Due to developing resistance to certain drugs, tuberculosis has reemerged as problematic for public health professionals.
Published January 1, 2002
By Linda Hotchkiss Mehta
Recent deaths from inhalation of the anthrax bacterium, coming in the wake of September’s terrorist attacks in the United States, have focused widespread public attention on the potential for biochemical terrorism. Potential agents of mass destruction being discussed range from the smallpox virus to the bubonic/pneumonic plague bacterium to a variety of toxic chemical agents.
While concern about the lethal potential of biochemical terrorism is warranted, many public health experts believe insufficient attention is being paid to an equally deadly germ whose spread is already a global pandemic: Mycobacterium tuberculosis. Unlike anthrax, which is not contagious and can be readily treated with antibiotics, tuberculosis (TB) is highly infectious and there is no effective treatment for some multi-drug-resistant (MDRTB) strains.
The TB threat is not new: In the early 19th century TB was so prevalent in England that it accounted for nearly one quarter of all deaths in the country. But 20th-century advances in treatment and public health have engendered a complacency that can tempt us to think we have put such scourges behind us.
Consider this: fully one-third of the world’s population is currently infected with tuberculosis. This amounts to 2 billion persons harboring Mycobacterium tuberculosis. And some MDR-TB strains are no more curable than the bacillus was in 1820.
A Patient Killer
TB remains, after HIV, the leading cause of young-adult death from infectious disease. Nevertheless, we have several advantages over the Victorians, one of which is that the survivors among them passed on some natural immunity to us, their descendants. We also are better housed and fed, and effective treatments now exist against most strains. We can quantify the risk better, and are much better at preventing hospital-based infection. Genetic research has identified TB-susceptibility genes in humans, making it possible to identify the mutations in the bacterium that make it drug resistant.
The 21st century has its own disadvantages, however, including much greater mobility of a large portion of the world’s population. Pharmaceutical companies fund most of the new drug research. Marketplace pressures might influence them not to pursue TB drugs, as most of the need is found in poorer countries. In any case, no new drugs or vaccines to either treat patients or contain the spread of TB are on the horizon in the next five years. The HIV/AIDS epidemic means that a much greater percentage of those persons exposed to TB will develop active cases, which in turn will exacerbate treatment of the HIV infection, causing a higher rate of premature death.
Drug resistance has been a problem since drugs were first used 50 years ago. An estimated 35 percent of people don’t take their medications correctly, whether for TB or any other ailment. This is true across socioeconomic and educational demographic lines, making it hard to predict which patients will be noncompliant.
Combination Therapy
The patient who is being treated with several antibiotics and decides to only take one at a time to cut down on side effects is providing the bacillus with ideal conditions for becoming progressively resistant to a series of medications. Use of combination therapy (two or three antibiotics in one capsule) has been demonstrated in Europe to be an effective way to circumvent this behavior, but this approach is only slowly catching on in the United States.
In March, the Royal Society of Medicine hosted a conference, Tuberculosis Drug Resistance: From Molecules to Macro-Economics, which will be published in Volume 953 of the Annals of the New York Academy of Sciences along with papers from another conference, New Vistas in Therapeutics: From Drug Design to Gene Therapy.
“Multi-drug-resistant tuberculosis has a 50 percent mortality rate and costs at least $10,000 per patient to treat,” according to Peter Davies, one of the principal organizers of the meeting. “It is of more concern than other infectious diseases, except perhaps malaria, because TB itself is so common around the world. Also, TB can “incubate” in the human body for decades, so infection caught now may erupt into active disease any time from six weeks to 90 years.”
The World Health Organization (WHO) has identified the world’s TB “hot spots”— 80 percent of the incident cases are found in just 22 countries. Mario Raviglione, coordinator of TB Strategy and Operations in the Stop TB Department of WHO in Geneva, reported that MDR-TB has been a major problem in the countries of the former Soviet Union. Newly identified areas with a high prevalence of MDR-TB are found in China, Iran and Russia.
The Situation in India
Zarir Udwadia, a consultant chest physician at three of Bombay’s private hospitals, described the situation in India, where half of the world’s TB is found and less than 1 percent of the gross domestic product is spent on health. In India, social factors, poverty, poor prescribing practices and uncontrolled sales of anti-TB drugs have contributed to a crisis in MDR-TB incidence. DOTS (directly observed treatment, short course) programs were introduced in 1992 and show heartening improvements in detection and cure rates, but are not likely to have an impact on existing MDR cases.
“Tuberculosis is a major cause of morbidity and mortality in sub-Saharan Africa, with an incidence rate of 259 per 100,000 population in the region,” said Alwyn Mwinga of the University of Zambia School of Medicine. “An increase in the number of TB cases has occurred in the last 15 years, much of them attributable to co-infection with HIV.”
In spite of these increases, the rates of MDR-TB in Africa are much lower than those in Russia. Overcrowding in Russian prisons, where the number of inmates has increased to seven times the Western European norm, mean that the beds in dormitories are used in three shifts.
Baroness Vivien Stern, of the International Center for Prison Studies at the Law School of Kings College London, reports estimates of MDR-TB in Russia that range between 20 percent and 40 percent. WHO guidelines recommend a 75 percent cure rate for MDRTB to control the disease within a community. Current data indicate that cure rates in Russia are as low as 5 percent.
An Insidious Bacterium
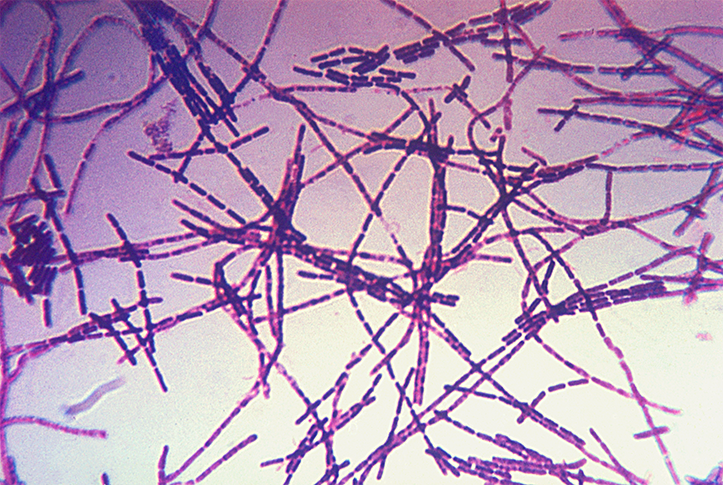
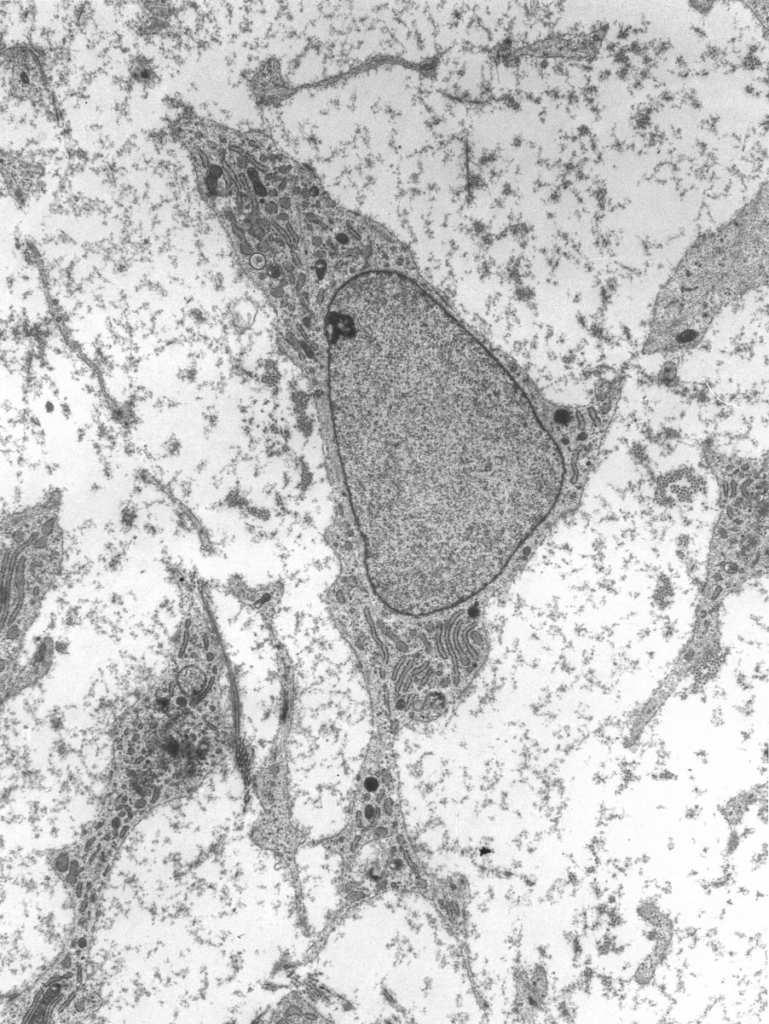
M. tuberculosis, discovered by Robert Koch in 1882, has a heavy lipid coat, which probably enables the bacterium to resist the onslaught of the body’s immune defenses, and a slow reproductive rate (18 to 20 hours, compared to less than one hour for other bacteria). The first effective treatment wasn’t discovered until 1943, when Selman Waksman identified streptomycin. Within 25 years, 11 more medications were available to combat TB, of which only a few were truly “first line,” including isoniazid and rifampin.
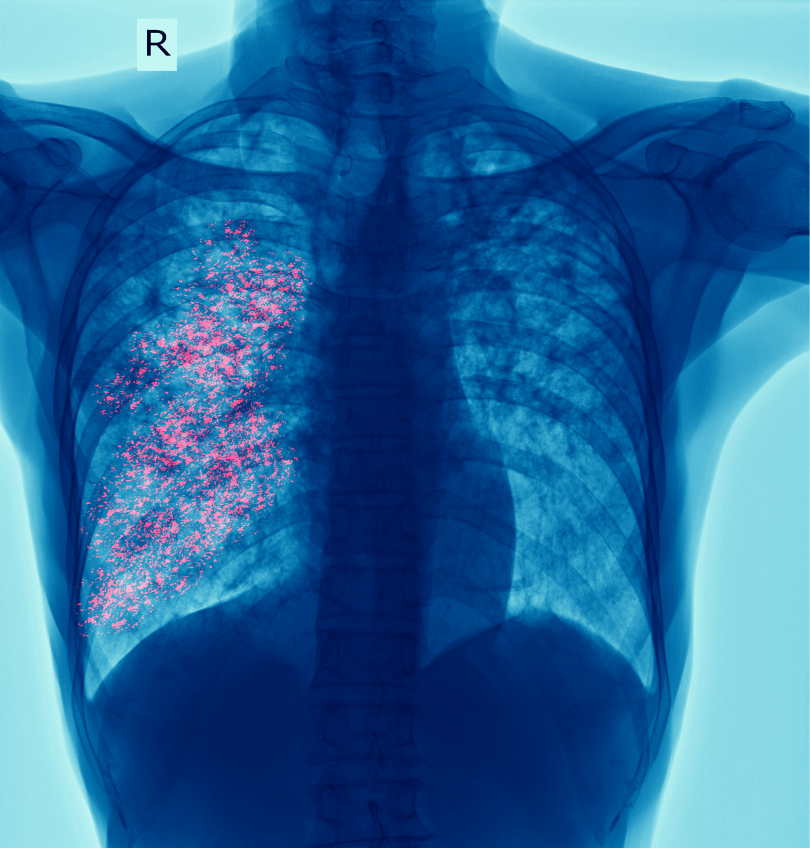
Unfortunately, the bacterium had also made great progress by then, and drug-resistant strains had developed. The tiny size (4 microns) of the bacillus meant that it could gain access to the deepest recesses of the lungs. Once lodged there, macrophages engulf the bacterium and begin to digest it, exposing some of its inner parts to the macrophage’s surface in the process, and then transport the bacillus to the lymph nodes, where T lymphocytes are stimulated to produce lymphokines, which in turn encourage the macrophages to become more aggressive.
As a result of these actions, the mycrobacteria will stop multiplying 95 percent of the time, but they remain in the body indefinitely, awaiting a weakening of the host’s immune system. HIV and AIDS have provided an opportunity for many infections to move from dormancy to an active state, as have cancer and the immunosuppressive drugs used in organ transplantation.
Cell Wall Biosynthesis
Most antibiotics work by affecting cell wall biosynthesis: We now understand these processes at the genetic level through structure–function analysis using recombinant DNA techniques. A drug that acts through inhibition of cell wall biosynthesis must be present long enough to be assured of an opportunity to act when the process it affects is under way. The slow reproductive rate of M. tuberculosis can, therefore, limit the effectiveness of these drugs.
Adrian Hill, professor of Human Genetics at the Wellcome Trust Centre for Human Genetics at the University of Oxford, reported on a two-stage, genome-wide linkage study in families from Gambia and South Africa to search for regions of the genome containing tuberculosis-susceptibility genes. Markers on chromosomes 15q and Xq showed evidence of linkage to tuberculosis, and an X chromosome susceptibility gene may contribute to the large number of males with tuberculosis in many populations.
Paul Farmer, of Harvard University Medical School, stressed the transnational quality of the spread of MDR-TB by describing the discovery of a patient from Massachusetts with pan-resistant TB. Because this patient had been working in Peru, Farmer and his team went to Lima to pursue the source of this strain of the bacillus. They detected the identical strain of TB and ultimately treated 74 patients who had been written off as “incurable.” The team achieved an 85 percent cure rate.
Education Is Essential
Farmer advocates implementation of local solutions that can respond appropriately to specific community circumstances.
Another contributor, Len Doyal, professor of Medical Ethics at the Royal London School of Medicine and Dentistry, explored the morality of one such solution: coercion and detention. He felt these policies could be part of an acceptable strategy, but that counterbalancing programs, including educational efforts to de-stigmatize TB and efforts to undermine the causes of world poverty, must be in place.
In light of evidence that MDR-TB is already a global pandemic, conference participants expressed concern that the global organizations and individual nations lack the will to provide the necessary resources to combat the tuberculosis epidemic in time to forestall a major crisis. Let this meeting be our warning.
Also read: The New Age Threat of Tuberculosis









{kind=link}
{kind=link}