There is an urgent need for new drugs and treatments to address a range of illnesses in infants, children, and adolescents, yet including these vulnerable populations in clinical research raises a number of ethical issues that are important to address. This event will explore key ethical considerations regarding the research participation of those who have not attained the legal age for consent to treatments or procedures involved in biomedical studies. Discussions will center on addressing consent, assent, and privacy in pediatric research, study design and regulatory issues, small sample size studies in genomics and rare disease research, health disparities, Covid-19 research in children, broad population-based disease prevention efforts, and will close with a look to the future of pediatric research.
Colloquium Conflict Management
The New York Academy of Sciences is a neutral convener of scientific symposia. We adhere to Accreditation Council for Continuing Medical Education (ACCME) principles for all of our programming. Please note that Johnson & Johnson is a sponsor of this convening, and The New York Academy of Sciences and NYU Grossman School of Medicine exercise full control over the planning of the program’s content, the selection of speakers and all enduring materials.
The symposium will focus on respiratory vaccine research and development, bringing together experts from various fields to discuss challenges and breakthroughs in vaccinology. Notably, it will cover the design of vaccines for respiratory diseases, including those targeting older adults and pregnant mothers and their infants, with updates ranging from preclinical research to surveillance and rollout.
Sponsors
Microbiology and Infectious Disease Discussion Group Lead Supporter
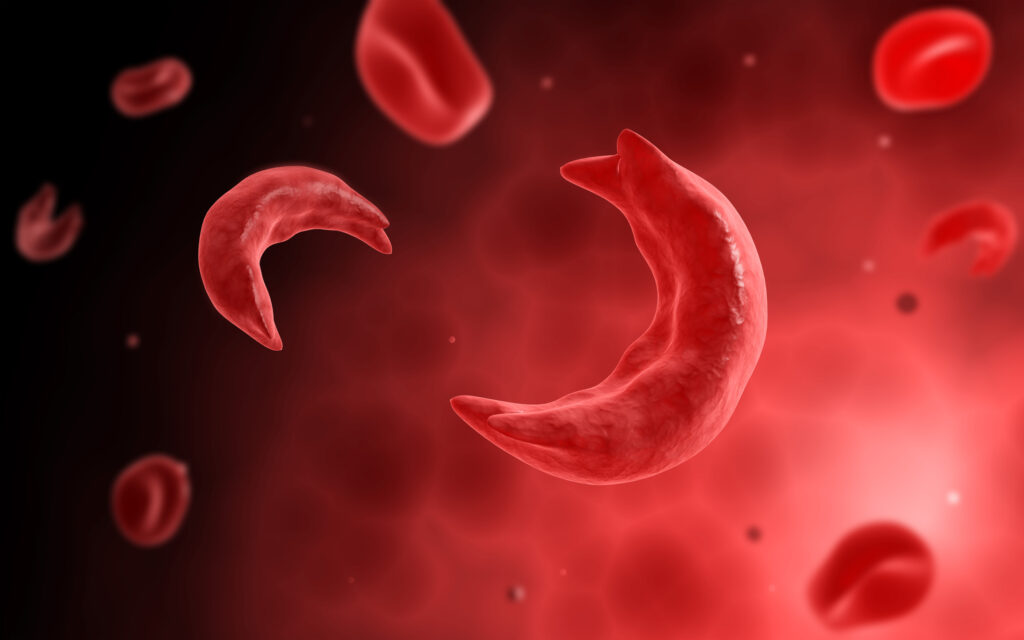
Sickle cell disease (SCD) is a genetic blood disorder affecting approximately 6 million people worldwide, with an estimated 120 million individuals carrying the sickle cell trait.
Advances in scientific research are essential to developing improved treatments and enhancing the quality of life for those living with this condition.
The conference, “Sickle Cell Disease: Existing Paradigms and Novel Approaches,” will feature groundbreaking discussions and research across five pivotal topics:
Disparities, Real-world Challenges, Opportunity in Sickle Cell Disease
Modeling Sickle Cell Disease
Vascular Pathology in Sickle Cell Disease
Autologous Gene Editing and Reprogramming Cures — An Update
This interdisciplinary symposium will unite leading clinicians, researchers, policymakers, and patient advocates from academia, regulatory bodies, and industry to foster information sharing and collaboration.
Sponsors
Presented By
The New York Academy of Sciences Biochemical Pharmacology Discussion Group
Sponsored By
Lead Supporter: Biochemical Pharmacology Discussion Group
We invite our Members to join us at the 205th Annual Meeting of The New York Academy of Sciences. Academy Chair of the Board Jerry Hultin, with President and CEO Nicholas Dirks, will kick off the event with a welcome address and share updates about new Academy initiatives.
Scientists involved in basic, translational, and clinical cancer metabolism research are invited to attend a symposium hosted by the Academy in New York on April 17th. The event will focus on the intersection between cell signaling and metabolism in cancer. Topics include the intricate networks of metabolite-signaling in tumor progression, therapeutic targets, and translating findings into patient treatments. Plenary presentations, panel discussions, and networking opportunities will foster meaningful conversations among attendees and world-class speakers regarding tumor cell exploitation of cellular signaling and metabolic pathways for malignant growth.
A recent Academy event explored near-death experiences and the medical application of psychedelic remedies, combining elements of science and philosophy.
Published June 9, 2023
By David Freeman
What is the nature of consciousness? What happens to it at the brink of death—and beyond? In what ways can the scientific study of near-death experiences and the medicinal use of psychedelic compounds boost our understanding of the human condition and our ability to ease emotional suffering?
These and related questions were the focus of an Academy conference held on June 8, 2023, in New York City. The one-day event included presentations by psychologists, neurologists, biomedical researchers and a religious scholar. Additionally, there was a gripping first-person account of a near-death experience from renowned journalist and author Sebastian Junger.
What are Near-Death Experiences?
Near-death experiences, or NDE’s, are deeply affecting, often mystical episodes. Experts call them periods of “disconnected consciousness.” They affect some people who are close to death or in situations of grave physical or emotional danger. They are commonly marked by feelings of floating outside one’s body and the sensation of moving toward a bright light, as well with as encounters with dead relatives.
NDE’s have been documented across many different cultures and have been known since ancient times. “We’re talking about something that could be hundreds of thousands of years old,” said Brian C. Muraresku. He is the author of the 2020 book “The Immortality Key.” His book examines scientific evidence for the ritual use of psychedelics in classical antiquity. He was also one of the speakers at the conference.
There’s something about that kind of experience—near-death, psychedelic, mystical, whatever it is—that holds the entire human race together.
Brian C. Muraresku, author “The Immortality Key”
NDE’s are now known to be remarkably common. In recent research, 15 percent of intensive care unit patients reported having one. As did up to 23 percent of survivors of cardiac arrest. This is according to neuropsychologist Helena Cassol, Ph.D. Dr. Cassol is the scientific coordinator of Neurological Rehabilitation Center of the University Hospital of Liege in Belgium and also presented at the conference.
“More people have survived cardiac arrest and other situations and could recall those experiences” as a result of improved resuscitation techniques that have become available in recent years, she explained. She added that NDE’s now represent an emerging field of scientific research.
NDE’s can be personally transformative. Some people report a reduced fear of death in the wake of an NDE. Others report enhanced feelings of compassion or purpose. But some are saddled with a pattern of persistent intrusive thoughts or dreams or other negative after-effects. Given these possibilities, “I think it is important for people to be able to talk about these experiences and be heard in a nonjudgmental way,” Dr. Cassol said.
The Evolution of Near-Death Experiences
There may be an evolutionary basis for NDE’s. Daniel Kondziella, M.D., Ph.D., is a neurologist at Copenhagen University Hospital and an associate professor at the University of Copenhagen in Denmark. During his conference presnetation he described research linking the episodes to thanatosis. That’s the well-documented and remarkably consistent phenomenon in which animals—even insects—feign death in order to avoid being killed by predators.
The research suggests that the evolution of language in humans gave us the unique ability to transform this stereotyped behavior into the rich narratives used to describe the mysterious sensations and perceptions commonly seen in near-death experiences, Dr. Kondziella said. Not everyone is convinced by such research.
“Evolutionary explanations are just-so stories,” said Christof Koch, Ph.D. Dr. Koch is chief scientist and president of the Allen Institute for Brain Science, and also presented at the conference. “They may be true. They made be false. It just doesn’t matter. But the fact that we do have experiences—that is the remarkable thing.”
Studies of the neurological underpinnings of NDE’s suggest that the phenomenon arises amid a sort of blending of conscious states: waking, rapid-eye movement (REM) sleep and non-REM sleep.
“The physiological balance between conscious states is disrupted during the conditions of near-death, leading the brainstem arousal system controlling conscious states to blend waking and rapid eye movement consciousness into a hybrid state” known as REM intrusion,” said Kevin R. Nelson, M.D., a University of Kentucky neurologist and another speaker at the conference. “REM intrusion leads to many key features of near-death, including lying still, visual activation, out-of-body, and the experience’s narrative qualities.”
Most individuals who experience near-death are physiologically predisposed to REM intrusion, according to Dr. Nelson.
Psychedelics as Medical Treatment
As some scientists work to gain a better understanding of NDE’s, others are pursuing clinical trials of psychedelic compounds, which have been shown to trigger an altered state of awareness similar to that seen in people experiencing an NDE. A growing body of evidence suggests that these compounds—given under expert supervision and in carefully controlled settings—can ease emotional distress in terminally ill people quite profoundly.
One landmark 2016 study by researchers including Anthony P. Bossis, Ph.D., clinical assistant professor of psychiatry at NYU Grossman School of Medicine and another speaker at the conference, showed that a single treatment with psilocybin—a psychoactive compound found in some mushroom species that humans have consumed for thousands of years—brought rapid reductions in depression, anxiety, and hopelessness in people with terminal cancer.
The benefits of psilocybin treatment were greatest among individuals who reported strong mystical experiences during the sessions, according to Dr. Bossis. “The more robust that mystical experience, the greater the outcome in terms of reduction of depression,” he said. “These aren’t NDE’s,” he added, “but they’re deathlike experiences with a similar phenomenology.”
Recent research shows that psilocybin is just one of many drugs that can induce NDE-like such experiences and suggests that those induced by ketamine, an anesthetic with hallucinogenic effects, show greater similarity to NDE’s than those induced by psilocybin. But “we only studied the phenomenological similarity between subjective experiences” and didn’t assess the extent to which any of the drugs might be effective treatments for depression, said Charlotte Martial, Ph.D., a neuropsychologist at the University of Liege in Belgium and another conference speaker.
Junger’s Brush with Death
Sebastian Junger’s brush with death came three years ago, following the rupture of an aneurysm in his pancreatic artery. As doctors rushed to stanch the bleeding that threatened his survival, he recalled, he encountered an “infinitely dark” pit that threatened to pull him in but also the welcoming “essence” of his beloved, long-dead father. “It wasn’t quite a vision. It was halfway between a vision and a feeling,” he said.
A self-described atheist whose father was a physicist, Junger said the experience nonetheless led him to reconsider his ideas not only about life and death but about the nature of the universe.
“I wish I could say I believe in an afterlife. I don’t. But I definitely have lost the certitude of my rationality,” he said, adding that he now believes it was possible that “some kind of energy or quantum phenomena” interacts with reality in ways we don’t understand.
If some see NDE’s as possible evidence of the supernatural or a phenomenon beyond the scope of scientific knowledge, others are convinced that they are simply the result of physiological processes—such as the oxygen starvation to the brain that can result from cardiac arrest.
There is a “perfectly natural explanation for NDE’s,” said Dr. Kondziella. “No need to postulate any supernatural events.”
But Raymond A. Moody, Jr., M.D., Ph.D., the keynote speaker whose remarks set the stage for the conference, expressed uncertainty over what near-death experiences actually represent.
Science? Or philosophy?
“I really just don’t know,” he said. “I think the questions that we are dealing with—a lot of them are not yet scientific questions,” he added. “They are philosophical questions.”
Dr. Moody is the author of the 1975 book “Life after Life” that sparked interest in near-death experiences. He has been documenting NDE’s for many years and is credited with coining the term near-death experience.
Uncertainty about life’s transcendent questions is inevitable, according to Karen Armstrong, a London-based author of numerous books on religious affairs and the other keynote speaker at the conference.
“Neither religion nor science can really respond. Ultimately, we are all in a ‘Cloud of Unknowing,’” she said in a reference to an anonymous 14th Century text on spirituality and Christian mysticism. “We are all just trying to find some meaning in it all,” she added, “without which we humans fall very easily into despair.”
For Brian C. Muraresku, the strange perceptions and complex emotions seen in near-death and similar visionary experiences are central to the human experience. “There’s something about that kind of experience—near-death, psychedelic, mystical, whatever it is—that holds the entire human race together.”
Ask Helen Hobbs, M.D. and Jonathan Cohen, Ph.D. about the secret of their research success, and it will come down to one core element: their partnership.
Published May 31, 2023
By David Freeman
The pair were recently awarded the 2023 Ross Prize in Molecular Medicine by the Feinstein Institutes for Medical Research and the journal Molecular Medicine for their pioneering and collaborative work in defining the genetic risk factors for dyslipidemias and metabolic liver disease that have led to the rational design of new therapies.
Hobbs trained as a physician and a human geneticist, while Cohen trained as a bench scientist and a physiologist. But they also recognize how the different perspectives they bring to their work contributes to its success.
“Helen’s got a very good feel for the big picture in terms of the scientific direction pathway areas to choose and which observations we should follow up…she is far more selectively curious than I am,” says Cohen of their research styles, “(while) I tend to pay attention to experimental details.”
Their complementary differences can also be seen in their personalities, “Helen is ‘s very exuberant and very extroverted, and I tend to be more introverted and certainly more self-contained,” says Cohen.
Hobbs adds, “Jonathan is very easy to work with… he’s got a very level disposition. We both need each other to balance each other out.”
In addition to their strengths both also cite good mentors as pivotal guides in their careers.
“A lot of people want to look for a lab that’s doing the latest technique or, you know, papers in Science and Nature,” says Cohen, “I think having somebody who’s a good first-rate mentor is a number one priority.”
Where it All Started
Cohen was fortunate to connect to Weiland Gevers, chair of biochemistry at the University of Cape Town in South Africa while he was still in high school. A similar relationship with Scott Grundy, head of the Center of Human Nutrition at the University of Texas Southwestern Medical Center, made it possible for Cohen to relocate to Dallas.
There, he soon would meet Hobbs, who moved to UT Southwestern in 1983. A trained physician, she was encouraged by Donald Selden, M.D., head of internal medicine at UT Southwestern to join Nobel Laureates Michael S. Brown and Joseph L Goldstein’s lab whose work in the regulation of cholesterol metabolism, laid the foundation for Hobbs’ own study of the genes that caused severe hypercholesterolemia.
In 1999 Hobbs was asked to help design an epidemiological study for a large grant that scaled from genes to populations. She knew she needed the right partner if she was going to take on the challenge.
“I was used to working with families, not populations,” recalls Hobbs. “I knew immediately if I was going to do this, … that I really needed a partner who had more quantitative skills than I did.”
She started talking to Cohen, and in just six weeks they launched the foundation for the Dallas Heart Study, a large multi-ethnic population study.
“We spent nights up in our labs writing this study, talking to each other, thinking about it, and getting advice from epidemiologists.”
Looking at Gene Variations
While most researchers in the field at the time were operating under the assumption that gene variations found frequently in the population were the cause of common diseases (like hypertension), Cohen and Hobbs took a different approach – they looked for gene variations that were rare but were more likely to cause disease if a person had that variant.
The multi-ethnic nature of the Dallas Heart Study, made up of 50% African-Americans, the most genetically diverse population in Dallas, and including Hispanic and European participants, led them to quickly zero in on mutations in a gene called PCSK9 that were associated with reduced plasma levels of low-density lipoprotein (LDL) cholesterol and decreased risk of heart disease.
This revolutionary discovery meant that new drug development could be targeted at PCSK9 to lower cholesterol levels in patients, and two therapies have since been FDA-approved to do just that. Despite the opportunities such a discovery could yield, the pair are more focused on how their work solves problems, rather than profiting from their foundational work.
“I am really thinking about solving a problem in a lab and answering a question, and the thrill I get is in getting that answer,” says Hobbs.
Doing What They Love
Ultimately, the two are happy to be in a lab doing what they love.
“I like the whole package of being an academic scientist,” says Hobbs. “I love the research, and I like the teaching, the mentoring. There’s just so many aspects of our job that I enjoy, and I just didn’t want to be distracted from them.”
Cohen can’t picture himself as anything other than a scientist, “I can’t imagine…doing anything other than what I do.”
Today, The Hobbs-Cohen Lab continues to use human genetics to identify new therapeutic targets to treat cardiovascular and metabolic disorders and to define key pathways in lipid metabolism. More recently, they discovered the first genetic cause of fatty liver disease in humans. They also continue to employ their dynamic partnership in the way they run their lab.
“There’s always somebody in the lab for the students and post-doctoral fellows to talk with. I think that if you were to talk to the people in our lab, they would see this as a very good thing,” says Hobbs. “But one thing’s always true. Nobody can split us.”
“To have our work recognized by such an honor (as the Ross Prize) is incredibly gratifying, especially for us to be honored together…there’s just no way any of it could have been done without the other,” said Hobbs.
Cohen agrees. “I was just going to say the same thing.”
In the healthcare field, artificial intelligence has the potential to improve everything from workflow efficiency to patient outcomes.
Published May 25, 2023
By Stephen Treffinger
Image Credit: Agne Sopyte Members of the Organizing Committee. (From left to right) Affiliated with the Mount Sinai Health System: Christina Virgo, Esq., Sara Roncero-Menendez, Silke Muehlstedt, PhD, Thomas Fuchs, Dr. sc., Marc Kaplan; Affiliated with The New York Academy of Sciences: Melanie Brickman Borchard, PhD, MSc, Barbara Knappmeyer, PhD
Appearing on the front page of news outlets nearly every day, artificial intelligence (AI) is already transforming the world. And it’s doing so at a staggering pace. In the healthcare field, it has the potential to improve everything from workflow efficiency to patient outcomes. But sifting through the hype can be a tremendous challenge.
The Windreich Department of Artificial Intelligence and Human Health at the Icahn School of Medicine at Mount Sinai and the New York Academy of Sciences hosted the ‘New Wave of AI in Healthcare’ symposium as a “call to action.” This brought together experts and leaders across the field to tackle this challenge through innovation, exchange, and collaboration.
The symposium took place over the course of two days: May 23 and 24, 2023. Researchers, academics, and industry leaders presented and discussed innovative research. They also focused on clinical solutions with the potential to advance the capabilities of AI. The goal is to better serve patients and clinicians from diagnostics to long-term care.
Opening remarks were delivered by, Nicholas Dirks, President and CEO of The New York Academy of Sciences, and Dr. Dennis Charney, Dean of the Icahn School of Medicine and President for Academic Affairs for the Mount Sinai Health System. They challenged attendees to identify ways to utilize the enormous amounts of health data available. If utilized properly, this can help predict, prevent, and develop more robust treatments for disease.
Advancing the Capabilities of AI
The two-day symposium featured sessions on foundational models that revolutionize diagnostics processes, infrastructural challenges to facilitate large-scale models and innovative deep learning solutions to deal with the petabytes of data generated in healthcare. Also, the symposium addressed ethical considerations for AI research in healthcare to eliminate bias and ensure its application is equitable as well as impactful.
“Today, patients are dying not because of AI, but because of the lack of it,” stated Thomas J. Fuchs, Dr. Sc, Dean for AI and Human Health at Mount Sinai, lead member of the scientific organizing committee in opening the symposium, Dr. Fuchs further emphasized that although machine learning has already led to significant achievements across the field of healthcare, we are only at the beginning of an AI revolution in healthcare.
Image Credit: Monika Graff (From left to right) Panelists: Eric Lium, PhD, Mount Sinai Health System, Brandon D. Gallas, PhD, U.S. Food and Drug Administration, Emma Benn, DrPH, Mount Sinai Health System, Moderator: Eric Nestler, MD, PhD, Icahn School of Medicine at Mount Sinai
AI Fundamentals – Facts, Fictions, and Possibilities
Despite the immense hype around AI (as Dr. Fuchs remarked, “If you haven’t talked about ChatGPT, you’re probably living under a rock.”) and excitement in the start-up scene (including 14,000 healthcare startups in the AI realm), the reality is not quite as dramatic. There are only a few AI applications that practitioners currently use in the clinical setting to benefit patients. “While the FDA cleared hundreds of systems in radiology, in pathology, for example, there’s one single system that has proven to be safe and effective.”
Dr. Fuchs stated that AI gives us the possibility to truly democratize access to healthcare for the first time in history. “The AI we’re developing here and you’re developing at your fabulous institutions can be used in community clinics throughout the U.S. and throughout the world.”
A Deep Crisis in Healthcare
The fact that clinicians are burned out and leaving practices has, according to several of the speakers, resulted in a deep crisis in healthcare. But AI is able to help combat this trend by automating workflows. One of the keynote speakers at the symposium was David C. Rhew, MD, Global Chief Medical Officer and VP of Healthcare at Microsoft. He presented developments in Ambient Clinical Intelligence. This system can, among other things, capture clinician-patient conversations and bring the information into the medical record.
“We have an ability now to pull data about individuals from every aspect. We can look at the perspective of what EHR [Electronic Health Record] data we have, what genomics data we have, and real-time data collection through remote monitoring.” This creates a 360-degree view of a person and one that changes as they evolve. “Now imagine having that at a population level,” he says. “That’s where the real power comes.”
Image Credit: Monika Graff (From left to right) Dennis S. Charney, MD, Anne and Joel Ehrenkranz Dean of the Icahn School of Medicine at Mount Sinai, President for Academic Affairs, Mount Sinai Health System Nicholas B. Dirks, PhD, President and Chief Executive Officer, The New York Academy of Sciences Thomas J. Fuchs, Dr.sc., Co-Director of the Hasso Plattner Institute for Digital Health at Mount Sinai, Dean of Artificial Intelligence and Human Health, and Professor of Computational Pathology and Computer Science at the Icahn School of Medicine at Mount Sinai
AI for Healthcare and Life Sciences – Accelerated Discovery
Will more data and data-driven models yield better patient outcomes? This was a central theme throughout the symposium. Speakers utilizing foundational models in research and clinical diagnostic support tools to create deep learning models. Researchers develop these across heterogenous data modalities to improve patient outcomes.
The conference’s second keynote was delivered by Jianying Hu, PhD, from IBM Research. Dr. Hu is also an adjunct professor at the Icahn School of Medicine at Mount Sinai. In addition to IBM’s use of AI to drive accelerated discovery, she discussed what it means to go beyond large language models to apply foundational models to healthcare and life sciences research.
“In our view, [it’s] really all about enabling the journey from data to impact. AI can be used to help with the development of new molecular entities through novel generative methods, as well as computational screening tools [that] can be used to also identify new indications for drugs that are already approved,” says Dr. Hu. In addition to drug repurposing, AI is critical, she says, for being able to identify multimodal biomarkers.
From the Laboratory to Practice: Clinical Applications of AI
Moving from the theoretical to the practical and harnessing the full power of AI will require a change in approach, especially as it pertains to data: how much of it is required, how it needs to be treated, and how to maximize its effects. Abundant medical data is playing an important role, as precision medicine tries to determine the right treatment for the right patient at the right time.
“When we think about precision medicine and AI in medicine, we think about the health state of a patient and how we can model that health state of a patient,” says Gunnar Rätsch, PhD, ETH Zürich, who is currently conducting research as a visiting scientist within Mount Sinai’s AI Department.
Evidence of the health state comes from heterogeneous data modalities such as EHRs, pathology images, genomic profiles, drugs, and mobile health data. Integrating this data into computational representation enables practitioners to access a patient’s health state. This requires new advances in AI approaches to exploit the specifics in the medical data, which requires genuine partnership between clinicians and machine learning/AI researchers.
Image Credit: Yovanna A. Roa, LMSW Christina Virgo, Esq., Director of Operations Hasso Plattner Institute for Digital Health at Mount Sinai
The Impact of the New Era of Large-scale Deep Learning Models
Increasing the speed by which researchers can process and analyze vast amounts of data is an ongoing challenge in AI. The exponential growth of healthcare data, genomics, electronic records, and imaging can overload systems and slow the path to progress.
But processing capacity and speed aren’t the only issues. Another challenge is to better merge clinical medicine and data science, the two being mutually beneficial. Anthony Chang, MD, from the Children’s Hospital of Orange County, thinks this is an essential—albeit largely absent—duality. Few people understand both sides of the equation.
Dr. Chang also sees the need for a shift to a new paradigm of databases, i.e. graph databases. “These are more three-dimensional and much more accommodating of the complexities of healthcare data. […] I can’t imagine we’re going to get a lot more dividends using deep learning healthcare without a change in how we look at databases, which is relational databases.”
In the detection of breast cancer, to cite one example, having very large scan sizes is advantageous, but dealing with these enormous images efficiently can be problematic due to the amount of memory in the GPU and other factors. Krysztof J. Geras, PhD, NYU Langone Health, discussed the particulars of multiple instance learning. “We have this ability to indicate those parts of the image that are important. We can actually look at this image with greater detail with a higher capacity network, but just at a certain region of it, and then we can fuse this information. And that works amazingly well.”
AI at Mount Sinai
The Mount Sinai Health System is dedicated to leading an AI-driven transformation of healthcare. This is done through innovative research, pioneering clinical care, and personalization for each patient. The aim is to have a wide-reaching impact on human health. In 2021, Mount Sinai established the Windreich Department of Artificial Intelligence and Human Health. This is the first department focused on AI and Human Health in any medical school in the United States.
As a leader in the AI in healthcare space, researchers at Mount Sinai are building an “intelligent fabric” of AI that will underpin all interdisciplinary efforts. They are combining AI, computer science, machine learning, and data science across the Health System to support every individual who comes through the hospital doors for care. It will also support nurses, physicians, scientists, hospital operations and leadership,
Several Mount Sinai researchers presented their AI-integrated research during the symposium. They highlighted the various ways in which this new technology can benefit researchers, clinicians, and patients. This ranges from diagnosis to treatment, as they are developing some of the most exciting advances in the field.
Highlights include:
Ipek Ensari, PhD, who works with AI and machine learning combined with statistics in the field of women’s health, noted the possible link between indicators in the female reproductive system to diseases such as coronary artery disease, and stroke.
Hayit Greenspan, PhD, focuses on AI in the medical imaging space. “We are developing a platform that provides tools for collection of the data, support of annotation of the data, and support of modeling that can be done to extract information that is useful from the imagery data.”
Xiaosi Gu, PhD, focuses on the fast-growing sub-sector of mental health in health tech. “We need to both achieve a mechanistic understanding of the brain and of the mind at the algorithmic level and to use brain-related data to try to create predictive models.”
John F. Crary, MD-PhD, is a neuropathologist and runs a research lab in neurodegenerative diseases. “Alzheimer’s is a monumental public health crisis. It’s really important […] to get […] tissues digitized, organized, and made available to scientists and computational people.”
Bruce J. Darrow, MD-PhD, who leads Mount Sinai’s AI ethics committee, often works on creating spaces and treatments that are not only safe and effective, but also equitable, being tested across the right demographics and taking into account factors such as insurance coverage, income, and zip code.
Robert Freeman, RN, MSN, NE-BC, is working on moving from the reactive to the predictive and preventative AI. In practice, this would lead to shorter patient time in the hospital and improved overall 30-day mortality.
Image Credit: Monika Graff (From left to right) Thomas J. Fuchs, Dr.sc., Mount Sinai Health System, Keynote Speakers: Jianying Hu, PhD, IBM Fellow, Director, HCLS Research, Global Science Leader, AI for Healthcare at IBM Research, David Rhew, MD, Global Chief Medical Officer, Vice-President of Healthcare, Microsoft
Governance and Ethics for the Use of Large Healthcare Datasets for AI
The use of massive amounts of patient data for AI naturally raises key governance and ethics issues. This includes data privacy, transparency, regulatory compliance, and bias screening to ensure fair representation. These issues and more were covered in a panel discussion moderated by Dean Eric Nestler, MD, PhD, Icahn School of Medicine at Mount Sinai.
The role of bias in large healthcare data models can take many forms. This is especially thru when it comes to populations of color and members of underrepresented communities. One of the panelists, Emma Benn, DrPH, is a biostatistician at Mount Sinai, applies her training to health equity research. She addressed the governance and ethics of the topic. In terms of race, she posed the question of whether the algorithms and technology are just describing racial and ethnic differences versus being able to operationalize race in a way that gets closer to identifying mutable targets for intervention.
“If we’re not operationalizing things correctly, we’re not going to be able to use AI to reduce health inequalities,” says Benn.
The Importance of Data Privacy
Another panelist, Dr. Erik Lium, PhD, discussed the importance of data privacy. Dr. Lium is the Chief Commercial Innovation Officer for the Mount Sinai Health System and the President of Mount Sinai Innovation Partners. One question posed by the audience was which processes a hospital uses to protect a patient’s personal health data. The answer depends on who is going to use said data, be it internally for research or with an external partner. Internally, an institutional review board decides acceptable usage. For use with external partners, it involves legal agreements with copious protections. These protections bar anyone from taking, for instance, de-identified data and attempting to re-identify the data.
“You can use the data for a stated purpose that we think is ultimately beneficial to patients. If you go outside of that purpose, then you’re doing something that’s inappropriate,” says Dr. Lium.
Keynote speaker Dr. David Rhew ended his address on a key philosophical and ethics-focused note. He brought up the idea of AI taking a pause to prevent potentially harmful aspects like the spreading of misinformation. “If the good actors pause on this, that doesn’t mean that the bad actors are going to pause.”
In Conclusion
Throughout the symposium, speakers were able to address successes, challenges, and future initiatives. This is needed to further the development of new AI technology in the field and how it can be implemented to better patient outcomes. Some of the key takeaways from the symposium’s sessions include:
Increasing cooperation between institutions.
Figuring out how to obtain and efficiently process ever larger data sets.
Using AI to enhance patient experience and outcomes.
Finally, these developments will need to be carefully and continuously filtered through the lenses of equitability and security to ensure that every patient receives the highest level of care no matter the setting. The ‘New Wave of AI in Healthcare’ symposium was an important step towards this equitable, AI-integrated future, with more advancements and discussions to come.
Can we stop the pain? It may be the oldest question in medicine, and it remains one of the most important. But with chronic pain afflicting billions of people worldwide, and few effective treatments besides highly addictive opioids, researchers are still searching for better answers.
On May 3-4, the New York Academy of Sciences, in collaboration with Science Translational Medicine, convened the Advances in Pain conference. Across the meeting’s two keynote presentations, nine sessions of talks, and concluding panel discussion, leading experts in many branches of pain research discussed the field’s biggest challenges and latest developments.
Highlights
Specific ion channels on neurons, such as Nav1.7, are critical components of pain sensing and potential drug targets for new analgesics.
Several novel laboratory models are revealing new details of nociception, or pain sensing.
Large databases of genetic and clinical records are helping researchers link specific genes with common pain conditions.
Neuroimaging and sleep studies may offer objective ways to measure the severity of chronic pain.
New mechanistic data are pointing researchers toward novel strategies for analgesic drug development.
A subset of gut epithelial cells is critical for sensing visceral pain.
The immune system links tightly to pain sensation, through multiple mechanisms scientists are now beginning to uncover.
Data mining reveals subsets of neurons with distinct responses to nerve injury, including chronic pain.
Understanding sex and ethnic differences in pain perception requires new strategies in experimental design and data analysis.
Besides neurons, Schwann cells can also carry pain signals.
Novel drug discovery platforms and trial designs can accelerate the development of new analgesics.
Part 1
Speakers
David Bennett, MB, PhD Oxford University, Nuffield Department of Clinical Neurosciences
Sarah E. Ross, PhD University of Pittsburgh
Jing Wang, MD, PhD NYU Langone Health
Tuning into the pain channel
A life free of pain may sound ideal, but as David Bennett explained in the meeting’s opening keynote presentation, individuals with defects in pain sensing often suffer tremendous difficulties. Describing one 26-year-old man with such a condition, Bennett explained that “he had pretty much fractured every long bone in his body, he is stunted because he’s destroyed all the growth plates … and had severe burns and mouth injuries.” The patient’s sister, who had the same condition, died of undiagnosed sepsis.
Genetic analysis revealed that the patient had a rare set of loss-of-function mutations in the gene for Nav1.7, a sodium ion channel expressed in nociceptors, or pain sensing neurons. Using a sophisticated cell culture system that mimics pain signaling through nociceptors, Bennett and his colleagues have characterized Nav1.7 in detail, and determined that it acts early in the pain signaling process, amplifying the electrical signal in the nociceptors to ensure that it’s relayed to the central nervous system.
Patients with gain-of-function mutations that make Nav1.7 overactive have the opposite problem: incurable chronic pain. Bennett’s team studied the Nav1.7 mutations in these patients, and discovered that the degree of the biochemical defect in a patient’s channel proteins correlates directly with the time of onset of their pain condition.
Based on his findings in patients with these rare, extreme pain disorders, Bennett hypothesized that Nav1.7 could also drive more common conditions. As rates of diabetes skyrocket globally, millions of people are developing diabetic neuropathy, which causes chronic pain only in a subset of patients. In an effort to determine what distinguishes painful from pain-free diabetic neuropathy, Bennett’s team looked at Nav1.7 gene sequences for patients with the condition.
“The rare variants in Nav1.7 seemed to cluster much more in the painful versus the painless diabetic neuropathy groups, so this is now acting as a risk factor, in the sense that these people did not experience [chronic] pain prior to developing diabetes,” Bennett says.
Some variants of Nav1.7 apparently predispose people to develop chronic pain, but the condition doesn’t manifest itself until a second event, such as diabetes, triggers it. A closer look at clinical testing results in these patients revealed that those with the rare variants were also more sensitive to certain stimuli, such as burning pain and pressure pain.
Nav1.7 isn’t the only ion channel involved in pain, though. The researchers have also identified strong associations between pain disorders and mutations in the related channel proteins Nav1.8 and Nav1.9, highlighting the diversity of channelopathies that can derail pain sensing. Indeed, an analysis of data from the UK Biobank, which has whole genome sequences and medical records for 100,000 Britons, revealed that voltage-gated sodium channels were the largest group of variants associated with neuropathic pain.
Based on his findings, Bennett advocates using both clinical testing data and gene sequencing to stratify patients according to which treatments are most likely to work for them. In particular, sodium channel blocking drugs appear to work much better in patients with variant channels predisposing them to pain.
Where does it hurt?
The meeting’s first regular session focused on efforts to dissect the central pain circuits in the nervous system. For Sarah Ross, the dissection is literal: she carefully removes a piece of a mouse spinal cord, along with the sensory nerves connected to a patch of skin from the animal’s hind paw, keeping all of the neuronal connections intact. Using luminescent probes, her team can then watch the activation of specific neurons in response to stimuli.
“We can see some neurons respond to heat, other neurons will respond to cool, other neurons will respond to mechanical stimuli,” said Ross.
Many neurons also respond to multiple stimuli, and mapping these responses reveals that distinct classes of neurons function as amplifiers, tuners, and integrators of pain signals.
Jing Wang studies what happens to pain signals in the cerebral cortex of the brain. Using optogenetics, which allows him to stimulate specific neurons in the brains of mice with light, he has identified subsets of neurons in the anterior cingulate cortex and prefrontal cortex that respond to pain.
In mice with experimentally induced chronic pain, low-intensity stimulation of the prefrontal cortex restores normal pain control. Wang’s lab is now studying ways to achieve similar responses with less invasive methods, including the drug ketamine and brain-machine interfaces.
“The cortex processes and regulates pain, but its normal endogenous function can be impaired by chronic pain, and [restoring cortical regulation] has the potential to transform pain treatment,” said Wang.
Part 2
Speakers
Aarno Palotie, MD, PhD Institute for Molecular Medicine, Finland
Luda Diatchenko, MD, PhD McGill University
Irene Tracey, MA (Oxon), DPhil, FRCA, FMedSci University of Oxford
Alban Latremoliere, MSc, PhD Johns Hopkins University
The pains of the father
Aarno Palotie began the meeting’s session on the genetics of pain by discussing his results from large-scale studies on migraine. With the exception of some rare, strictly inherited forms of the condition, these sporadic, debilitating headaches usually stem from variations in numerous common genes. To identify those genes, Palotie and a large team of collaborators scrutinized genetic and medical data from hundreds of thousands of migraine sufferers.
The effort revealed over 100 gene loci linked to migraine, mostly in regulatory regions associated with genes expressed in cardiovascular tissue and the central nervous system. Tracking those variants in another large data set revealed a cumulative effect.
“We can see that those with a high polygenic risk score, meaning a high load of common variants, they seem to have an earlier onset of migraine,” said Palotie.
Using data from the 500,000 participants in the UK Biobank, Luda Diatchenko and her colleagues have performed a similar analysis to identify genetic variants linked to chronic pain. The investigators subdivided chronic pain patients based on the type of pain they experienced, such as back pain, hip pain, knee pain, and multi-site pain.
Analyzing gene sequences for these sub-groups showed that multi-site pain had the highest correlation with specific gene variants. The gene most strongly linked to multi-site pain encodes a receptor protein involved in guiding nerve axons in development.
“This is one example of how [genome-wide association studies] can show us a new mechanism which contributes to human chronic pain conditions,” said Diatchenko.
On a scale of one to ten
The meeting’s third session focused on one of the biggest challenges in studying pain: measuring it. Clinical studies attempt to quantify pain severity with patient questionnaires, while animal experiments rely on behavioral responses, but both methods are notoriously unreliable.
Ilene Tracey hopes to solve that problem with neuroimaging, linking specific patterns of neuronal activation to painful stimuli.
“We’ve got now quite a good array of tools that are reasonably well developed and robust, that allow you to look at … ways that patients will experience their pain,” said Tracey.
By combining functional magnetic resonance imaging with electroencephalography, video analysis, and other sensing methods, this approach could allow researchers to quantify patient responses to pain treatment more reliably than current, fundamentally qualitative methods. Using machine learning, Tracey’s team can now measure pain and also distinguish different categories of it, such as physical versus emotional pain.
Sleep disturbances might also provide a pain gauge.
“The vast majority of patients with chronic pain suffer from poor sleep quality,” said Alban Latremoliere, who has been studying this connection as a potential pain biomarker.
By tracking electroencephalography and other measurements in sleeping mice, he and his colleagues have found that nerve injury, which causes chronic neuropathic pain, also changes the animals’ sleep architecture. Compared to uninjured animals, those with injured nerves suffer multiple brief interruptions in the non-REM phase of their sleep. When the injury heals, the normal sleep architecture returns; Latremoliere now hopes to use these patterns to quantify neuropathic pain severity and treatment efficacy in humans.
Part 3
Speakers
Greg Scherrer, PhD University of North Carolina
Venetia Zachariou, PhD, MBBS, MMed, MS Icahn School of Medicine at Mount Sinai
Rajesh Khanna, PhD New York University
David J. Julius, PhD University of California, San Francisco (UCSF)
The hurt blocker
As Greg Scherrer pointed out in the meeting’s fourth session, the real problem with pain isn’t that it exists, but that it’s unpleasant.
“If we were to understand how our brain collects this information from sensory neurons and the spinal cord to make pain unpleasant … maybe we’ll discover new ways to treat pain,” said Scherrer.
Indeed, a patient whose basolateral amygdala was removed to treat epilepsy could still sense painful stimuli, but didn’t label them as painful; the unpleasantness was gone. Examining mice with various alterations to the same brain region, Scherrer and his colleagues believe they have identified the amygdala cells responsible for connecting pain to unpleasantness. The investigators are now trying to identify receptors on those cells that would be good drug targets for new pain treatments.
Venetia Zachariou is also dissecting cellular signaling pathways to target in pain treatment, and her lab has uncovered several promising leads in recent years. When the COVID-19 pandemic derailed that work, though, the scientists quickly pivoted to apply their skills and techniques to study the new disease’s neuronal pathogenesis.
In a hamster model, they found that SARS-CoV-2, the virus that causes COVID-19, can acutely infect nerves in the dorsal root ganglia, which are also involved in pain sensing. Looking more closely at both the hamster model and a mouse model of SARS-CoV-2 infection, Zachariou has identified distinct changes in neurons’ gene expression patterns after virus infection, including a signature similar to that seen in models of neuropathic pain.
One of the most popular targets for researchers trying to develop new pain therapies is the sodium channel Nav1.7, a “pain amplifier” that several speakers at the meeting discussed. Rajesh Khanna is also interested in Nav1.7, but instead of targeting the protein directly, his team is trying to identify proteins that interact with it. That work led them to focus on collapsin response mediator protein 2 (Crmp2), which regulates Nav1.7 signaling.
Mice lacking Crmp2 are resistant to chronic pain, suggesting that drugs inhibiting its action would be good pain therapy candidates. After conducting extensive mechanistic studies, Khanna started a company to identify such inhibitors. So far, the company has optimized a lead compound that appears to stop chronic pain in animal models, without causing detectable side effects or tolerance.
You feel it in your gut
The meeting’s first day concluded with a keynote presentation by David Julius, who discussed his work on chronic visceral pain. This subtype of chronic pain, which can be caused by gut infection or non-infectious conditions such as inflammatory bowel disease, affects about 15% of the population. It’s three times more common in women than men, but nobody knows why.
“We’re interested in a particular aspect of visceral pain signaling, and that involves the interaction of sensory nerve fibers with the gut epithelium,” said Julius.
A subset of gut epithelial cells, called enterochromaffin cells, plays an outsize role in that interaction. Comprising only a fraction of a percentage of all gut epithelial cells, enterochromaffin cells make about 90% of the body’s serotonin, a potent neurotransmitter protein. They also fire electrical signals that could propagate to nearby neurons.
Julius wanted to analyze that process in live mice, but wasn’t happy with the standard mouse system for those types of experiments. That model involves putting irritants into a mouse’s gut to trigger a major inflammatory response, after which the animal remains hypersensitive to physical stimuli such as colon distention.
“Do we need to … put the mouse through all that, or can you have a model that’s simpler [and] does not require all the sequellae of an inflammatory episode?” asked Julius.
Instead, he and his colleagues first tried studying enterochromaffin cells in the context of cultured enteroids, pieces of intestinal epithelium that can mimic many aspects of gut biology in a petri dish. That system revealed that enterochromaffin cells respond to numerous compounds that fall into three general classes: ingested irritants, metabolites of common gut microbes, and endogenous regulatory hormones.
“So, we want to know how these cells integrate all this information, and what role this plays in maladaptive situations like [inflammatory bowel disease],” said Julius.
Based on those results, the researchers moved to a more complex system, an explanted piece of a mouse colon with its connecting nerves. Monitoring the electrical signals in the connected nerves reveals sensory signals from the explanted gut. In this setup, bathing the colon section with isovalerate, a bacterial metabolite that triggered a response from enterochromaffin cells in the enteroid experiment, makes it hypersensitive to subsequent physical or biochemical stimuli. This system also revealed different response patterns in guts from male and female mice.
Having demonstrated that isovalerate could induce gut hypersensitivity without the inflammatory response of harsher irritants, Julius’s team next tried looking at its effect in live mice. They used a small balloon in the colon, similar to an endoscope, as a stimulus, and monitored abdominal muscle contraction, a behavioral response to pain. Treating the mice with isovalerate increased the magnitude of subsequent pain responses potently in male mice, but less so in females, consistent with the explant results.
Subsequent experiments showed that enterochromaffin cells mediate these responses in live mice, apparently through both serotonin secretion and direct electrical signaling to neurons, and that these cells seem to respond differently in male and female mice.
Part 4
Speakers
Isaac Chiu, PhD Harvard Medical School
Camila Svensson, MS, PhD Karolinska Institutet
Alexander J. Davies, PhD Nuffield Department of Clinical Neurosciences
Dana Orange, MD Rockefeller University
Shrinivasan Raghuraman, PhD University of Utah
Jeffrey S. Mogil, PhD McGill University
Frank Porreca, PhD University of Arizona
Roger Fillingim, PhD University of Florida
Is antibody hurt?
Infections commonly cause pain, which researchers had long assumed was just a byproduct of the body’s inflammatory response. However, as Isaac Chiu explained in the meeting’s session on neuroimmune and autoimmune mechanisms in pain, infecting pathogens can also interact directly with nociceptors, or pain-sensing neurons. In one set of mouse experiments, for example, Chiu’s team found that nociceptors in the intestine can detect infection with Salmonella enterica, triggering a response that decreases the number of M cells, the specialized intestinal epithelial cells S. enterica preferentially infects.
“These neurons actually regulate cell numbers, [which] not only shuts down the number of gates for pathogen entry, it also helps a protective microbe … attach better on the surface of the epithelium,” said Chiu.
Camila Svensson discussed a pain condition that has baffled researchers and clinicians for decades: fibromyalgia. Characterized by pain hypersensitivity in soft tissues, sometimes coupled with neuropathic pain, the condition has long eluded efforts to uncover its etiology and underlying mechanisms.
After serendipitously discovering evidence for autoantibodies in fibromyalgia patients, Svensson has now developed human tissue and mouse models to characterize these antibodies in more detail. Transferring antibodies from fibromyalgia patients into mice causes pain hypersensitivity in the animals, and patients with higher levels of antibodies that react with human dorsal root ganglia cells have more severe disease.
“This suggests that there is an autoimmunity in subpopulations of fibromyalgia patients,” said Svensson, adding that besides suggesting a mechanism for the disease, autoantibody levels could help stratify patients in clinical trials.
The body’s own immune response is also a key contributor to chronic neuropathic pain, especially through neuroinflammation. Alexander Davies presented his work on another component of neuropathic pain: the cytotoxic cellular response.
Cytotoxic cells normally detect cancerous or virally-infected cells and target them for destruction, but they can also target injured neurons. Dissecting this response in an extensive series of experiments in mice, Davies and his colleagues have found that a specific receptor on cytotoxic cells allows them to target nociceptors after nerve injury, leading to degeneration of the damaged axons and resolution of pain hypersensitivity.
“So, our data suggest that intact sensory networks are a source of ongoing neuropathic hypersensitivity, and that by targeting those, we can help to resolve that,” said Davies.
Short, sharp shocks
Dana Orange gave the first of two short “data blitz” presentations, providing an overview of her group’s work on rheumatoid arthritis pain. Though inflammation of joints is a hallmark of this form of arthritis, Orange noticed an odd discrepancy.
“Patients who really don’t have a lot of inflammation were reporting a lot of pain,” she said.
Through a combination of human gene expression and mouse studies, she’s found that nerve development may play a bigger role than inflammation in driving rheumatoid arthritis pain.
Shrinivasan Raghuraman described his approach to characterizing chronic pain mechanisms, using a rat model. By collecting thousands of data points from individual rat neurons under different conditions, his lab has identified 19 different subsets of neurons with distinct responses to nerve injury. Raghuraman hopes that correlating the cells’ electrical responses with their gene transcription profiles will identify the underlying mechanisms driving chronic pain, and how different candidate drugs can influence it.
Sex and race
In the session on sex and ethnic differences in pain, Jeffrey Mogil began by pointing out a critical flaw in traditional pain research methods. Despite ample evidence that women experience more pain than men, “80 percent of preclinical studies use male rats or male mice only,” said Mogil.
That skew overlooks important differences in the biology of pain in males and females, though. In a mouse model of chronic neuropathic pain, for example, Mogil’s lab has linked chronic pain to premature shortening of chromosome ends, or telomeres – but only in male mice. Besides studying both sexes instead of just one, Mogil argued that researchers need to extend their animal studies to monitor chronic pain for longer time periods, to account for age-related phenomena such as telomere shortening.
Frank Porreca also looks at sex differences in pain, but focuses on the role of stress. Clinical data clearly show that stress exacerbates functional pain syndromes such as inflammatory bowel disease, migraine, and fibromyalgia, all of which are more prevalent in women than men.
To study such syndromes, Porreca’s team developed a mouse model in which they restrain the animals for a short time to induce stress, then treat them with a compound that causes headaches. These stress-primed mice develop allodynia, interpreting normally non-painful stimuli as painful, while controls that only got the headache-inducing compound didn’t.
While both male and female mice exhibited the same response, Porreca found that it operates through different biochemical mechanisms in the two sexes, underscoring the importance of studying both in preclinical research.
Unlike sex, race and ethnicity lack clear biological definitions.
“It’s important to keep in mind that race and ethnicity are not causal factors, but rather proxies for these many psychosocial and biopsychosocial factors, largely driven by systemic societal and environmental exposures,” said Roger Fillingim.
At the same time, the groups that suffer disproportionately from racial and ethnic health disparities are often the least-studied. That’s certainly the case in pain research and treatment. Indeed, experiments suggest that Black patients may experience more pain than white ones, but health data show they’re less likely to be treated for pain in hospitals and clinics.
Summarizing a large body of additional evidence for similar skews in various minoritized groups, Fillingim advocated more holistic approaches to pain research across and within sub-populations.
Part 5
Speakers
Alexander Chesler, PhD National Center for Complementary and Integrative Health (NCCIH), NIH
Patrik Ernfors, PhD Karolinska Institutet
Clifford Woolf, MD, PhD Harvard Medical School
Bryan Roth, MD, PhD University of North Carolina
Kelly Knopp, PhD Eli Lilly
Get the sensation
The meeting’s penultimate session focused on how sensory signals such as pain propagate toward the central nervous system. Alexander Chesler started the session with a discussion of his work on peripheral sensory neurons.
To study these cells, Chesler and his colleagues initially developed an elegant system that allowed them to probe the responses of individual mouse cells in the trigenimal ganglion, a nerve cluster that receives sensory signals. That revealed a specific subset of neurons that responded only to a painful stimulus, while other subsets responded to gentle touches. By extending the system with gene expression profiling, and correlating responses in the mouse with those in a human patient who lacks a receptor critical for mechanical sensation, the scientists are now tracing pain-sensing pathways in unprecedented detail.
Neurons aren’t the only cells carrying pain signals, though, as Patrik Ernfors has discovered. In tracing sensory circuits, he and his colleagues discovered that Schwann cells, support cells closely associated with peripheral neurons, are also stem cells that form a sensory organ under the skin.
Using genetically modified mouse models that allowed them to selectively activate these Schwann cells, Ernfors and his colleagues discovered that both the Schwann cells and their associated neurons can initiate acute pain sensations. Further work revealed that the Schwann cells also appear to become sensitized during the development of arthritis.
“We believe that we have found the mechanosensory skin organ that is associated with [mechanical pain sensation],” said Ernfors, adding that these cells could contribute to allodynia in arthritis.
Something for the pain
Clifford Woolf began the meeting’s final session, on finding new ways to treat pain, with a summary of his team’s novel approach to drug discovery. Currently, most pharmaceutical companies focus on finding compounds that can target specific cellular molecules known to be involved in pain, then trying to develop them into drugs.
In 2010, Woolf advocated an alternative strategy, screening drugs to find those that inhibit stem cell-derived pain-sensing neurons, without worrying about their mechanisms of action.
“However, the question was how to execute on this,” he said.
After extensive effort, his team can now derive the correct neuron types from patients’ cells. Screening libraries of compounds against these cells has yielded several promising hits, which inhibit pain signaling in nociceptors without affecting other cell types.
Others hope to broaden the scope of target-based drug screening, which has focused on a large and diverse class of cell surface proteins called G-protein coupled receptors, or GPCRs.
“But … when we mapped the drugs onto the phylogeny of all the [GPCRs] in the genome, only a few targets actually came out as being targets of approved drugs,” said Bryan Roth, adding that “there are many, many other potential targets for treating pain and other serious conditions.”
To test those targets, Roth’s team developed an assay that allows them to test drugs against a library encompassing 90% of GPCRs encoded in the human genome. That has revealed several new targets, which the researchers are now testing with more specific screens, ultimately hoping to develop safer opioids.
Kelly Knopp began the meeting’s final talk with the grim statistics of chronic pain: affecting about one fourth of the global population, the direct and indirect costs of this condition add up to more than a trillion dollars.
“[Meanwhile,] the probability of technical success for pain [drugs] is worse than any other therapeutic area,” said Knopp.
To address that, she and her colleagues have focused on establishing standardized protocols for phase 2 proof-of-concept trials of pain treatments. Their approach uses sophisticated statistical techniques and uniform trial designs to enable testing of many more drug candidates, without exceeding available funding and medical trial capacity.
After the presentations, a panel of speakers from the meeting discussed several of the field’s biggest challenges. Chief among them are the immense burden of opioid addiction, and the difficulty of shifting real-world clinical treatment toward less addictive but possibly less effective therapies for chronic pain. Despite the difficulties, many researchers in the field remain optimistic.
As Ilene Tracey said in her presentation, “We’re often quite doom and gloom in the pain field, [but] we’ve actually got a lot of different tools at our disposal, [and] we should be more confident about where the field has got to and where it can go quite rapidly.”
Omicron, Mandates, Prevention, and a Pancoronavirus Vaccine: Leading scientists and public health experts share stories of their work amid global questions about the Omicron COVID-19 variant.
Published December 17, 2021
By Roger Torda
Discovery; The Story from Southern Africa
The discovery of the Omicron variant in Southern Africa started with what experts call a “spike gene dropout.”
“It was identified by colleagues in Botswana and by our sequencers in South Africa,” explained Penny Moore, PhD. “We’d just been through a third wave in South Africa that was driven by the Delta variant. And what happened was a local diagnostic laboratory…started noticing an uptick in infections, and associated with that, they noticed that the diagnostic test that we routinely use was not performing optimally.”
Moore, a virologist at the University of the Witwatersrand, described the fast-moving sequence of events during a webinar hosted by The New York Academy of Sciences (the Academy) on December 14. She explained that the PCR diagnostic test looked for four genetic markers typically found on the COVID-19 coronavirus. The tests in early November showed a reduced sensitivity; they were not detecting one of the targets. “That’s something we’d previously seen, with the Alpha variant in the UK,” Moore continued. “It’s called a spike gene drop out, or spike gene target failure.” It was a red flag.
“So that’s what led us in South Africa to start sequencing very deeply,” Moore explained. “We have a really excellent, next-generation genomics consortium here in South Africa, and they moved very rapidly to target those specific diagnostic samples that were behaving differently in the diagnostic tests. And that…showed us that we were dealing with a variant that had many, many more mutations that we were used to seeing in Delta.”
“Deluged in Data”
Moore, and her colleagues, soon were “being deluged in data” as they tried to answer questions from around the world about Omicron’s properties, including transmission rates, efficacy of vaccines, and whether the new strain causes more or less severe disease than others. As Moore earlier told Nature, “We’re flying at warp speed.”
Moore was one of four prominent scientists and public health officials participating in the webinar, What You Need to Know About Omicron and Future Coronavirus Variants. The others were: Rick Bright, PhD, who heads the Rockefeller Foundation’s Pandemic Prevention Institute; Dave A. Chokshi, MD, MSc, the Commissioner of the New York City Department of Health and Mental Hygiene; and Drew Weissman, MD, PhD, a pioneer in mRNA vaccine research at the University of Pennsylvania. The program was moderated by the Academy’s Melanie Brickman Borchard, PhD, MSc.
Moore’s work, and that of her colleagues, has drawn praise from around the world. “Timing and speed is absolutely essential for getting in front of an outbreak and for saving lives,” Bright told the panelists. “And I believe the world owes a debt of gratitude to the researchers in Southern Africa for immediately sharing this virus sequence with the global GISAID community, and for rapidly notifying their government and the word of this variant.” (GISAID is a global initiative that promotes the rapid sharing of genetic sequence and epidemiological data associated with human viruses.)
New York City; Fighting Back with Multiple Responses, Exactly One Year Later
“I want to start by just recognizing that we are on, precisely, the one year anniversary of our vaccination campaign,” said Chokshi. “It was December 14 of last year when the first person in the United States, Sandra Lindsay, a nurse in Queens, was vaccinated.” The day of the webinar also marked an escalation in New York City’s measures to tamp down the pandemic. It was the first day of a vaccine mandate for children aged 5 to 11 who engage in indoor public activities.
“For New York City, we have about 160,000 children, five to 11, who are vaccinated with at least one dose so far,” Chokshi reported. “It’s a great start, but it’s only about a quarter of the total population.” He stressed that mask and vaccine mandates are only some of the tools at the city’s disposal: “We’re partnering with over 1,500 pediatrician offices. We’ve launched a school based vaccination clinic where we visited every single school that had children in that age range. And we have mobile vaccination units that are providing vaccination across the city.”
Yearning for Social Connection
Chokshi said the city would be working hard to support pediatric vaccination in the new year, including the vaccination of younger children, which he said he hoped would be approved in the first quarter. He also said that as a public health official and the father of a two-and-a-half year old daughter, he is closely following an early report out of South Africa of an increase in very young children hospitalized with COVID-19 infections.
While the Delta variant continues to circulate, and community spread of Omicron has begun in New York, Chokshi said he and his colleagues must address very human needs, as well as science.
“You know, as we are entering the holidays, people are yearning of the social connection that the holidays bring, particularly given the trials and tribulations that we’ve all been through over the past, almost two years,” Chokshi said. “And, I think as public health professionals, we have to recognize, that that is where our fellow New Yorkers, our fellow human beings, are. And so my job, and our job, is to provide the guidance and the tools to be able to facilitate people celebrating as safely as they possibly can.”
A Pancoronavirus Vaccine
Weissman, a pioneer in the development of a core technology that makes the mRNA vaccines possible, shared some background and a status report on his current efforts to create what he calls a “pancoronavirus variant vaccine”. “If you look at coronaviruses, there have been three epidemics in the past 20 years, Weissman said. “That tells us there will be more. And we can do what we did for COVID-19, which is rush and make a vaccine. But it still shuts down the world for a year and a half.” Weissman’s research focuses on another approach, creating a vaccine that prevents transmission of all coronaviruses and their variants.
Weisman said his lab’s challenge is to identify “conserved regions” of genetic sequences shared by all coronaviruses, and to direct the immune response against those targets. In the lab, Weissman said his vaccine has been effective against “all of the current variants that have appeared, and will likely work against any variants that appear in the future.” Plans are underway to begin clinical trials within about a year.
Vaccine Hesitancy
Moore described mistrust of vaccines in many communities in South Africa, including among people who work in hospitals who have a very high rate of exposure to Sars-CoV-2. “I think the barriers are in many cases the same barriers that have been faced across the rest of the world,” she said.
“There is a huge feeling of fear and helplessness in many of those communities and a lot of suspicion around vaccination…[T]here’s much talk in South Africa about the speed at which these vaccines have been developed. It’s something that we, as scientists, need to address very urgently. We need to explain that it may look like these vaccines have been develop really quickly, but it’s not true. You know, this comes out of decades and decades [of research]”
Concurrent Clinical Trials
Weissman spoke to the same issue:
“I joke with people about this because had we taken two years or three years to develop the vaccine, they would’ve yelled at us that we were too slow. What people have to understand is that RNA vaccines have been studied for 25 years. They’ve been in clinical trials for almost 20 years. This is not brand new technology,” he said.
“The nucleoside modified mRNA LMPs [lipid mRNA particles] that we’ve developed, they’ve been in clinical trials for over five years before COVID 19 hit. So even this exact platform isn’t new technology. What people have to understand is that no corners were cut in its development. What happened is the researchers, the pharmaceutical companies, the FDA, all got together and said, ‘how can we do these studies as fast as possible?’”
The answer, Weissman said, was to conduct Phase 1, 2, and 3 clinical trials concurrently, rather than serially, which would have taken several years. “So there were no corners cut,” Weissman added. “More people were studied for COVID 19 than just about any other vaccine. It was done quickly because we have an emergency.”
Testing, Testing, and Testing
Bright, who heads the Pandemic Prevention Institute at the Rockefeller Foundation, told the Academy audience that the emergency of Omicron could prompt necessary global, coordinated action—especially the expansion of testing—to control the pandemic.
“This virus has now taken hold of the human population,” Bright said, adding:
It is not going to go away on its own. We need to fight it with every tool that we have, vaccines, therapeutics, high quality masks, ventilation, air filtration, and implementing a robust testing strategy that can trigger effective contact tracing and rapid access to therapeutics. The question now for, for us, for me, is whether Omicron will remind the world of the urgency we face and drive us to real collaborative action.
The four experts all agreed a heightened focus on healthcare equity is necessary to control the pandemic. “Vaccine inequity is prolonging the COVID-19 pandemic and it’s jeopardizing all the progress that we’ve made to date,” Bright said, pointing out that people who are unvaccinated remain significantly more likely to get sick from COVID-19, to pass it on to others, and to facilitate the emergence of new variants.
Equity: An Important Factor
Chokshi said equity has been an important focus of efforts in New York City, especially in lowering barriers to access. This means bringing vaccines “into people’s communities, into their neighborhoods.” He cited as examples: “Partnering with federally-qualified health centers. Moving to a decentralized approach where we use mobile sites, and also using in-home vaccination which is now available to anyone 12 and up across New York City.”
Another part of New York City’s efforts, Chokshi said, is building trust:
“We worked on building vaccine confidence with our partners across New York City, knowing that government is one messenger, but that often it is not the most trusted messenger within communities. So we are partnering with faith leaders and community based organizations to build vaccine confidence.”
The Mission of the Academy
An important point that emerged in the December 14 discussion aligns closely with the mission of the Academy, that while science plays a central role in the global response to the pandemic, scientists must partner with members of many other communities, and with experts from many disciplines.
“We have to also realize that science alone can’t keep us safe,” Bright said. “We need to ensure that governments and companies and communities, and even individuals such as ourselves, are working together. We’re sharing information, we’re making decisions based on science…to stop this outbreak.”
This type of collaborative effort is a goal of an important new Academy initiative, the International Science Reserve (ISR). The project aims to mobilize scientists and critical resources in the face of future global crises, whether a new pandemic, a cyber attack, flooding, or a massive wildfire.
The Academy’s program on the Omicron variant was just the latest in a broad series starting early last year, all designed to help meet the need for unbiased, scientific information on Sar-CoV-2. Next in line is a symposium on March 30 and March 31, The Future of Vaccinology. The program will feature speakers from the Bill and Melinda Gates Research Institute, Pfizer, Novavax, and the Human Vaccines Project.