The neuroscientist and former Academy board chair broke scientific and social ground throughout her long career.
Published January 11, 2012
By Diana Friedman
Fleur L. Strand, a physiologist who was a pioneer of the neuropeptide concept, died of cancer on December 23, 2011, in her home in Snowmass Village, Colorado. She was 83.
Strand was actively involved in The New York Academy of Sciences throughout her career, being named a Fellow in 1976 and being elected as chair of the board in 1987. Both her leadership and her friendship will be missed by the Academy community.
Most recently, Strand held the title of Carroll and Milton Petrie Professor of Biology and Professor of Neural Science, Emerita, at New York University (NYU), where she retired in 1997. After her retirement, she was appointed by Governor George Pataki to the New York State Spinal Injury Research Board in 2001 and served as a consultant for several pharmaceutical companies until 2010.
Throughout Strand’s illustrious career, which began at NYU, where she received her BA, MS, and PhD degrees, she broke new ground, both in research and the role of women in science. In 1957, she received a National Institutes of Health postdoctoral fellowship to study at the Physiological Institute of the Free University in Berlin, Germany. During these early years of research, Strand was the first to show that stress-evoked hormones could have a direct effect on the peripheral nervous system, independent of the classical role of the adrenal gland. It took a number of years for the scientific community to accept the concept of neuropeptides.
First Female Department Chair
Following her postdoctoral research in Berlin, Strand returned to NYU in 1961 and was appointed to a faculty position in the Biology Department. In 1980, she became the first female chair of the department. Strand remained an active researcher in the field of neuropeptides, as well as a beloved teacher and mentor, at NYU for 36 years. During this time, Strand sponsored more than 80 graduate student dissertations, authored multiple textbooks and primary research and review articles, and co-founded several professional societies, including the International Neuropeptide Society.
In her personal life, Strand enjoyed a long marriage to her husband of 65 years, Curt Strand. Curt Strand is a retired CEO of Hilton International. The couple enjoyed many years of vacationing in Snowmass Village, Colorado, before moving there full-time in 2004. A memorial celebration for Strand will be held on February 24 at the Snowmass Club.
Science is a discipline that whittles the abstract into clear and precise terms. So it might seem odd, at first, that Elias Zerhouni, former director of the National Institutes of Health and esteemed scientist, takes issue with certain characterizations.
“I don’t like to call something, ‘basic science’ or ‘translational science,’” says Zerhouni, a member of the Academy President’s Council. “It’s either good science or bad science. I don’t think we should characterize any type of science. Science is an adventure; it’s the human search for knowledge and new ideas that can better humankind. To pigeonhole types of science is, in my view, not beneficial.”
Definitions can create barriers, says Zerhouni. And he has spent his life stepping over such lines, first in academia at Johns Hopkins, then at the National Institutes of Health, and now in private industry in his recently assumed role as president of global research and development at Sanofi-Aventis.
In the early days of Zerhouni’s career as a radiologist at Johns Hopkins, he recalls not being able to secure NIH funding for his own research, because it didn’t fit neatly into a single disease process or under the purview of one single NIH institute. It took private industry funding to make his proposed research path—which years later led to imaging technologies that could show the heart in three dimensions and help clinicians decipher between cancerous and noncancerous nodules in the lungs—a reality.
Funding Reform
Zerhouni got the opportunity to make changes in the way the NIH chooses and awards research grants when he was appointed NIH director. He assembled a multidisciplinary team and a “Roadmap for Medical Research,” which isolated areas of science that would most benefit from cross-collaboration. The NIH Reform Act of 2008 established the NIH’s Common Fund, specifically for research that involves at least two of the 27 institutes in the NIH. In addition, it also set up funds for the Pioneer Award, which supports individual scientists of exceptional creativity who propose pioneering, and possibly transforming, approaches to major challenges in biomedical and behavioral research, despite not fitting neatly into a single disease category.
“You need a diversity of approaches,” Zerhouni says. “Sometimes funding agencies use a one-size-fits-all approach, which doesn’t help the real nature of science, which can go from the proverbial single investigator in the lab doing fundamental observation…to having the ability to put together teams to understand computational biology and bioinformatics. So in my view, the funding agency should reflect the realities of science and not the other way around.”
During his time at the NIH, Zerhouni encouraged further collaboration between scientists by creating multi-principal investigator grants, which allowed each scientist on a project to have lead investigator status. “Under a single lead investigator system, everybody else would be secondary. Well, that, in some way, discourages collaboration because everyone wants to be recognized in their own field as the top scientist.” The multi-PI grant gave scientists equal billing to contribute to the scientific problem at hand—and to converge in the same way as science does.
Matter of Perspective
Zerhouni attributes his success, in part, to his own unique background. Algerian-born, Zerhouni came to America when he was 24, after securing a residency at Johns Hopkins. He quickly learned the role perspective can play in the world of medicine.
“I think maybe part of my ability to succeed here is that I can bring a viewpoint that many people feel is sometimes surprisingly different and constructive in showing there is a different way,” says Zerhouni. “I think being an immigrant enriches the mix.” He applauds the U.S. for welcoming scientific immigrants and their contributions, pointing out that science is the great peacemaker.
Zerhouni cites the fact that 30% of all Nobel Peace Prizes in Medicine have been won by immigrant Americans. “No country has all of the talent to overcome its problems and that’s why I think science has to be global, it has to be without artificial barriers, and we should encourage collaboration and self-assembly wherever it comes from, provided that it is good science.”
About the Author
Marci A. Landsmann is a medical writer in Philadelphia.
Academic and industry researchers, technology developers, and clinicians discuss the progress and the challenges in the field of personalized cancer medicine.
Published December 1, 2011
By Jamie Kass
Personalized medicine, the treatment of patients based upon their individual genetic, epigenetic, and phenotypic makeup, is the ultimate goal of many researchers and clinicians trying to find less toxic and more effective therapies for cancer. While cancer as a whole is characterized by uncontrollably proliferating cells, the disease is being subdivided into increasingly smaller units, from organ-specific to gene-specific categories.
An understanding of the molecular basis of some cancers and an increasing knowledge of how those cancers differ from those in other organs and in other individuals have led to the development of drugs enormously successful at treating those types of cancer. Yet many other candidate drugs based on the same kind of analysis fail in the clinic, leaving cytotoxic chemotherapy still the standard treatment for many patients.
From May 19-21 2010, academic and industry researchers, technology developers, and clinicians from around the world gathered in Barcelona, Spain, to discuss the progress and the challenges in the field of personalized cancer medicine. A special technology workshop highlighted the important role of technological advances in driving the efforts toward personalized medicine. Conference participants also discussed their concerns about the field, in particular the failure of the U.S. clinical trial system to keep up with the changes demanded by the new approach.
Researchers have made great progress in discovering the cellular processes that have become pathological in cancer. For example, it is clear that genetic and epigenetic changes that affect cell proliferation, DNA repair, programmed cell death, stem cell maturation or self-renewal, and other fundamental cellular and molecular activities can lead to cancer formation.
Systemic Problems, Clinical Medicine, and Technology
New information is also coming to light about more systemic problems, such as the survival of cancer cells in different microenvironments, the cells’ ability to stimulate angiogenesis, and the way they promote their own survival by interacting with noncancerous cells to acquire nutrients, suppress immune response, and meet other important needs. The most cutting-edge research in all of these areas was discussed by leading researchers in the field.
Moving toward clinical medicine, researchers discussed how oncogenomics and tumor profiling can reveal the signaling pathways mutated in a particular tumor type as well as the variability among tumors within that type. Breast cancer researchers are at the forefront of efforts to use gene expression signatures and other molecular data to guide treatment, predict risk, and understand epidemiological phenomena. There are several clinical trials underway to test some of these new tools, some of which were presented in talks about efforts to identify biomarkers for prognosis and treatment response.
The conference also delved into a variety of approaches to developing targeted therapies for cancer. Some of these efforts take advantage of technologies that allow high-throughput analyses of genomic information and drug responses in cell culture. Others use preclinical mouse models to evaluate candidate target therapies or to counteract the drug resistance that often thwarts cancer treatment. Next-generation sequencing and microarray technology have also played an important part in the advance toward personalized cancer medicine, as a technology workshop highlighted.
“We want to know why, for example, not all tumors respond to vascular endothelial growth factor inhibitors. We want to understand resistance.”
Published December 1, 2011
By Diana Friedman
Napoleone Ferrara (center) receives the 2011 Dr. Paul Janssen Award for Biomedical Research with (left to right) Joaquin Duato (J&J), Craig Mello (University of Massachusetts Medical School; Howard Hughes Medical Institute), Harlan Weisman (J&J) and Paul Stoffels (J&J).
Napoleone Ferrar, a Genentech Fellow, discusses his life’s work: from discovering the core angiogenic signaling molecule, vascular endothelial growth factor (VEGF), to creating anti-VEGF therapeutics for wet age-related macular degeneration and cancerous tumors.
What motivated you to go into research?
I studied medicine in Catania, Italy, my hometown. Initially I thought that clinical medicine was very interesting, but I didn’t have a firm direction. Then, I met a professor of pharmacology with an established research group. I joined this group as a medical student and that’s what introduced me to research. It was thanks to my post-doctoral mentor at University of California, San Francisco, that I was able to further hone my research interests. Both of these people were very influential and inspirational factors.
Broadly, how did you identify VEGF and identify its role?
I was interested in endocrinology and neuroendocrinology. The pituitary is the master regulator of many key physiological processes. During my fellowship at UCSF, I stumbled on a population of pituitary cells without an established function. As part of my postdoctoral work, I tried to characterize these cells. I found that they released a factor that promotes angiogenesis. Over time I was able to isolate this molecule: I named it vascular endothelial growth factor (VEGF). After that, and through the work of a number of other labs, it became clear that VEGF is a very important signaling molecule.
As your work progressed, what were your biggest challenges in translating your discoveries to the development of therapeutics?
We were very fortunate that we found the right target but the challenge was proving that. Initially there was a lot of controversy about angiogenesis. There was skepticism about VEGF’s role in angiogenesis; people thought that maybe there were other molecules at work. We had to prove our findings through sound scientific methods.
What factors have contributed to your success?
I have a medical background even though I have not been a practicing physician for a long time. Perhaps that medical background helped me to guide my research into an area that is therapeutically relevant. I was also just very fortunate that the VEGF molecule turned out to be so important. Being at Genentech for 22 years helped push my work along. I think it would have been difficult to do the same work in a different setting.
You recently received the 2011 Dr. Paul Janssen Award for your breakthrough research on VEGF, and in 2010 you received the Lasker Award. What do these awards mean to you?
They express the fact that my peers, my colleagues, respect this work, so that means a lot to me personally. But the awards also reflect on the work that my group has done over the years. To me, these awards are really a stimulus to do more. I see them as motivation to do more and better research.
What are your biggest research priorities right now?
We’re trying to follow up on our work on VEGF. We want to know why, for example, not all tumors respond to VEGF inhibitors. We want to understand resistance. This will mean dissecting tumors to refine our understanding of angiogenesis. Regarding pro-angiogenic therapies, clinical studies thus far have been quite disappointing. It’s very difficult to reconstruct complex vessels to positively impact circulation. It would be really wonderful if someone could figure out how to do that.
This story originally appeared in the Fall 2011 issue of The New York Academy of Sciences Magazine.
Academic medical center must continue to bring together clinical and scientific resources, in the service of bettering humankind.
Published December 1, 2011
By Diana Friedman
“I don’t like the distinction between basic and translational science; science should be seamless,” says Laurie Glimcher, the Stephen and Suzanne Weiss Dean, Weill Cornell Medical College, effective January 2012. Many of her colleagues in the academic medical center community support Glimcher’s viewpoint.
“No matter what we call the discovery and development of new therapeutic drugs, it’s critical for the future of patient care that we focus on breakthroughs in therapeutics,” says Kenneth L. Davis, president and CEO, Mount Sinai Medical Center.
For Glimcher, who spends the majority of her professional life in a laboratory, her training as a physician still informs her desire to translate laboratory discoveries into viable clinical treatments. This is the quintessential mission of an academic medical center: to bring together clinical and scientific resources, with a greater duty of service to humankind. This mission is further supported by the Bayh-Doyle Act, a federal mandate that requires academic medical centers to develop discoveries at the bench into benefits for patients, notes Glimcher.
In order to move translation forward, clinicians and scientists must interact. “We need great clinicians who understand how to interface with laboratory scientists, we need scientists to ask research questions that are relevant to disease, and we need bridges that connect the two groups,” says David S. Stephens, vice president for research, Woodruff Health Sciences Center, Emory University. “This happens in academic medical centers, but it doesn’t happen well in all of them.”
Medical Model of Choice
“We have never lived in a time when opportunities were greater in biomedical research,” says Davis. And, as pharmaceutical interests increasingly move from discovery to development, academic medical centers must play a leading role in seizing these opportunities.
Jeffrey Bluestone, executive vice chancellor and provost, University of California, San Francisco (UCSF), believes that one way to greatly increase translation is to focus “our incredible science on humans as the complex medical model of choice.”
“To me, one of the most exciting post-human genome and technology advancements is thinking about the human organism as a place to do cutting-edge research, just like mice were our organism of choice in the past.” To do that, says Bluestone, academic medical centers will need to engage faculty and students in areas of human biology while improving existing infrastructure (data and tissue banks, bioinformatics technology, etc.) so that it is up to the task of human research.
Incentives Needed
Despite the incredible research opportunities afforded by an increase in scientific knowledge, academic medical centers face many challenges that make the realization of translation an uphill climb. Declining Medicare and Medicaid reimbursement leads to clinicians with packed patient schedules, leaving less time for vital collaboration with laboratory-based scientists, who are themselves faced with a dearth of research funds.
“Ninety-three percent of grants are turned down. A basic scientist will write their best grant in the area with which they are most comfortable and often that isn’t an area of disease,” says Davis. This underscores a critical need in academic medical centers: finding ways to incentivize both laboratory-based scientists and clinicians to spend more time working together and, ultimately, to make progress in creating new therapeutics for disease.
Many academic medical centers are providing incentives on an institutional level, by investing large amounts of financial and organizational resources to create physical spaces that support the day-to-day process of translation. For example, new buildings are being created at Weill Cornell Medical College and Mount Sinai Medical Center to foster closer collaboration between clinicians and laboratory-based scientists, blurring the lines between such disciplines to create the ‘seamless science’ of Glimcher’s vision.
Putting scientists and clinicians from diverse disciplines and backgrounds in close proximity to each other is useful both for its practicality and its ability to drive culture change. “Many of our faculty are used to, and very successful at, working independently or with a few collaborators,” says Bluestone. “We need to find ways to allow faculty to overcome barriers to communication and collaboration.” Having a building where scientists, clinicians, and students with varying degrees and areas of expertise work side-by-side is one way to facilitate a free exchange of information and ideas.
Reaching Out
In addition to new initiatives that pool intra-institutional resources, partnerships between academic medical centers are key, says Glimcher. “Here in New York, we have the so-called four corners—New York Presbyterian, Memorial Sloan Kettering Cancer Center, Weill Cornell Medical Center, and The Rockefeller University. We all have unique strengths, so we want to leverage those to avoid duplicating efforts. It’s more cost effective.”
At the Atlanta Clinical & Translational Science Institute (ACTSI), partnerships span three academic institutions—Emory University, Morehouse School of Medicine, and Georgia Institute of Technology—as well as a variety of health care and non-profit partners. All of these organizations pool resources “to rapidly and efficiently translate scientific discoveries to impact all populations of the Atlanta community,” says Stephens, who is the institute’s principal investigator.
Often, the results of these initiatives reach well beyond Atlanta. For example, ACTSI scientist Bali Pulendran recently published a systems biology approach to determine innate and adaptive responses to influenza vaccination, providing a new platform to predict vaccine immunogenicity and establishing new mechanistic insights for vaccine development.
Educating the Educators
Another way to incentivize both scientists and clinicians to expend more time and professional resources on the development of disease-modifying compounds is to provide professional education that emphasizes the skills necessary for translation. Some schools now offer master’s degrees in clinical sciences or translational science, in which physicians learn to become clinical researchers.
UCSF, a health sciences campus, recently developed ties with a local law school to help researchers learn about issues such as conflict of interest and consent forms. And ACTSI hosted a forum, in partnership with industry, to teach laboratory-based scientists about the process of creating a therapeutic product—an area most of those in attendance had never learned about before.
Such ties with industry are vital to avoiding the so-called valley of death—that stage where development of a previously promising compound languishes and dies—says Bluestone. “We need a different model of partnership with industry. Not one where industry licenses a drug from us and they tell us to go away, or one where industry provides us with money to do research and we tell them to go away.” At UCSF, Pfizer locates full-time scientists on the university campus, leading to greater interaction and better understanding of both sides of the process—discovery and development.
Industry collaboration is incredibly valuable, agrees Glimcher, provided there is full transparency from all sides. “In the olden days, basic scientists looked down on clinical researchers,” says Glimcher. “It’s not so different from how academics used to perceive industry. I believe those distinctions are largely being erased. Many of my esteemed colleagues have crossed over from academia to industry and vice versa. I think that’s a positive thing, so long as there’s transparency.”
A Unique Advantage
Indeed, collaboration, both within and outside of academia, is necessary to overcome translational hurdles. The potential rewards are great. But, says Bluestone, academic medical centers do not have to look beyond the borders of their campuses to find two of their most valuable resources: students and patients.
“Our students are tremendous resources that drive innovation and creativity,” says Bluestone. “They can help us challenge the status quo.”
At ACTSI, researchers interact regularly with community boards, set up to provide a forum for two-way communication and to engender trust between community members/patients and the institute. “The community boards allow us to reach out to communities about our research projects, but they also allow communities to contribute to us by telling us about their unmet clinical needs,” says Stephens.
Targeting research, and subsequent drug development, to unmet health needs is perhaps the best example of how academic medical centers can make a real-life difference through translation.
George Thibault and the Josiah Macy Jr. Foundation help the Academy push progress around medical education for the public good.
Published September 1, 2011
By Noah Rosenberg
George Thibault
George Thibault knows as well as anyone that medicine is an ever-evolving frontier, continuously fraught with new challenges that demand innovative solutions. In fact, Thibault, president of the Josiah Macy Jr. Foundation and an Academy governor, is the first to admit that his medical school education at Harvard would, by itself, be insufficient in today’s medical world.
“Health care professionals,” he says, “now need different kinds of experience to prepare them for a very different world than the one I was prepared for when I finished my training.”
Thibault stresses that the health care system evolves so quickly that current health care professional training, in certain respects, is often obsolete by the time a graduate enters his or her chosen field. Factors such as the diversification of patient demographics, the rise of chronic disease, and the shift in care delivery from hospitals to community-based interventions make for a model in flux.
“Educational programs,” he insists, “need to catch up with those changes.”
Thibault and the Josiah Macy Jr. Foundation, recently partnered with The New York Academy of Sciences (the Academy) to create the Translational Medicine Initiative. A three-year partnership that began in early 2010, the initiative fosters discussion and collaboration among physicians and basic researchers, industry and academic scientists, and public health experts, among others in the medical arena. The goal is to enable participants to learn from recent scientific breakthroughs, receive career development in translational medicine, and, ultimately, decrease the time needed to convert basic science into clinical applications.
Shaping the Future of Science
The partnership is accomplishing nothing less than helping to “shape the future education, research, and clinical care practices of thousands of physicians, scientists, and educators around the globe.” This is achieved through programs like the Translational Medicine Discussion Group—a forum for distributing information to the larger scientific and medical communities—and partnership-sponsored Academy memberships for medical school students and clinical fellows, which expose them to cutting-edge discoveries and enhance their delivery of care. Additionally, the Translational Medicine Initiative, whose findings are disseminated via simulcast webinars, multimedia eBriefings, podcasts, and articles in Annals of the New York Academy of Sciences, grants students access to the Academy’s Science Alliance events, which provide non-traditional career development opportunities.
The Translational Medicine Initiative, Thibault says, goes hand in hand with The Macy Foundation’s simple yet lofty goal: improving the health of the public through improving health professional education, a philosophy that was at the core of Thibault’s esteemed career as a Harvard physician and educator. He spent more than 40 years with the university, in posts including founding director of the Academy at Harvard Medical School and chief medical officer at Brigham and Women’s Hospital, and he has brought his educational values and beliefs with him to The Macy Foundation.
“We’re not abandoning what we’ve done before,” Thibault says of progress in the industry, “but we need to do more and improve upon it for this different health care system, delivery system, and patient population.”
“We’re building on the excellence of the past but adapting it to a changing world,” he says.
Creating a Healthier Society through Empowerment
After all, Thibault explains, the irony of medical training is that physicians traditionally spend most of their education alongside classmates in their particular specialty as opposed to those in complimentary fields with whom they will spend most of their careers.
“We think more of the educational process should be learning with and from other health professionals,” he says, noting that The Macy Foundation has received commitments from more than 15 schools and six major professional societies—including nursing and medicine— who recognize the importance of making joint-curriculum planning “the educational paradigm for the future.”
At the end of the day, however, Thibault is careful to note that while The Macy Foundation’s strategy has certainly adapted over the years, its core mission is as strong as ever: creating a healthier society by empowering the professionals who live and breathe medicine. “We don’t have enough resources ourselves to bring about the changes we want to see,” Thibault says, “so a large part is communicating ideas and getting others to pick up ideas. Ultimately, we have to go beyond what we alone as a foundation can do.” The Translational Medicine Initiative does just that, lending Academy resources to The Macy Foundation’s mission.
From the research lab to the movie set, Columbia University’s W. Ian Lipkin lends his public health expertise to the pandemic thriller Contagion.
Published September 1, 2011
By Diana Friedman
W. Ian Lipkin at the New York City premiere of Contagion on September 7, 2011. Photo courtesy of Dave Alloca via Starpix.
W. Ian Lipkin, The John Snow Professor of Epidemiology at Columbia University’s Mailman School of Public Health, recently found himself mentoring a new kind of student—the Hollywood variety. Lipkin, also director of the Center for Infection and Immunity, served as senior technical advisor for Contagion, the pandemic thriller released in September 2011. The advising process started three years earlier, when the Academy member was recruited to work on the big-budget film.
Why did you sign on as an advisor for Contagion?
I had been asked to review movies in the past and most of the time, my reviews were negative. This was the first time I signed on to help in the creation of a movie. I was very impressed with the screenwriter, Scott Z. Burns, because he came to this with no preconceived notions. Both Scott and the director, Steven Soderbergh, were committed to a strong scientific foundation (incidentally, they’re both kids of academics, so they grew up in that tradition).
Additionally, the movie provided a unique opportunity to educate millions of viewers about the challenges—scientific, political, economic, logistical, and humanistic—of emerging infectious diseases, and the opportunities we have to address them.
How does the topic of the movie relate to what you do on a daily basis?
Our Center is known for its work in pathogen discovery, surveillance, diagnostics, and immunotherapeutics. We have programs in the developing world, including one focused on the Nipah virus, the inspiration for the virus in the film.
In which aspects of the movie-making process were you involved?
I presented several scenarios for the pandemic, and recommended the one that was selected. Thereafter, Craig Street, a bioinformatician at the Center for Infection and Immunity, and I designed the virus by downloading existing viral sequences from a GenBank database and stitching them together. We then created three dimensional virus models based on structures of Nipah and Hendra, which were solved by Bowden and colleagues at Oxford, and described its evolution over the course of the pandemic.
I also helped with dialogue; made suggestions for props, set, makeup, and costume design; helped to train actors in the specifics of laboratory work; and connected the crew and cast to laboratory and public health scientists for expertise and insights I could not provide. We also recorded portions of the soundtrack at Columbia—biocontainment doors opening and closing, whirring centrifuges, cages rolling down hallways.
Do you feel that the finished movie accurately represents the work of an infectious disease scientist?
Consultants don’t, nor should they, have control of the finished work. Nonetheless, I am pleased with the outcome and the feedback from my colleagues has been positive too.
There are minor issues like the time from virus discovery to having a vaccine might be six months rather than four, or that the incubation period is too short. But by and large, the movie is scientifically plausible. Furthermore, it shouldn’t take six months to make and distribute a vaccine. We can do better.
How does this film address the issue of translational science?
In this film, we’re trying to engender interest in supporting translational work: developing vaccines, drugs, and diagnostics to reduce the impact of disease.
We think this film is timely because there is a threat to science funding at all levels: state, federal, and global. This film makes the case for why it’s important to not only maintain support, but increase it. The risks are too great.
What are your biggest professional priorities when faced with a new microbial threat?
I start out with a series of questions: What is it? Where did it come from? How is it transmitted? What does it do and how? Where is it going? Is it stable or is its pathogenicity changing? Is everyone equally vulnerable, and if not, why not?
My action items include answering the questions, building and implementing diagnostic tools for clinical management and surveillance, and establishing countermeasures.
The authority to make claims about food and bodily knowledge was not always so squarely situated in the hands of professional physicians and nutrition experts. In fact, as Harvard historian of science Steven Shapin explained in his January 26, 2011 talk at The New York Academy of Sciences (the Academy) titled You Are What You Eat: The Long History of Knowing about Our Food, Our Bodies, and Ourselves, Europeans from antiquity to the early modern period, while seeking advice from experts in many aspects of their daily lives, remained very much their own physicians.
These Europeans lived in the era of a branch of Western medicine known as dietetics. Unlike its sibling disciplines of diagnosis, prognosis, and therapeutics, dietetics was “not just called into play when [one] was manifestly unwell.” Instead, this particular and, it should be noted, remarkably stable body of knowledge focused on maintaining as well as restoring health through balance and moderation of the elements at play. Intricately connected to daily routines, behaviors and practices, dietetics was associated with the concepts of “regimen” and “hygiene,” and it prescribed an ordered, balanced life for its adherents.
These values might resemble, for example, aspects of certain modern cultural or religious traditions, but they are a far cry from the realm of modern medicine and present-day nutritional science, according to Shapin. Whereas a modern nutrition expert might advise you to “reduce your fat intake,” and a modern physician might prescribe medications to help you reduce your cholesterol, a 17th century dietetics expert or a reader of dietetic texts (or “dietaries” as they were known) might suggest you eat foods that match your “temperament,” including high-fat foods as long as they taste good.
The History of Dietetics
Delving into the history of dietetics is a fascinating journey in its own right, but there are other motivations for studying a set of historical practices now so divorced from our own lives, as well. If the history of dietetics provides us no useful framework for considering our present reality, why study it at all? The answer is relatively simple, as Shapin made clear.
Understanding the history of dietetics tells us a great deal about how people have thought of themselves in relation to their food and their surroundings. Furthermore, because of its unique blending of ethical and instrumental authority, dietetics and the course of history from that body of knowledge to modern medicine can help us comprehend how European societies came to segregate knowledge into the prescriptive and the descriptive, separating “what ought to be” from “what is.”
As scientific concepts of nutrition took over in the early 19th century, substantial authority was invested in these new scientific disciplines to speak about aspects of daily life that were formerly the domain of dietetics. How and why this change occurred are fundamental questions to the study of our own contemporary relationship to our food, to our bodies, and to the experts who study them. And so, as it turns out, the premise of our earlier question is flawed: the history of dietetics has much to say about our current condition.
What is (or was) Dietetics?
During his talk, Steven Shapin had the unenviable task of rendering familiar the vocabulary and the culture of dietetics, which was so pervasive as to be a “coordinating mechanism [for many aspects of life] in the late Middle Ages, even for ‘non-experts,'” but which today is a worldview entirely foreign to our own. He accomplished this feat by relating for his audience the fundamental principles of dietetics and by explaining the intuitive and perceptual ways individuals could access dietetics knowledge.
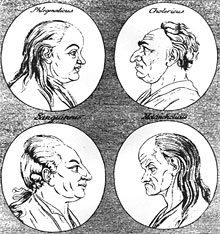
An 18th century illustration showing the different “complexions” (or temperaments: sanguine, phlegmatic, melancholic, and choleric) that result when each of the four humors dominates.
At its most basic, dietetics relied on the notion of four principal “elements” (air, water, earth, and fire) composing the physical world—everything from rocks to flies to humans to food. These four elements mapped onto four bodily “fluids,” or humors, respectively: the sanguine humor (blood), the phlegmatic (phlegm), the melancholic (black bile), and the choleric (yellow bile). To these fluids belonged certain qualities in different combinations.
For instance, yellow bile was believed to be both dry and hot, the qualities of the element fire. Inscribed in the combinations of four qualities, dry, hot, moist, and cold, one could find four personality types, one for each of the dominant humors. To this day, we can describe someone prone to anger as both “hot headed” and “choleric,” reflecting the cultural legacy of these concepts.
Adjusted for Each Person’s Specific Temperament
These qualities and personality types (also called “temperaments” or “complexions”) were maintained in health through balance and moderation. One should, according to dietetic advice, consume “hot” and “dry” foods to restore health when sick with “cold” and “moist” illnesses. To maintain health, one should match the food one consumes with one’s temperament. For instance, those of choleric tendencies should eat mostly foods with “hot” and “dry” qualities.
And because dietetics considered everything in terms of these same four qualities, it provided an integrative and coherent vocabulary that allowed for the description of relationships between diseases and their treatments, or people and their food, for example. This vocabulary and its corresponding culture of practice reached far into the fabric of everyday life; according to Shapin, “it belonged to you in ways that other science [does] not.” Dietetics advice could involve proscriptions against certain types of foods, but it could also venture into areas quite beyond the domain of modern nutritional science.
Shapin spelled out the areas on which a dietetics expert could advise, the realm of which included all the areas of someone’s life that could be altered in some way. These “six things non-natural” consisted of one’s airs (one’s surroundings), food and drink, motion and rest, sleep or waking, evacuations (including excretion, retention, and sexual release), and the passions of one’s soul (the emotions).
This list broadly encompassed many of the practices of everyday life and could include where someone should go on vacation or which direction his house should face, to name a few examples. Dietetic prescriptions were adjusted for each person’s specific temperament, so that a melancholic person (with a cold and dry temperament) was not constantly trying to counterbalance his or her temperament with sanguine treatments or vice versa.
The Good and the Good for You: The Instrumental and Ethical Authority of Dietetics
At this point it might seem that dietetics, insofar as it involved the treatment of disease through prescriptions for behavior changes, is not that different from aspects of modern primary care. However, dietetics can be distinguished on a number of fronts from the body of knowledge and the culture of practice belonging to modern medicine. Chief among these is “the way dietetics stood with respect to what was medical or scientific on the one hand and [to] what was moral on the other,” noted Shapin. For, as he explained, dietetics sat at the boundary of description and moral prescription.
Dietetics advice was therefore both instrumental and ethical in nature. The dietetic values of temperance and moderation, expressed in prescriptions such as “live to the golden mean” or “nothing too much” did not just resemble the four cardinal virtues of prudence, justice, fortitude, and temperance, they affirmed them. Dietetics told people not just what was good for them (nutritionally, physically, mentally, etc.), but also what was good morally. Those who followed such direction would benefit materially, through the maintenance of their health, but also morally, through the affirmation of ethical truths.
“You are What You Eat”
“You are what you eat,” the phrase that began Shapin’s talk, takes on a level of meaning in this dietetics context beyond what is available in modern nutrition science’s vocabulary of “constituents.” People were characterized in the same way as their food, and just as knowing the correct description of someone’s qualities would lead you to the right description of their nature, knowing the right descriptors (hot, cold, moist, dry) for their food would tell you its nature as well. Knowing the nature of your food would allow you to predict how it would interact with your digestive system and whether it would make you sick, among other aspects of its behavior.
Furthermore, this analysis could be used to understand not simply the nature of people in the present, but also how they retained that temperament over time and what practices might drastically disrupt that nature in the future. In this way, custom was thought of as a second nature because people believed that a lifetime of custom, of eating behaviors and the like, could remake someone’s nature. In this framework, one had good reason to fear radical changes to lifestyle or drastic imbalance of the humors, and maintenance of that balance through dietetics knowledge became all the more important.
Dietetics and Expert Knowledge
Given the implications of a humoral imbalance, early modern Europeans clearly needed a reliable source of dietetic knowledge, but that source could be found surprisingly close to home. Although the “dietaries” written by dietetic experts were one avenue of access to dietetics knowledge, self-knowledge and experiential knowledge were both extremely important parts of the culture of dietetics.
In an era where independent testing of blood pressure, heart rate, or any of the metrics so fundamental to modern primary care was unheard of, even the most expert physicians were very much dependent on the patients’ accounts of their own behaviors and symptoms. Even the treatments for illness were largely in the patients’ hands, as medications took a back seat to lifestyle adjustments.
But early modern Europeans could get by without seeking advice from experts at all, explained Shapin. In most instances, non-experts could reliably deploy dietetic knowledge simply by engaging in what Shapin called “analogical forms of reasoning” to relate the superficial (or obvious) characteristics of food to the qualities of its nature and consequently, to the food’s fate as it was digested, to whether it would make a particular person unwell. Most of these superficial qualities could be reliably ascertained through intuitive descriptions of the food’s texture, general appearance, and so on. A cantaloupe, for example, would be considered “cold” and “moist,” and a chili “hot.”
Quod Sapit Nutrit
Of the ways to determine whether and how a particular food would match one’s own qualities, taste was crucial. The Latin saying “quod sapit nutrit,” meaning “if it tastes good, it’s good for you,” was not a playfully insincere justification for indulgence, as it might be today, but was instead a rule of thumb for assessing the goodness of food. In general an aliment agreed with someone—that is, made him well, not ill, if it sat well on the stomach—if its qualities matched his temperament, and the same principle applied in the mouth.
What tasted good on the tongue clearly matched the tongue’s, and therefore the person’s, nature. In this framework, because the perceived qualities of the food and the nature of that food were identical; the categories of being and of experience were one and the same. And more importantly, as Shapin put it, “the tongue [was] a reliable philosophical probe into the nature of things.” Not since has the role of the tongue been quite as authoritative as it was in dietetic culture.
The Rise of “Constituent” Descriptions
Smell, taste, and other everyday experiential ways of knowing have become “philosophically devalued” with the disappearance of dietetics from formal medical training in the 1810s and 1830s and eventually from lay consciousness, according to Shapin. Although they are the vehicles for the study of art and beauty through connoisseurship, these senses are no longer thought to be reliable probes into the nature of things. Dietetics and its ontology of “qualities” gave way to the beginnings of modern nutritional science and, with it, to a world of “constituents,” such as proteins, carbohydrates, and fats.
Such a drastic change first in the content of professional medical education and then in the public understanding of concepts as fundamental as which foods are beneficial did not happen over night. To begin to think of foods in terms of what they were made of instead of in terms of their qualities took a great deal of adjustment. Initially medical doctors, trained in the burgeoning discipline of chemistry, began to describe foods in terms of their sweetness, alkalinity, acidity, and so forth. These descriptions were constituent-based but were nonetheless available in some respects to the lay public through personal observations and sensory experience.
Fuel versus Non-fuel
William Prout in the 1810s and Justus von Liebig in the 1830s, both chemists by training, helped move the authority to make claims about foods’ components further out of the reach of the untrained public. Liebig in particular thought of the body as a kind of engine in which digestion was one mechanical process among many. And, like an engine, the body required materials to construct it and “fuel” to run it.
The distinguishing feature of “non-fuel” for him was the presence of nitrogen—an assessment that could clearly only be made by chemical examination. Of course, today this category of “nutrients” includes much more than nitrogen-containing substances, but it is no less in need of chemical interpretation than it was in Liebig’s era. Ideas of fuel have not left public discourse, though from that century to this, calories have come to mean “the power of food” rather than something contained within it.
Evidence for the present-day centrality of scientific interpretation can be found in what Shapin called “one of the great artifacts of the role of the state and the relationship of expertise—the Nutrition facts label.” This label, required on all processed, purchasable foods, indexes “the achievements of nutritional science,” and most of its details are only known to the consumer on the condition of expert knowledge.
Without the testing and re-testing of foods by scientific experts, we cannot know, for example, the iron content or carbohydrate content of the foods we consume. And this reliance on one set of experts cements our dependence on yet another set—we cannot be our own physicians in the same way as were early modern Europeans, so we must turn to nutrition experts and other medical professionals for advice.
The New Vernacular of Scientific Constituents Shows the Power of Modern Science
An example of a nutrition label showing the constituents of a package of pork rinds.
Despite our reliance on the authoritative accounts of modern medicine, we still use this scientific language, as in “I have to watch my cholesterol,” as though there were no expert intermediary to our knowledge of our foods and our bodies. In fact, as Shapin understands it, this scientific language is part of who we are and of how we understand ourselves, though that was not always the case. He explained that the rise of scientific expertise to dominance played a role in reconstituting ourselves. As he put it, “We are what scientists say. We didn’t used to be.” Without criticizing this reality, he went on to articulate that this new vernacular of scientific constituents shows the power of modern science.
He clarified, however, that there are actually two ways to think about this power. One way is to consider the rise of constituent descriptions as a reflection of the medicalization of modern life—our lives as we understand them are more medical than they once were. But, Shapin qualified, it is also possible to see this “power” as an indication that the “reach of modern science is actually less than it once was.”
Under dietetics food and drink composed just one of six aspects of daily life over which medical advice (expert or not) reigned. And, whereas modern medicine is adamantly instrumental, advancing physical but not moral well-being, dietetics advice had moral dimensions. Today, we might look to religion or philosophy to tell us what is morally right; dietetics shows how science (of a sort) once dominated these spheres, too.
Then and Now: What Has Changed?
Shapin concluded his talk by asking how we might begin to think about the big picture, the fate of dietetics and the rise of nutritional science to replace it. How, he asked, can we describe what has changed and where that leaves us in relation to our bodies, our food, and our physicians? Two historical trends can guide an answer to this question.
The first of these, the separation of expertise and lay knowledge, occurred concurrently with the increasing professionalization of medicine. Dietetics asked people to be their own physicians in many respects, requiring them to report on, to sense, and to manage daily routines through illness and health. This system, by contrast to modern medicine, elevated the level to which each person monitored his medical well-being on a daily basis.
Explored during Shapin’s talk as a key distinction between dietetics and nutritional science, the separation of ethical prescription from instrumental description was increasing in other areas of western culture at the same time. As he explained, under dietetics “instrumental advice occupied much the same cultural terrain as moral advice,” and medical and moral assessments used the same sort of vocabulary and reached much the same conclusions as one another.
The division of the ethical from the instrumental in medicine belongs to the same historical move as the emergence of “the naturalistic fallacy” in philosophy around the turn of the 20th century. This fallacy says that, logically, one can’t move from an “is” statement to an “ought” statement—just because something is or has been a certain way, one should not assume it should (morally) be that way.
Balance and Moderation
Examples of dietetics-like advice found on fast food companies’ websites to advertise high calorie foods.
Whereas the principles of balance and moderation once offered the means to an end (health) and an end in and of themselves (moral health), modern science provides means, but not ends. For us, equaling our consumption of healthy foods with that of unhealthy ones just for the sake of upholding balance would be nonsensical, and we would not dream of prescribing cantaloupe to someone simply because he was sluggish. Today we would not find, nor presumably welcome, a conversation with our nutritionist in which the concepts of sin, gluttony, and excess were deployed as medical advice.
But balance and moderation have not disappeared completely from public discourse about food. In fact, in a humorous turn, Shapin revealed that “what was once traditional dietetic counsel has become the property of agents in society with the least credibility” when it comes to food: fast food companies.
These companies use the idea of balancing healthy foods “with a little fun” to advertise the very foods nutrition experts would warn us against. Shapin’s parting remarks left the audience considering the role of dietetics principles in a world so very different from the 17th century world of their prominence: “Prudence, now an aid to profit, once the most authoritative dietary advice, now a cynical attempt to link the bad and the bad for you with the good and the good for you.”
I grew up in Wisconsin and Michigan in a family that has been dairy farming for generations. While studying at Michigan State University, I grew vegetables–sweet corn, tomatoes, squash—that I sold to local grocery stores to support my studies.
I started off there in physics and food science. Then, I went on to medical school but took several electives on nutrition-related topics. I spent one summer on a reservation in the Upper Peninsula of Michigan doing a health and nutrition survey. I was shocked that 50 percent of adults in our survey had type-2 diabetes, and the study demonstrated to me how it was possible to collect very interesting and useful data about people’s diets with a simple structured questionnaire.
My papers on how diet relates to long-term health and disease have led to being the second-most-cited author in clinical medicine. Much of this work was conducted within the Nurses’ Health Study, which has provided a tremendous platform that continues to yield an expanding output of data as the subjects grow older.
The original focus of the study was breast cancer, but that allowed us to get funding to collect dietary data starting in 1980. The Nurses’ Health Study was the first large study to gather dietary data and follow a large number of people for many different outcomes. It’s also unique for having repeatedly updated dietary data every four years over time.
Diet and Cardiovascular Disease
Many of our findings flew in the face of conventional wisdom. I was interested in the 1970’s in the relationship between diet and cardiovascular disease and people were being told very strongly, as though it was absolutely established truth, that we should avoid eggs to prevent heart disease and give up saturated fat.
When I dug into the literature supporting this, it was remarkably weak. In fact, there were no studies that showed that people who ate more eggs had higher risk of heart attacks, and the few small studies showed no relationship. It became apparent to me that a strong body of empirical evidence was needed if we were going to be giving guidance to individuals or the public.
During that time, several epidemiologists were documenting that rates of many cancers around the world varied tremendously. For example, the rates of breast cancer in post-menopausal women in Japan were only about one-eighth of those in the U.S. That obviously provokes the question, why? When I was in medical school, no one really asked why these things were happening, why people get cancer. When I went to the Harvard School of Public Health, people in the Department of Epidemiology were asking those questions.
The Department Chair at the time, Brian MacMahon, said there were some suggestions that diet might be important in the cause or prevention of cancer. That sounded like a pretty radical statement. The evidence was very scattered and not very strong, but the topic seemed worth investigating. What has unfolded has been surprising. Many highly controversial at first, but the finding has been replicated repeatedly and it’s accepted now.
Research Leads to Regulation of Trans Fats
There had been a belief that the percentage of calories from fat in the diet was the main reason why breast cancer rates were higher in the U.S. than in Japan and in developing countries. That idea turned out to be not supported by the data. Trans fats appeared early on as a problem. Experts in the cardiovascular field had been telling people to replace butter with margarine and Crisco to reduce cholesterol and saturated fat. But it turned out that those foods were very high in trans fats and were even worse than the foods they were meant to be replacing.
I was attacked, but most of these findings have become accepted with time. It took about 10 years to get FDA to require that trans fats be included on food labels. Just a few weeks ago, The New England Journal of Medicine published a letter by one of our junior colleagues showing that in prepared foods, restaurant foods, and main national chains the amounts of trans fats have been reduced by about 90 percent. There’s been a huge change in the last three or four years in the national food supply and probably in everybody’s body. If you actually stuck in a needle and analyzed your tissues, you’d find a big difference.
In the field of nutrition, the tools did not exist to answer the most important questions: How does what I eat affect my long-term health and wellbeing? The bridge between epidemiology and nutrition provides a way to these answers.
Four members of The New York Academy of Sciences (the Academy) in the psychology and neural science departments reported their new-found technique in the journal Nature.
Researchers in the New York University Department of Psychology and Center for Neural Science, Daniela Schiller, Elizabeth Phelps, Marie Monfils, and Joseph LeDoux, have developed a noninvasive technique to block the return of fear memories in humans. The technique, reported in the December 9 edition of Nature, may change how memory storage processes are viewed and could lead to new ways to treat anxiety disorders.
The four Academy members and colleagues showed that reactivating fear memories in humans allows them to be updated with non-fearful information, a finding that was previously demonstrated in rodents. As a result, fear responses no longer return.
Finding the Re-consolidation Window
The experiment was conducted over three days: the memory was formed in the first day, rewritten on the second day, and tested for fear on the third day. However, to examine how enduring this effect is, a portion of the participants was tested again about a year later. Even after this period of time, the fear memory did not return in those subjects who had extinction during the re-consolidation window. These results suggest that the old fear memory was changed from its original form and that this change persists over time.
“Our research suggests that during the lifetime of a memory there are windows of opportunity where it becomes susceptible to be permanently changed,” says Schiller. “By understanding the dynamics of memory we might, in the long run, open new avenues of treatment for disorders that involve abnormal emotional memories.”
Phelps added, “Previous attempts to disrupt fear memories have relied on pharmacological interventions. Our results suggest such invasive techniques may not be necessary. Using a more natural intervention that captures the adaptive purpose of re-consolidation allows a safe way to prevent the return of fear.”