establishing her new laboratory, Naik has now turned her focus to another aspect of epithelial immunity: the link between immune responses and tissue regeneration. She looked first at a type of T cells found in abundance around hair follicles on skin. Mice lacking these cells exhibit severe delays in wound healing, apparently as a result of failing to vascularize the wound area. That implies a previously unknown role for inflammatory T cells in vascularization, which Naik and her lab are now probing.
Skin Deep
Michele De Luca, Senior Scientist winner of the 2019 Innovators in Science Award, has developed techniques for regenerating human skin from transgenic epidermal stem cells. Researchers first isolated holoclones, or cells derived from a single epidermal stem cell, over 30 years ago. These cells can be used to grow sheets of skin in culture for both research and clinical use, but scientists have only recently begun to elucidate how the process works.
The first stem cell-derived therapies tested in humans were for skin and eye burns, allowing doctors to regenerate and replace burned epidermal tissue from a patient’s own stem cells. That’s the basis of Holoclar, a stem cell-based treatment for severe eye burns approved in Europe in 2015.
Holoclar and similar procedures work well for injured patients with normal epithelia. “We wanted to genetically modify those cells in order to address one of the most important genetic diseases in the dermatology field, which is epidermolysis bullosa (EB), a devastating skin disease,” said De Luca. In EB, patients carry a genetic defect in cell adhesion that causes severe blisters all over their skin and prevents normal healing. A large number of EB patients die as children from the resulting infections, and those who survive seldom get beyond young adulthood before succumbing to squamous cell carcinomas.
De Luca developed a strategy to isolate stem cells from a skin biopsy, repair the genetic defect in these cells with a retroviral vector, and then grow new skin in culture that can be transplanted back to the patient, replacing their original skin with genetically repaired skin. In 2015, the researchers carried out the procedure on a young boy named Hassan, who had arrived in the burn unit of a German hospital with EB after fleeing Syria. The burn unit was only able to offer palliative care, and his prognosis was poor because of his constant blistering and infections. De Luca’s team received approval to perform their gene therapy on him.
The new strategy, which combines cell and gene therapy, resulted in the restoration of normal skin adhesion in Hassan.
After isolating and modifying epidermal stem cells from Hassan and growing new sheets of skin in culture, De Luca’s team re-skinned the patient’s arms and legs, then his abdomen and back. The complete procedure took about three months. The new skin resists blister formation even when rubbed and heals normally from minor wounds. In the ensuing three and a half years, Hassan has begun growing normally and living an ordinary, healthy life.
Detailed analysis of skin biopsies showed that Hassan’s epidermis has normal cellular adhesion machinery and revealed that his skin is now derived from a population of proliferating transgenic stem cells, with no single clone dominating. By tracing the lineages of cells carrying the introduced transgene, De Luca was able to identify self-renewing transgenic stem cells, intermediate progenitor cells, and fully differentiated stem cells, indicating normal skin growth and replacement.
Besides being good news for the patient, the results confirmed a longstanding theory of skin regeneration. “These data formally prove that the human epidermis is sustained only by a small population of long-lived stem cells that generates [short-lived epithelial] progenitors,” said De Luca, adding that “with this in mind, we’ve started doing other clinical trials.”
The researchers plan to continue targeting junctional as well as dystrophic forms of EB, both of which are genetically distinct from EB simplex. Initial experiments revealed that in these conditions, transplant recipients developed mosaic skin, where some areas continued to be produced from cells lacking the introduced genetic repair. The non-transgenic cells appeared to be out-competing the transgenic cells and supplanting them, undermining the treatment. De Luca and his colleagues developed a modified strategy that gave the transgenic cells a competitive advantage. This approach and additional advances should allow them to achieve complete transgenic skin coverage.
The Journal of Investigative Dermatology. 2017;137(4):836-44.
.
Good for What Ails Us
Speakers
Masayo Takahashi RIKEN Center for Biosystems Dynamics Research
Hiromitsu Nakauchi Stanford University and University of Tokyo
Highlights
The first clinical use of iPS cells in humans replaced retinal cells in a patient with age-related macular degeneration.
“Superdonor” stem cells can evade immune rejection in multiple patients.
Culturing hematopoietic stem cells has been an ongoing challenge for immunologists.
Polyvinyl alcohol, used in making school glue, is a superior substitute for bovine serum albumin in stem cell culture media.
Large doses of hematopoietic stem cells may obviate the need for immunosuppression in stem cell therapy.
An iPS Cell for an Eye
Masayo Takahashi, of RIKEN Center for Biosystems Dynamics Research, began her talk with a brief description of the new Kobe Eye Center, a purpose-built facility designed to house a complete clinical development pipeline dedicated to curing eye diseases. “Not only cells, not only treatments, but a whole care system is needed to cure the patients,” said Takahashi. In keeping with that philosophy, the Center includes everything from research laboratories to a working eye hospital and a patient welfare facility.
Takahashi’s recent work has focused on treating age-related macular degeneration (AMD). In AMD, the retinal pigment epithelium that nourishes other retinal cells accumulates damage, leading to progressive vision loss. AMD is the most common cause of serious visual impairment in the elderly in the US and EU, and there is no definitive treatment. Fifteen years ago, Takahashi and her colleagues derived retinal pigment epithelial cells from monkey embryonic stem cells and successfully transplanted them into a rat model of AMD, treating the condition in the rodents. They were hesitant to extend the technique to humans, though, because it required suppressing the recipient’s immune response to prevent them from rejecting the monkey cells.
The advent of induced pluripotent stem (iPS) cell technology pointed Takahashi toward a new strategy, in which she took cells from a patient, derived iPS cells from them, and then prompted those cells to differentiate into retinal pigment epithelial cells that were perfectly compatible with the patient’s immune system. Her team then transplanted a sheet of these cells into the patient. That experiment, in 2014, was the first clinical use of iPS cells in humans. “The grafted cells were very stable,” said Takahashi, who has checked the graft in multiple ways in the ensuing years.
Having proven that iPS cell-derived retinal grafts can work, Takahashi and her colleagues sought to make the procedure cheaper and faster. Creating customized iPS cells from each patient is a huge undertaking, so instead the team investigated superdonor iPS cells that can be used for multiple patients. These cells, described by Shinya Yamanaka in his keynote address, express fewer types of human leukocyte antigens than most patients, making them immunologically compatible with large swaths of the population. Just four lines of superdonor iPS cells can be used to derive grafts for 40% of all Japanese people.
Transplantation of an iPS cell-derived sheet into the retina ultimately proved successful.
Transplantation of an iPS cell-derived sheet into the retina ultimately proved successful.
In the next clinical trial, Takahashi’s lab performed several tests to confirm that the patients’ immune cells would not react with the superdonor cells, before proceeding with the first retinal pigment epithelial graft. Nonetheless, after the graft the researchers saw a minuscule fluid pocket in the patient’s retina, apparently due to an immune reaction. Clinicians immediately gave the patient topical steroids in the eye to suppress the reaction. “Then after three weeks or so, the reaction ceased and the fluid was gone, so we could control the immune reaction to the HLA-matched cells,” said Takahashi. Four subsequent patients showed no reaction whatsoever to the iPS superdonor-derived grafts.
While the retinal grafts were successful, none of the patients have shown much improvement in visual acuity so far. Takahashi explained that subjects in the clinical trial all had very severe AMD and extensive loss of their eyes’ photoreceptors. “I think if we select the right patients, we could get good visual acuity if their photoreceptors still remain,” said Takahashi.
Takahashi finished with a brief overview of her other projects, including using aggregates of iPS cells and embryonic stem cells to form organoids, which can self-organize into a retina. She hopes to use this system to develop new therapies for retinitis pigmentosa, another major cause of vision loss. Finally, Takahashi described a project aimed at reducing the cost and increasing the efficacy of stem cell therapies even further by employing a sophisticated laboratory robot. The system, called Mahoro, is capable of learning techniques from the best laboratory technicians, then replicating them perfectly. That should make stem cell culturing procedures much more reproducible and significantly reduce the cost of deploying new therapies.
A Sticky Problem
Hiromitsu Nakauchi, of Stanford University and the University of Tokyo, described his group’s efforts to overcome a decades-old challenge in stem cell research. Scientists have known for over 25 years that all of the blood cells in a human are renewed from a tiny population of multipotent, self-renewing hematopoietic stem cells. In an animal that’s had all of its hematopoietic lineages eliminated by ionizing radiation, a single such cell can reconstitute the entire blood cell population. This protocol is the basis for several experimental models.
In theory, then, a single hematopoietic stem cell should also be able to multiply indefinitely in pure culture, allowing researchers to produce all types of blood cells on demand. In practice, cultured stem cells inevitably differentiate and die off after just a few generations in culture. Nakauchi and his colleagues have been trying to fix that problem. “After years of hard work, we decided to take the reductionist approach and try to define the components that we use to culture [hematopoietic stem cells],” said Nakauchi.
The team focused on the most undefined component of their culture media: bovine serum albumin (BSA). This substance, a crude extract from cow blood, has been considered an essential component of growth media since researchers first managed to culture mammalian cells. However, Nakauchi’s lab found tremendous variation between different lots of BSA, both in the types and quantities of various impurities in them and in their efficacy in keeping stem cells alive. Worse, factors that appeared to be helpful to the cells in some BSA lots were harmful when present in other lots. “So this is not science; depending on the BSA lot you use, you get totally different results,” said Nakauchi.
Next, the researchers switched to a recombinant serum albumin product made in genetically engineered yeast. That exhibited less variation between lots, and after optimizing their culture conditions they were able to grow and expand hematopoietic stem cells for nearly a month. Part of the protocol they developed was to change the medium every other day, which they found was required to remove inflammatory cytokines and chemokines being produced by the stem cells. That suggested the cells were still under stress, perhaps in response to some of the components of the recombinant serum albumin.
Polyvinyl alcohol can replace BSA in culture medium.
Polyvinyl alcohol can replace BSA in culture medium.
The ongoing problems with serum albumin products led Nakauchi to ask why albumin is even necessary in tissue culture. Scientists have known for decades that cells don’t grow well without it, but why not? While trying to figure out what the albumin was doing for the cells, Nakauchi’s lab tested it against the most inert polymer they could find: polyvinyl alcohol (PVA). Best known as the primary ingredient for making school glue, PVA is also used extensively in the food and pharmaceutical industries. To their surprise, hematopoietic stem cells grew better in PVA-spiked medium than in medium with BSA. The PVA-grown cells showed decreased senescence, lower levels of inflammatory cytokines, and better growth rates.
In long-term culture, Nakauchi and his colleagues were able to achieve more than 900-fold expansion of functional mouse hematopoietic stem cells. Transplanting these cells into irradiated mice confirmed that the cells were still fully capable of reconstituting all of the hematopoietic lineages. Further experiments determined that PVA-containing medium also works well for human hematopoietic stem cells.
Besides having immediate uses for basic research, the ability to grow such large numbers of hematopoietic stem cells could overcome a fundamental barrier to using these cells in the clinic. Current hematopoietic stem cell therapies require suppressing or destroying a patient’s existing immune system to allow the transplanted cells to become established, but this immunosuppression can lead to deadly infections. Transplanting a much larger population of stem cells can overcome the need for immunosuppression, but growing enough cells for this approach has been impractical. Using their new culture techniques, Nakauchi’s team can now produce enough hematopoietic stem cells to carry out successful transplants without immunosuppression in mice. They hope to take this approach into the clinic soon.
Brigid L.M. Hogan Duke University School of Medicine
Emmanuelle Passegué Columbia University Irving Medical Center
Hans Schöler Max Planck Institute for Molecular Biomedicine
Austin Smith University of Cambridge
Moderator: Azim Surani University of Cambridge
Highlights
A dramatic transition separates early embryonic stem cells from their descendants.
Newly isolated formative stem cells represent an intermediate step in development.
Organoids derived from iPS cells provide excellent models for studying human physiology and disease.
In the Beginning
Austin Smith, from the University of Cambridge, gave the final presentation, in which he discussed his studies on the progression of embryonic stem cells through development. In mammals, embryonic development begins with the formation of the blastocyst. In 1981, researchers isolated cells from murine blastocysts and demonstrated that each of them can grow into a complete embryo. Stem cells isolated after the embryo has implanted itself into the uterus, called epiblast stem cells, have lost that ability but gained the potential to differentiate into multiple cell lineages in culture. “So we have two different types of pluripotent stem cells in the mouse, and they’re different in just about every way you could imagine,” said Smith.
Work on other species, including human cells, suggests that this transition between two different types of stem cells is a common feature of mammalian development. The transition from the earlier to the later type of stem cell is called capacitation. To find the factors driving capacitation, Smith and his colleagues looked for differences in gene transcription patterns and chromatin organization during the process, in both human and murine cells. What they found was a global re-wiring of nearly every aspect of the cell’s physiology. “Together these things lead to the acquisition of both germline and somatic lineage competence, and at the same time decommission that extra-embryonic lineage potential,” Smith explained.
Having characterized the cells before and after capacitation, the researchers wanted to isolate cells from intermediate stages of the process to understand how it unfolds. To do that, they extracted cells from mouse embryos right after implantation, then grew them in culture conditions that minimized their exposure to signals that would direct them toward specific lineages. Detailed analyses of these cells, which Smith calls formative stem cells, shows that they have characteristics of both the naive embryonic stem cells and the later epiblast stem cells. Injecting these cells into mouse blastocysts yields chimeric mice carrying descendants of the injected cells in all their tissues. The formative stem cells can therefore function like true embryonic stem cells, albeit less efficiently.
The developmental sequence of pluripotent cells.
The developmental sequence of pluripotent cells.
Post-implantation human embryos aren’t available for research, but Smith’s team was able to culture naive stem cells and prompt them to develop into formative stem cells. These cells exhibit transcriptional profiles and other characteristics homologous to those seen in the murine formative stem cells.
Having found the intermediate cell type, Smith was now able to assemble a more detailed view of the steps in development. Returning to the mouse model, he compared the chromatin organization of naive embryonic, formative, and epiblast stem cells. The difference between the naive and formative cells’ chromatin was much more dramatic than between the formative and epiblast cells.
Based on the results, Smith proposes that naive embryonic stem cells begin as a “blank slate,” which then undergoes capacitation to become primed to respond to later differentiation signals. The capacitation process entails a dramatic change in the cell’s transcriptional and chromatin organization and occurs around the time of implantation. “We think we now have in culture … a cell that represents this intermediate stage and that has distinctive functional properties and distinctive molecular properties,” said Smith. After capacitation, the formative stem cells undergo a more gradual shift to become primed stem cells, which are the epiblast stem cells in mice.
Smith concedes that the human data are less detailed, but all of the experiments his team was able to do produced results consistent with the mouse model. Other work has also found corroborating results in non-human primate embryos, implying that the same developmental mechanisms are conserved across mammals.
Organoid Recitals
After the presentations, a panel consisting of members of the Innovators in Science Award’s Scientific Advisory Council and Jury took the stage to address a series of questions from the audience.
The panel first took up the question of how researchers can better study human stem cells, given the ethical challenges of working with embryos. Brigid Hogan described organoid cultures, in which researchers stimulate human iPS cells to grow into minuscule organ-like structures. “This is a way of looking at human development at a stage when it’s [otherwise] completely inaccessible,” said Hogan. Other speakers concurred, adding that implanting human organoids into mice provides an especially useful model.
Another audience member asked about the potential for human stem cell therapy in the brain. Hogan pointed to the use of fetal cells for treating Parkinson’s disease as an example, but panelist Hans Schöler suggested that that could be a unique case. Patients with Parkinson’s disease suffer from deficiency in dopamine-secreting neurons, so implanting cells that secrete dopamine in the correct brain region may provide some relief.
Panelists also addressed the use of stem cells in regenerative medicine, where researchers are targeting the nexus of aging, nutrition, and brain health. Emmanuelle Passegué explained that the body’s progressive failure to regenerate itself from its own stem cells is a hallmark of aging. “I think we are getting to an era where transplantation or engraftment [of cells] will not be the answer, it will really be trying to reawaken the normal properties of the [patient’s own] stem cells,” said Passegué.
As the meeting concluded, speakers and attendees seemed to agree that the field of stem cell research, like the cells themselves, is now poised to develop in a wide range of promising directions.








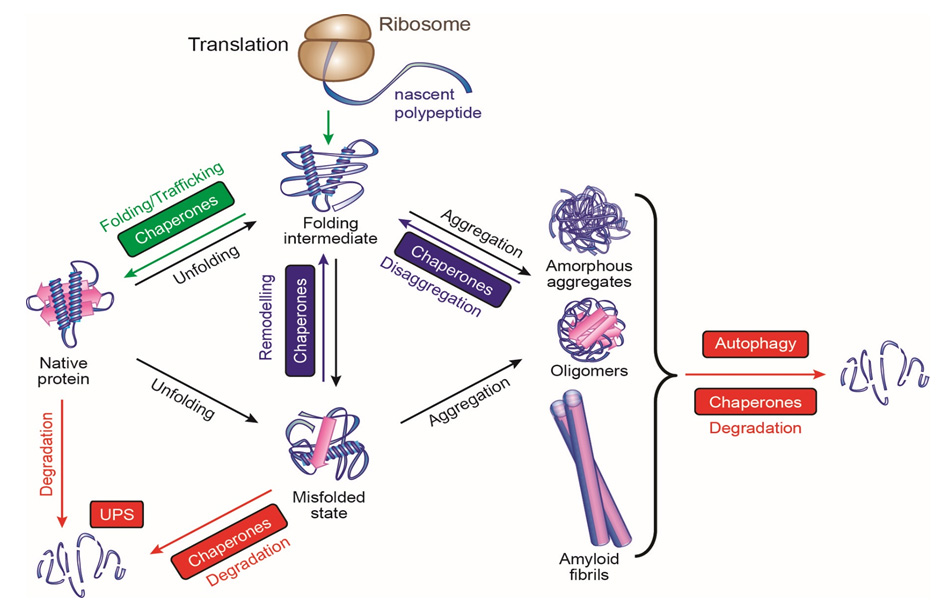
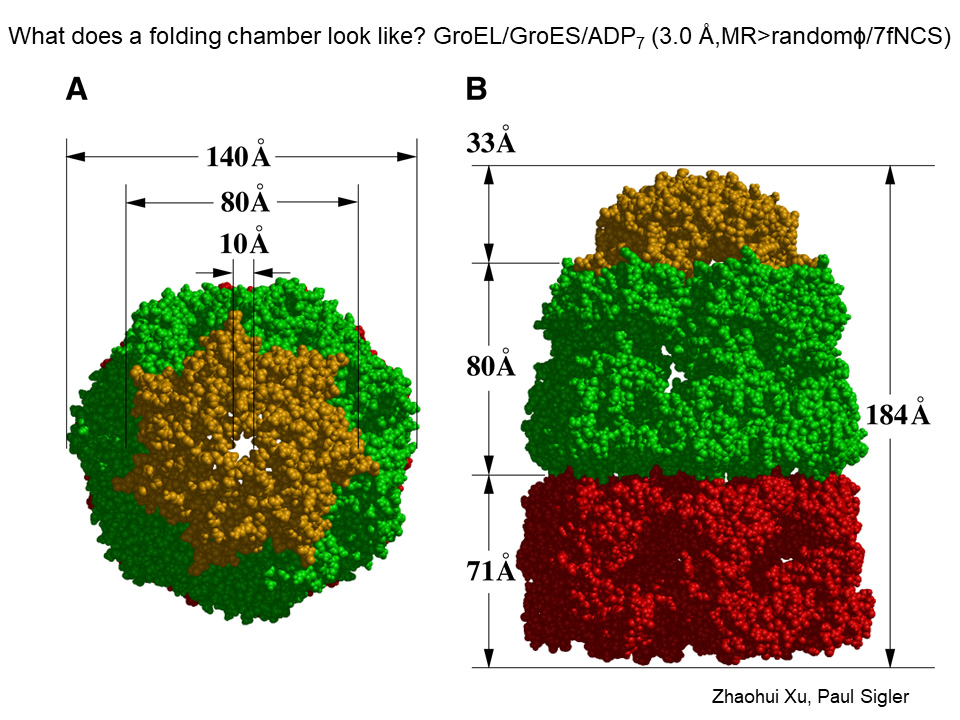
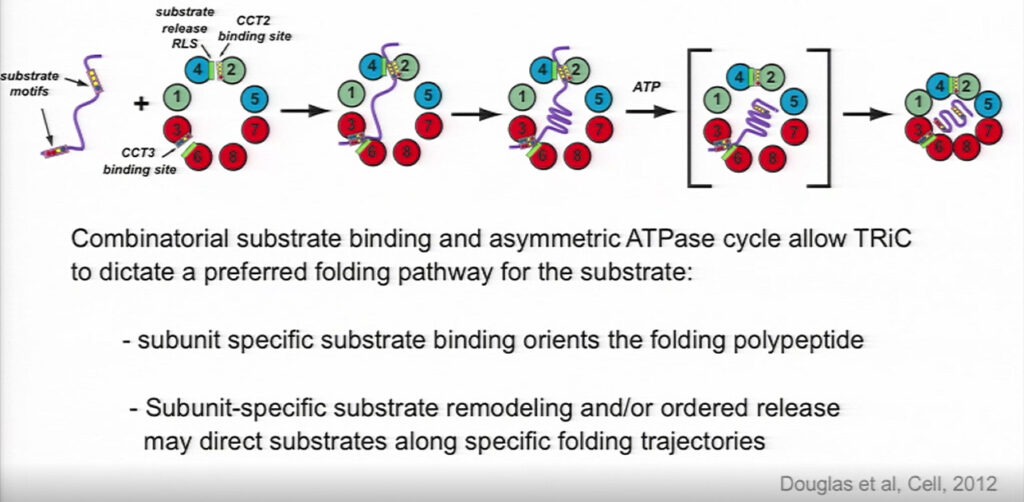
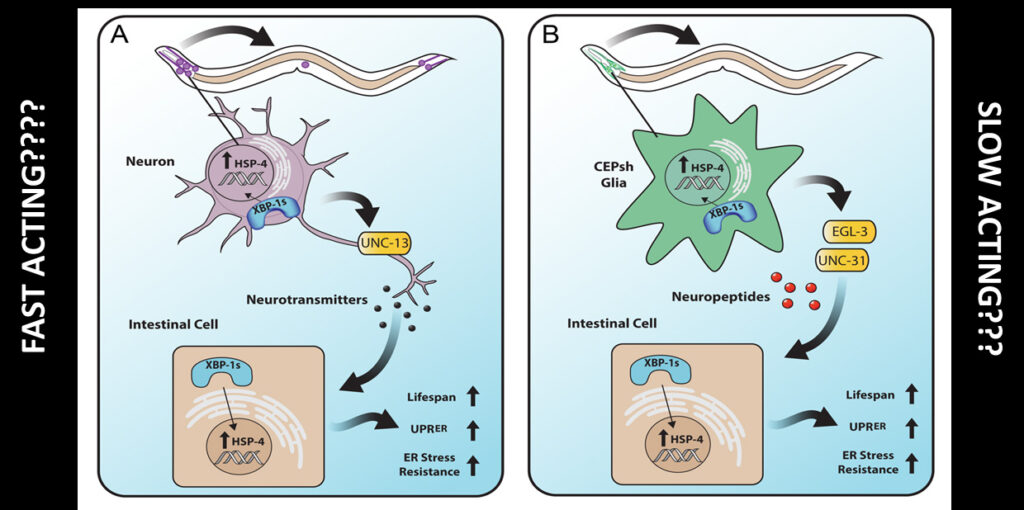
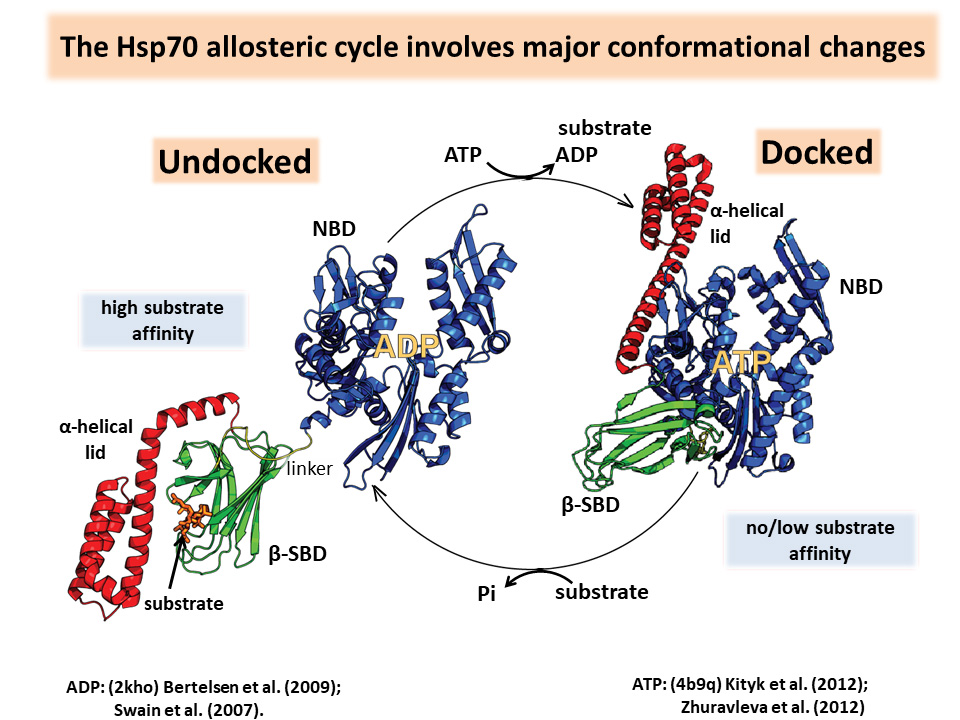





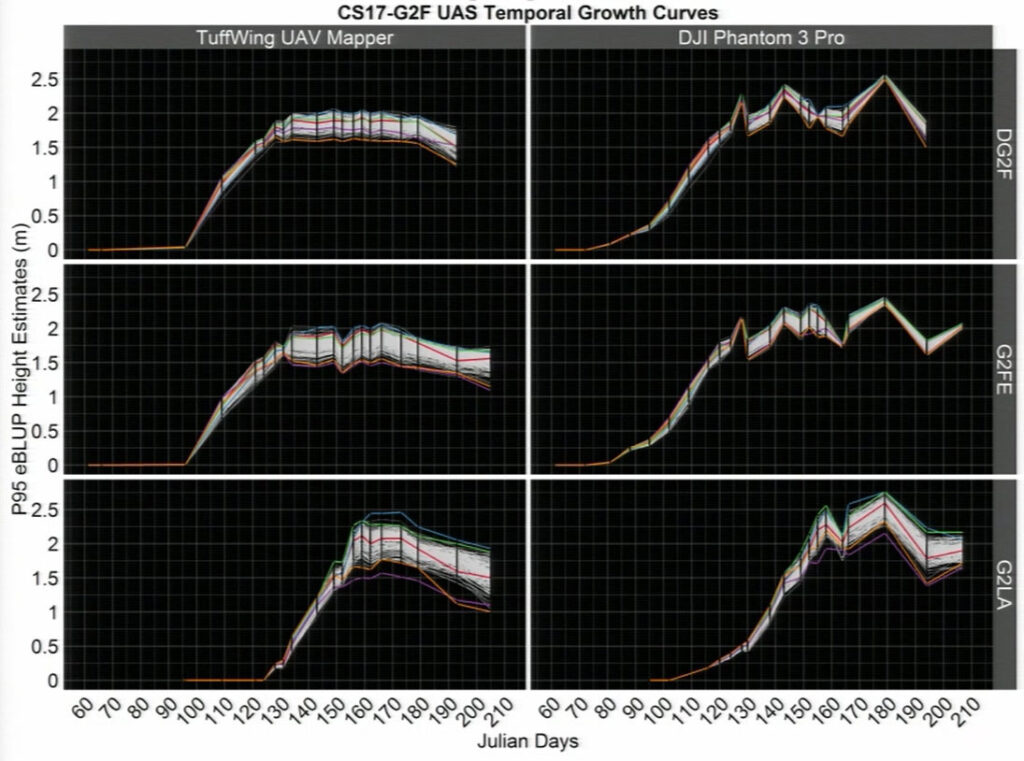
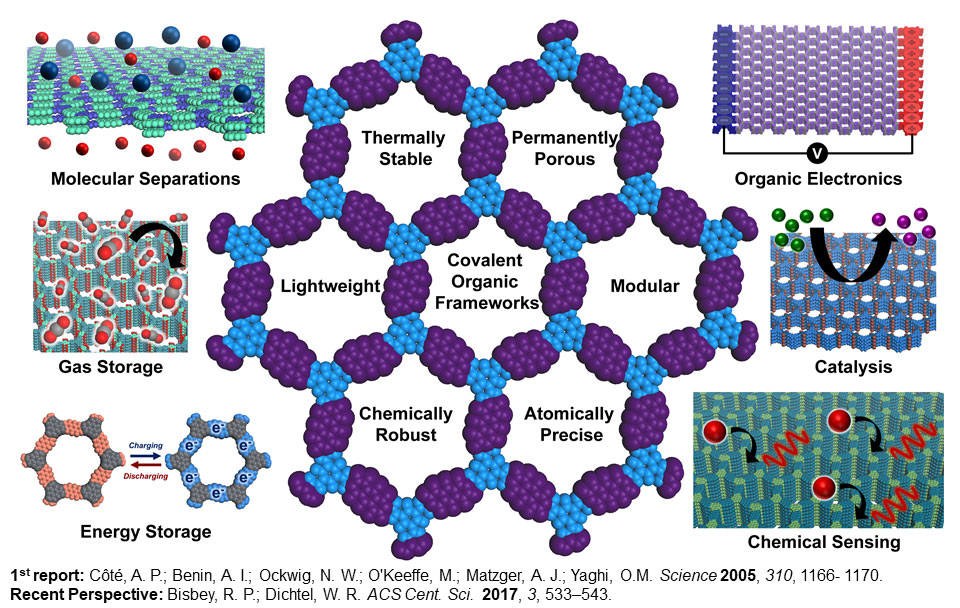
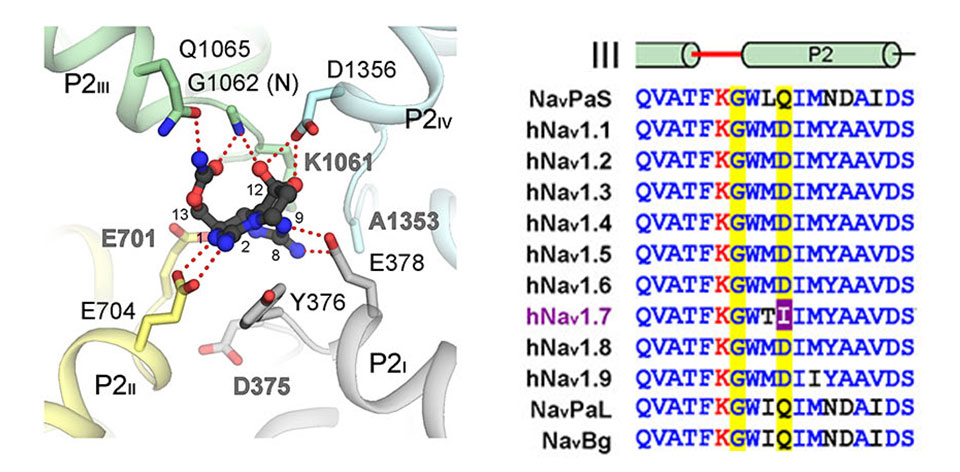
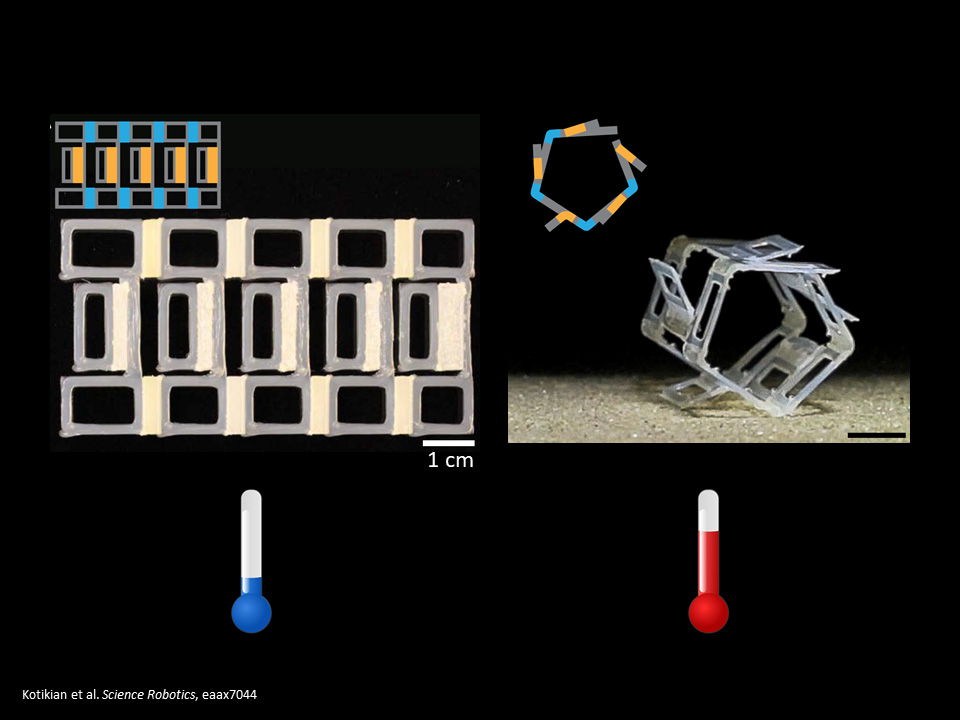
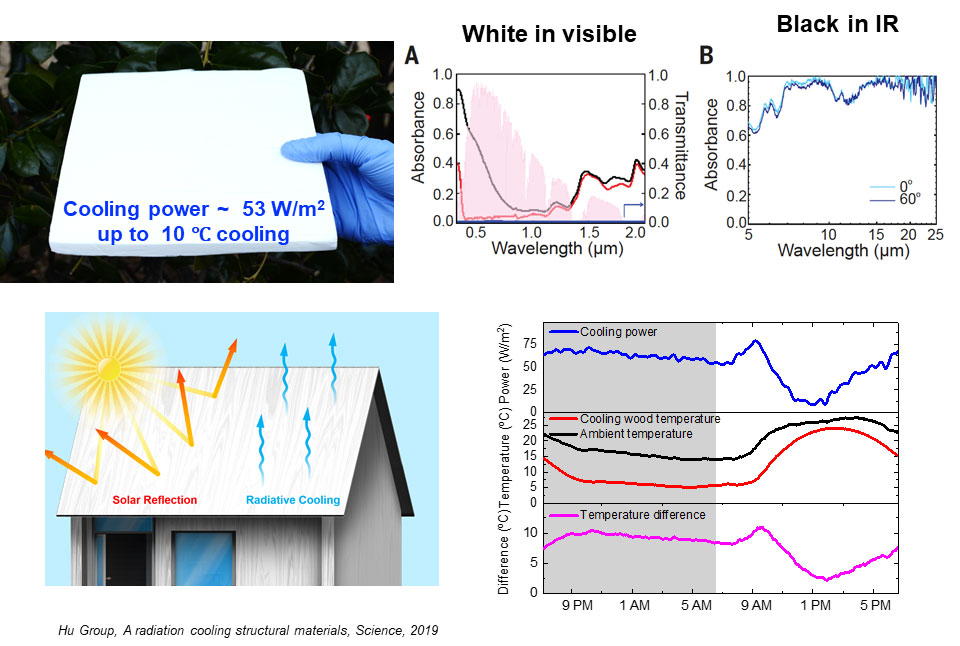
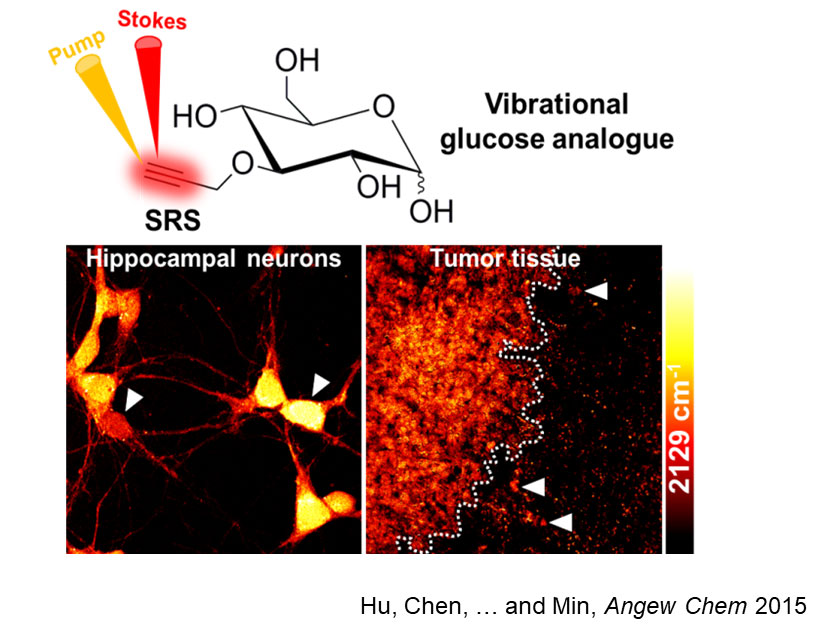




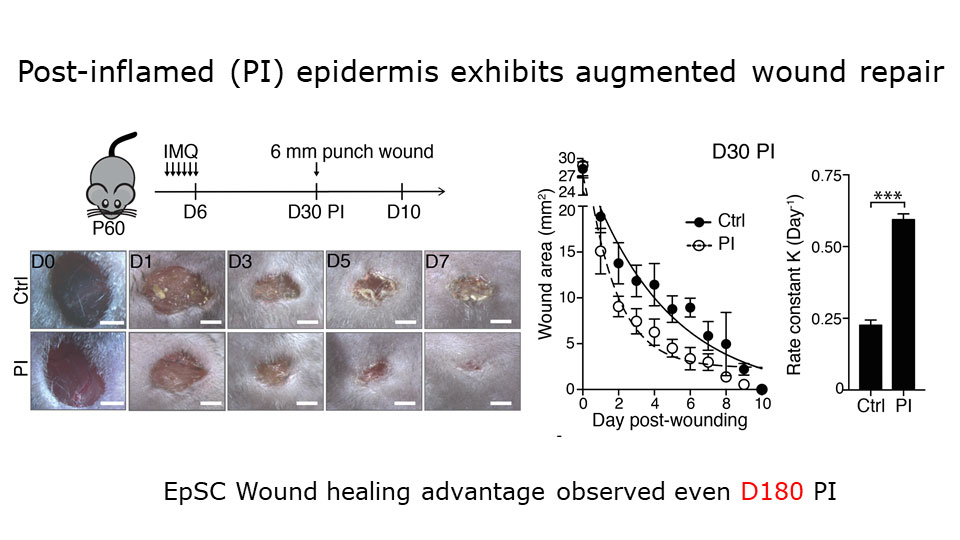
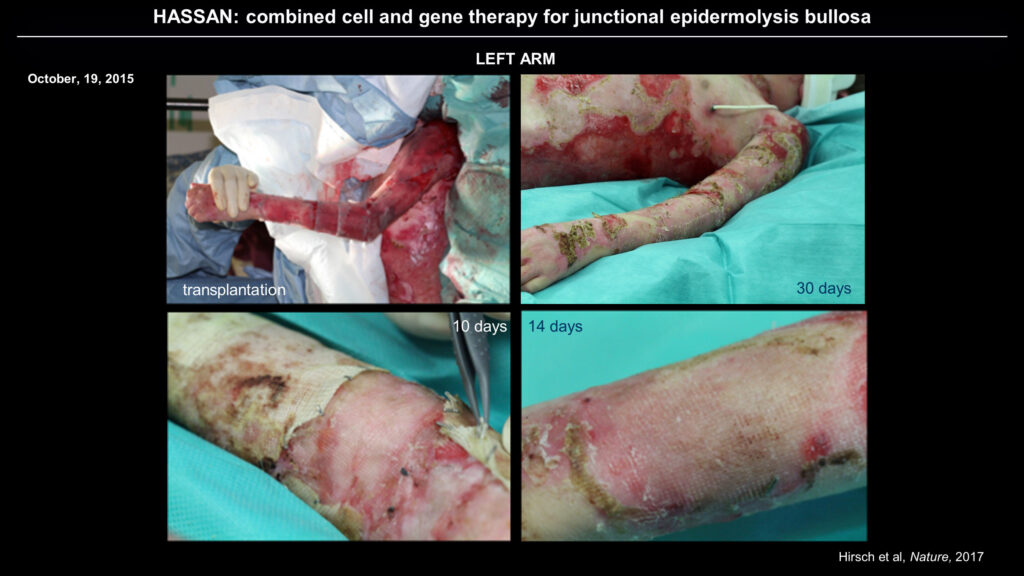
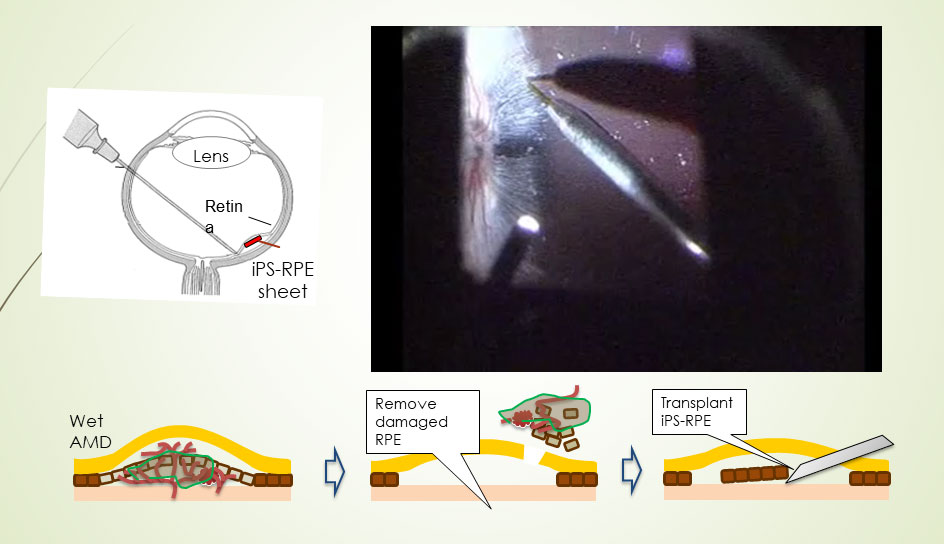
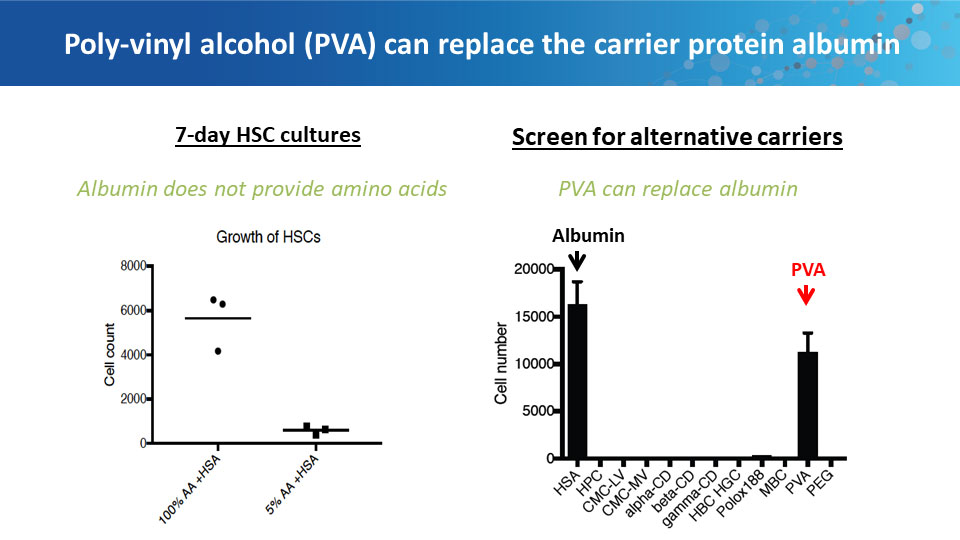
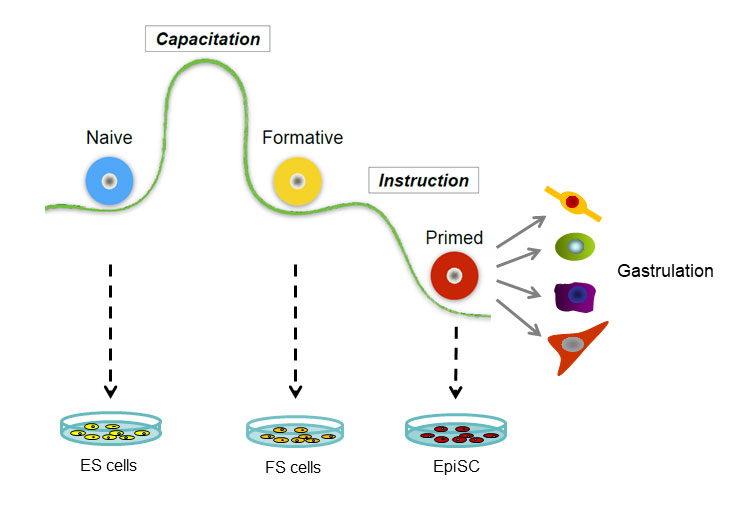
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}