Greater efficiency in the tri-state region’s medical facilities can lead to more affordable costs for patients. The region is currently nearly twice as expensive as neighboring Massachusetts.
Published January 1, 2000
By Frank B. Hicks, PhD, and Susan U. Raymond, PhD
HMOs claim that it’s a matter of efficiency; hospitals say it’s a lack of revenue. But whether because they spend too much or are paid too little, the region’s medical institutions are in trouble. Both as employers of skilled workers and as provider of care for the region, health care and its costs affect all businesses.
Hospitals, which make up about half of health services, are hurting in New York and New Jersey. Total margins in both states—revenues outpace expenditures by 3.0% in New Jersey and by only 2.2% in New York—are lingering at the bottom of the nation. Fears are that these margins will drop even further as a result of the 1997 balanced budget legislation, which has limited Medicare payments to hospitals.
Connecticut, on the other hand, has become a regional bright spot. Between 1994 and 1997, the median hospital margin there more than quadrupled, from 1.0% to 4.2%. Connecticut leads the region and betters the national average in another, broader measure of hospital health, the Financial Flexibility Index. New York and New Jersey have been relatively static in this measure and again lurk near the very bottom of the nation.
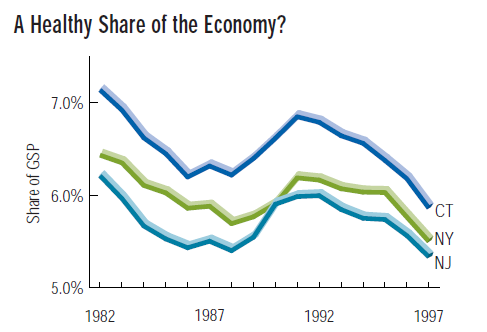
Health Expenditures Rise, but Health Services Shrink
Total national health expenditures have been on the rise: from 8.9% of the Gross Domestic Product in 1980 to 13.5% in 1997. But over the same period, the health services share of the GDP (a subset of national health expenditures) has slipped from 6.7% to 5.2%. The same trend is evident in the Tri-State region. While a slow-growing health services sector may eventually contribute to containing health expenditures, it will also become a smaller driving force for the overall economy, a driving force often credited with helping lessen the impact of the last recession on the Tri-State region.
New York’s Academic Medical Centers: Academic Backbone
TREND: NYC Remains Academic Medical Stronghold
More than half of New York City’s hospital beds are housed in academic medical centers—hospitals whose work extends beyond patient care to include research and instruction for medical students and graduates. With only 2.8% of the total US population, the city trains more than 14% of the nation’s medical residents.
IMPACT: Tendency to More Expensive Care
While academic medical centers offer both patients and students access to cutting edge health care, research and teaching tend to boost their operating expenses as well. These differences traditionally have been shored up largely through Medicare, but this support was trimmed by the federal government’s Balanced Budget Act of 1997.
New York’s Academic Medical Centers: Economic Impact
TREND: Substantial Direct Spending
Direct spending by academic medical centers in New York State totaled $21.3 billion in 1996. Nearly half that spending was supported by out-of-state funding sources, the largest of which were Medicare and Medicaid, which provided $6.6 billion to the state.
IMPACT: Ripples Through the Economy
Academic medical centers paid $2.85 billion in city and state taxes in 1996, and the Greater New York Hospital Association estimates that the academic medical infrastructure accounted for $43.1 billion of total spending within New York State, 6.9% of the 1996 GSP.
New York’s Academic Medical Centers: Managed Care
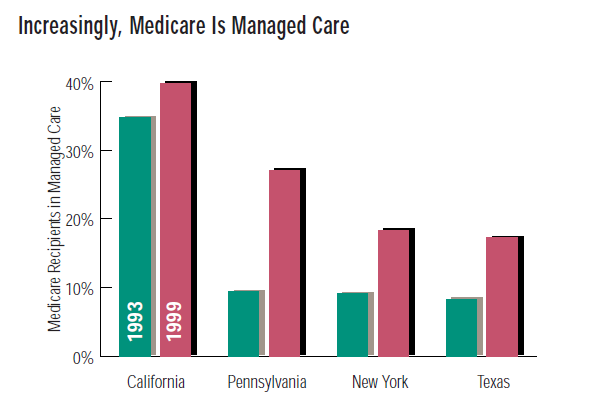
TREND: Managed Care on the Rise
Since 1995, the fraction of New York State Medicare recipients enrolled in managed care plans has more than doubled, to 18.3%, and that fraction will continue to grow.
IMPACT: The Crux of the Crisis
Increasing enrollment in managed care (which tends to take patients away from the higher fees of teaching hospitals) and Medicare cuts from the Balanced Budget Act have hit academic medical centers on two fronts. While academic medical centers claim they are not receiving enough money to provide first rate care and cover indigent patients, managed care providers cite the centers’ high cost of treatment and argue the goal should be higher efficiency.
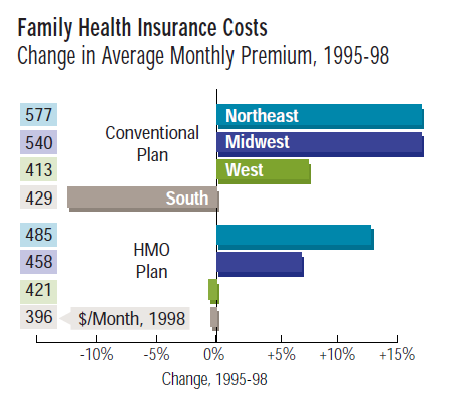
Healthcare Costs from the Consumer Perspective
Health insurance premiums for conventional and HMO plans are higher in the Northeast than in any other region of the country. What’s more, the rates in the Northeast have also shown the greatest growth from 1995 to 1998: rates for HMO family coverage rose nearly 13% over that period, compared to a national rise of only 4%. In the South and West, rates even fell over the same period.
The high northeastern rates are no wonder, since the insurance companies themselves are also hardest hit in the Northeast, particularly in the Tri-State region. A hospital stay for an elderly patient suffering from pneumonia costs nearly twice as much in New York as it does in Massachusetts. These cost differences fuel the claim that there is room for improvement in the efficiency of the Tri-State region’s hospitals.
Also read: The Economics of Health Services Employment
Sources
- William O. Cleverly, The Center for Healthcare Industry Performance Studies, The 1998-99 Almanac of Hospital Financial & Operating Indicators.
- Health Care Financing Administration; U.S. Department of Labor.
- American Hospital Association; Greater New York Hospital Association and Amos Ilan and Associates; Health Care Financing Administration.