Motivated to help his son battle a rare genetic disorder known as NGLY1, this researcher has transition from the field of computer science to biology and drug development.
Matthew Might, Director, Hugh Kaul Precision Medicine Institute at the University of Alabama at Birmingham is a computer scientist by training but now works in the field of drug repositioning. His research is dedicated to finding new therapeutic purposes for already existing drugs. Recently he sat down to discuss his work.
How would you describe your work?
As a researcher I’m focused directly on scaling up the process of drug repositioning for specific rare and medically complex patients. I’m investing heavily in the creation of bioinformatics infrastructure that allows us to repurpose drugs and implement a workflow that can guide patients through the identification of a therapy.
What brought you to the field of drug repositioning?
My shift from computer science to medicine was motivated entirely by my son Bertrand. He is the first discovered case of an ultra-rare genetic disorder known as NGLY1 deficiency. The lack of any available treatments inspired me to look for existing medications that could be repurposed to treat his disease. Over time I was able to use a variety of techniques to find three different compounds with some therapeutic potential for his disorder.
How difficult was transitioning from computer science to medicine?
The transition was gradual. Initially, I learned about genetics, and then I began reading about glycobiology, which is an interesting way to learn biology. After learning enough glycobiology and about metabolism, I made some predictions about what Bertrand might be deficient in. That led to the discovery of the first natural product that serves as a therapy for his disorder.
Six years was the total time it took to go from computer science to having enough biology to make a reasonable therapy prediction. I wouldn’t have done this without the personal motivator, but I think this is not just the right time to have more computer science in biology. It’s the right time to have more computer scientists in biology.
When looking for drug repositioning candidates do you identify a disease or treatment first?
Matthew Might
We start with the disease. When a patient comes in with a rare monogenic disease, we ask four questions about the gene: ‘Is the gene overactive? Is it underactive? Is activity absent? Or has its activity become toxic?’ These answers tell us what direction to go.
The two most common directions are genes that have a gain of function or partial loss of function. We’re going to be manipulating the gene that has a variant. The tools we’ve developed are capable of answering questions like, ‘Given a gene, how do I modulate its activity up or down through any mechanism whatsoever?’ A lot of what we do is harvesting data sets that enable us to answer that specific question better.
What’s the biggest challenge in identifying drugs to be repositioned?
From a bioinformatics perspective the challenge we face is that only a small fraction of genetic targets have a candidate drug known to hit them. This isn’t a limitation of the drugs, it’s a limitation of our knowledge about them. If I could have the NIH fund one experiment, it would take all approved drugs and do an exhaustive transcription against many cell lines. That would show the impact of every drug on every cell type, on every gene. If we had that database, we could do much more drug repurposing.
How do you get these treatments to patients?
Once we’ve found a target, we will do whatever we can computationally to find a compound that might modulate the target. If we get lucky and we hit it computationally, we will end up generating a research report. We do this when we find an approved compound, or a natural product that’s already available.
The report is a factual summary of the information we’ve discovered about the compound and includes research papers that back this up. We turn that report over to the patient’s treating physician. At that point, it’s up to the treating physician to decide what to do.
While the development of vaccines against infectious diseases has had a profound impact on life expectancy, there remain many resistant and emerging infections for which no effective vaccines are available, such as malaria, HIV, and Zika. Recent advances in biotechnology and our understanding of human immunity hold great promise for conquering new diseases. For example, advances in structural biology allow for the discovery of new antigens that can target broad viral families, such as influenza, or complex parasites like malaria. Novel clinical trials for maternal immunizations have shown encouraging results for reducing dangerous diseases in newborn infants. Furthermore, recent progress in DNA- or RNA-based vaccines holds promise for inexpensive and fast production, which is especially favorable for responding to emerging epidemics. Learn more about recent breakthroughs in vaccine development in this summary of our May 20, 2019 symposium, which gathered the world’s leaders in vaccine development.
Symposium Highlights:
Emerging infectious diseases can be treated quickly with a passive vaccine containing human monoclonal antibodies isolated from the blood of an infected patient.
Targeting multiple stages of the malaria life cycle is a promising strategy for the development of a successful vaccine targeting this complex parasite.
Clinical trials show promise for maternal immunizations in protecting newborn infants from respiratory syncytial virus (RSV) and Group B streptococcus.
A vaccine containing the influenza hemagglutinin (HA) fusion protein without the head domain can elicit protection against a broad group of influenza viruses.
Synthetic DNA and mRNA vaccines are simple to manufacture and show promise for treating a wide range of diseases, including Ebola, HIV, Zika, influenza, and malaria.
A promising new adjuvant, AS01, has contributed to breakthrough vaccines for Malaria, tuberculosis, and shingles.
Speakers
James E. Crowe, Jr., MD Vanderbilt University Medical Center
New Approaches for Understanding the Immune System for Vaccine Development
Speaker
James E. Crowe, Jr. Vanderbilt University Medical Center
Human Antibodies and Repertoires for Emerging Infectious Diseases
James Crowe, of Vanderbilt University Medical Center, discussed his lab’s work developing treatments for emerging infectious diseases using monoclonal human antibodies. “Antibodies essentially are a passive vaccine,” explained Crowe. Currently, it takes about two years to develop a vaccine for an infectious disease agent, which is not quick enough for outbreak response. Therefore, Crowe argues that antibodies are the “most appropriate public health measure for most emerging infections.” Crowe’s group is working on two strategies for developing human antibody drugs: one focuses on speed, whereas the other aims to develop broad antibodies ahead of an outbreak.
The Rapid Rational Antibody Design and Delivery (RRADD) project uses ultra-fast techniques to respond to a specific outbreak in the moment. They recently used Zika as a test case. Starting with a blood sample from a surviving patient, their facility used single-cell RNA-sequencing to produce a list of antibody genes within a day. These antibodies were quickly produced and then tested in a high-throughput real-time cell culture system to assay for protection against Zika infection. Leading candidates were tested in mouse and primate models, leading to the discovery of protective antibodies within 78 days.
Illustrations of antibody (Ab)- antigen (Ag) complexes for human monoclonal antibodies (mABs) recently discovered in the AHEAD100 project.
The second strategy is the Advanced Human Epidemic Antibody Defenses (AHEAD100) project, a methodical approach that aims to develop antibodies for the 100 most likely infectious diseases ahead of any future outbreaks. Interestingly, they found broad antibodies that work across viruses of a related class, such as noroviruses, alphaviruses, and flu.
Taking on the Big Challenges Facing Novel Vaccine Development
Adrian Hill University of Oxford
Wayne Koff Human Vaccines Project
New Generation Malaria Vaccines
Adrian Hill from the University of Oxford presented his work on the development of a malaria vaccine. Malaria causes 500,000 deaths each year, but developing an effective vaccine is challenging. “Even if you get a good antigen, you need remarkably high immunogenicity,” Hill explained. Therefore, Hill’s group aims to develop a vaccine that targets multiple stages of the malaria parasite life cycle.
In the first stage, mosquitos introduce malaria sporozoites into a human host. Hill’s group and others have been developing vaccines that combine malaria antigens with virus-like particles to induce antibody production against sporozoites. Hill and colleagues are developing R21, a more potent version of the RTS,S vaccine currently in Phase III trials. In R21, 100% of the molecules encode the sporozoite antigen. Studies show that this formulation allows for a lower dose, as antibody titers are indistinguishable between a 10 µg dose of R21 and a 50 µg dose of RTS,S. Furthermore, R21 shows a more durable response, with higher titers at six months versus RTS,S. By 2020, they expect efficacy results from the first Phase IIB trial.
As the malaria life cycle progresses, sporozoites infect liver cells, where the parasite matures. “[To target] the liver stage, you need T-cells” said Hill. Inducing T-cells requires a viral vector approach. Research on mice and clinical studies from Hill’s group show that the ME-TRAP antigen viral vector can induce high levels of resident memory T-cells in the liver. There are ongoing field clinical trials for this vaccine.
The Future of Vaccine Development
Wayne Koff, the president and CEO of the Human Vaccines Project, described the nonprofit’s research decoding the human immune system. Vaccines for complex infectious and non-communicable diseases such as HIV, tuberculosis, and cancer have been difficult to develop. Koff believes that a better understanding of human immunity is essential for accelerating vaccine development for these diseases.
One strategy is to investigate why some people respond to vaccines and infections much better than others. “If we can understand this, we can get at the pathogens we haven’t been able to tackle,” said Koff. Recent developments in single cell multi-omics allow for an in-depth analysis of an individual’s immune system. A growing body of evidence suggests that immunity biomarkers at baseline can predict an individual’s response to immunization. Researchers performed single cell RNA-sequencing on innate immune cells before immunization and successfully identified biomarkers predictive of the response to the Hepatitis B vaccine. By integrating all of the pre-immunization data, investigators could build biostatistical models that accurately predicted final antibody titers, while revealing pathways that may be involved in the response mechanism.
This data suggests that “we all have an immune set point,” said Koff, which leads to the opportunity to modulate this set point before immunization to improve outcomes. Furthermore, smaller trials that account for individual variability and assay predictive signatures may be more effective than standard large vaccine efficacy trials.
Kathrin Jansen from Pfizer discussed recent advances in maternal immunization. Infants under six months are the most vulnerable to infection, but most vaccines are not available at this early stage of life. Furthermore, “20% of stillbirths seem to be associated with an infectious disease,” said Jansen. Active antibody transfer from mother to baby during pregnancy is an essential mechanism for protecting infants from infectious diseases. The goal of maternal immunization is to enhance maternal antibody levels to further protect newborns. Jansen explained that these vaccines could either “augment pre-existing antibody responses or induce a de novo response” to infections the mother has not yet been exposed to.
Jansen presented recent findings for maternal vaccines targeting respiratory syncytial virus (RSV) and Group B streptococcus bacteria, two infections that are especially deadly for newborn infants. In a recent Phase I/II trial, the Group B streptococcus vaccine induced high levels of antibody titers for up to six months in healthy adults, giving confidence to move forward for testing in pregnancy. Recent structural biology studies of RSV identified a metastable form of the viral fusion protein. With this form in mind, a screen for vaccine candidates revealed molecules that were 30 times more powerful than the current licensed prophylactic antibody in rodents. Data from a Phase I/II study will be available later this year.
Protecting Infants from RSV via Maternal Immunization
Greg Glenn, of Novavax, presented recent progress on the development of an RSV maternal vaccine. RSV is the leading cause of hospitalization of infants in the United States. While the Pfizer version of the vaccine, described by Kathrin Jansen, resembles the metastable prefusion form of the viral fusion protein, the Novavax version targets an earlier, stable form known as the prefusogenic form. This vaccine contains a near full-length fusion protein, but with deletions in a furin cleavage site. “These deletions fix the protein structure, and that allows it to be very stable,” Glenn explained. Through stabilizing the prefusogenic form, the virus is prevented from successfully infecting cells, which allows the vaccine to be produced in culture with higher yields. Furthermore, all antibodies that target the metastable prefusion form also target the prefusogenic form. Immunization with the Novavax vaccine induces antibodies to a variety of viral epitopes, which are also transferred to the infant.
Schematic showing the different forms of the fusion (F) protein of the RSV virus.
Currently, Novavax is running a worldwide Phase III randomized placebo-controlled trial to evaluate protection of infants against RSV with their maternal vaccine. The vaccine was given “to immunized mothers in third trimester, and we monitored infants intensely for six months,” explained Glenn. The trial showed a 40% reduction in their primary endpoint, which was medically significant RSV lower respiratory tract infection at 90 days old.
Next Generation Vaccines to Eliminate Congenital Cytomegalovirus: We are halfway there
Sallie Permar, of Duke University, shared her work developing an effective vaccine for congenital cytomegalovirus (CMV), which is the most common congenital infection and cause of birth defects worldwide. Developing a vaccine has been tricky, as it’s unknown exactly what maternal immune responses are protective against congenital CMV transmission. Permar’s group is investigating these questions with a novel, non-human primate model as well as data analysis from previous vaccine trials.
Permar and colleagues infected seronegative rhesus monkeys with CMV at the beginning of pregnancy. “We used a model of severe pathology with maternal CD4+ T-cell depletion followed by an intravenous inoculation to ask whether antibodies alone could be protective against congenital CMV transmission,” explained Permar. Data from a small group of animals suggests that treatment with passive antibodies from donor plasma prior to inoculation prevents fetal transmission. This result indicates that stimulating potent antibody responses could be a promising route to an effective maternal CMV vaccine.
Previous trials of a vaccine containing glycoprotein B, the main fusion protein of the virus, have shown partial effectiveness. Permar’s group probed the trial data to investigate what immune responses correlate with protection against CMV in infected versus uninfected vaccine recipients. “The ability of vaccine-elicited antibodies to bind to glycoprotein B-transfected cells was higher in uninfected vaccinees,” said Permar, suggesting that eliciting antibodies that bind to glycoproteins is a promising vaccine target. Furthermore, the infected group of vaccine recipients was still protected against specific CMV strains, suggesting that a broader immunogen might be more effective.
Guiding Vaccine Candidates: Antibodies That Can Neutralize Influenza and Malaria
Ian Wilson, from the Scripps Research Institute, shared his recent work investigating the structural biology of antibodies to guide vaccine candidates for influenza and malaria. Wilson’s group aims to “design immunogens or even small molecules from the structural information about how antibodies bind.”
Human antibodies that neutralize a broad range of flu subtypes have been characterized in the last ten years. Interestingly, the broadest antibodies bind to the less immunogenic “stem” domain of the influenza hemagglutinin (HA) fusion protein, rather than the “head” domain. “We are using this information to try to think of novel vaccines,” said Wilson. “If we chop off the immunogenic head, then we can target the response against the stem.” Indeed, a recently developed headless HA construct elicited protection against all influenza A group 1 antibodies in mice and monkeys.
Wilson’s group has also probed the structural biology of human antibodies elicited in recent RTS,S malaria vaccine trials. Cryo-EM revealed the structure of antibodies binding to the circumsporozoite protein (CSP) of malaria: the antibodies spiral all the way around the NANP peptide repeats of the protein. Furthermore, antibodies in the spiral bind in close proximity, and often, somatic mutations strengthen these homotypic contacts for a more stable spiral. Future work will explore the relevance of this spiral structure for vaccine purposes.
Synthetic DNA Approaches for Difficult Infectious Disease Targets
David Weiner, of the Wistar Institute, presented recent findings on the development and efficacy of synthetic DNA vaccines. DNA vaccines are “very consistent, very simple to manufacture, temperature stable,” and allow for local transfection without systemic expression, explained Weiner. Recent early stage clinical trials have shown promising results for using synthetic DNA vaccines as immunotherapy to treat human papillomavirus (HPV)-related cancers. Synthetic DNA is also promising for treating emerging infectious diseases. Wiener discussed three examples, Ebola, MERS, and Zika, where prophylactic treatment with synthetic DNA induced a 95%–100% response rate, and transmission into the clinic occurred in only 7–15 months.
Weiner also discussed his group’s work developing a DNA-encoded monoclonal antibody (dMAb) platform. Muscle or skin tissue “is transfected and becomes a factory for expression of the protein. The idea is getting [the antibody] secreted into the bloodstream at detectable levels,” said Weiner. They have developed dMAbs targeting Ebola, HIV, and Zika that induce robust antibody expression and viral protection in animal models. For HIV, multiple dMAbs can be delivered at one time, which has been shown to induce broad neutralizing titers against nine HIV subtypes in non-human primates.
Weiner and collaborators are also working to engineer DNA cassettes that encode self-assembling nanoparticles directly in vivo. Nanoparticles targeting HIV showed improved immune responses versus the monomeric form: “It’s dose sparing, it’s much faster seroconversion and much higher titers, and it elicits very good CD8+ T-Cells,” Weiner said.
mRNA Vaccines: A New Era in Vaccinology
Drew Weissman, of the University of Pennsylvania, discussed recent advances in the development of mRNA vaccines for infectious diseases. Why use RNA? In theory, the cost of mRNA production would be much less than that of protein, which requires large-scale cell culture followed by purification that differs for every protein. Weissman’s group developed a platform using nucleoside-modification and purification techniques to optimize mRNA structures that induce high and long-lived translation when delivered within lipid nanoparticles to peripheral sites.
Mice vaccinated with the A/Cal/7/2009 HA mRNA vaccine challenged with the distant flu virus H5N1 showed full protection. These results suggest immunization with HA mRNA could result in a universal flu vaccine.
Weissman discussed mRNA vaccines developed with their platform targeting influenza, HSV-2, HIV, and malaria, which have all shown promising results in animal models. For influenza, a single immunization with an mRNA vaccine coding for the hemagglutinin (HA) fusion protein in mice resulted in titers 50 times higher than the current FDA approved vaccine. As a mechanism of action, they found that the lipid nanoparticles used for vaccine delivery induce T- follicular helper cells, which drive long-term immune memory and are “critical in the induction of potent antibody responses,” explained Weissman. Furthermore, their mRNA vaccines induce responses to subdominant epitopes in the presence of dominant epitopes, which isn’t seen with whole proteins. This response is useful because subdominant epitopes, such as the HA stem domain, can be broadly cross-reactive across viral subtypes. Vaccinated mice challenged with distant flu viruses were fully protected, “suggesting that using a full HA could give you a universal vaccine,” said Weissman.
Transforming New Technologies into Vaccines: Genomics, Adjuvants and Self-Amplifying RNAs
Rino Rappuoli, of GlaxoSmithKline, shared how new technologies will allow us to conquer new diseases. Recent advances have allowed for major improvements in reverse vaccinology — using human genomics and structural biology to discover new antigens and instruct vaccine design. “Today we have the tools of synthetic biology,” said Rappuoli. At GSK, “we are using self-amplifying mRNA instead of simple mRNA. We use the replicon of the alphavirus to amplify the RNA and give a better response.” Nucleic acid vaccines work well in animal models, and the challenge now is testing whether it will work well in humans.
Rappuoli also discussed encouraging new advances in antigen delivery using nanoparticles or Generalized Modules for Membrane Antigens (GMMA). While self-assembling natural nanoparticles have been around for years, fully synthetic nanoparticles have only recently been designed. “We are going from mimicking nature to completely computationally designing vaccines,” explained Rappuoli. GMMAs consist of outer membrane vesicles from bacteria, which are engineered to release these vesicles in large quantities with the desired antigens. Rappuoli also highlighted recent developments in adjuvants, substances within vaccines that enhance the immune response to antigens. A promising new adjuvant, AS01, has contributed to breakthrough vaccines for Malaria, tuberculosis, and shingles. Moving forward, Rappuoli aims to use these new technologies to target vaccines for the elderly, emerging infections, and antimicrobial resistance.
“Optimized degrader molecules will have fast rates of degradation and relatively short exposure with therapeutic doses that result in complete elimination of the target protein, which can result in a more durable and deeper effect.”
Published July 23, 2019
By Robert Birchard
Eric Fischer, PhD
Around 80% of disease-causing proteins, including key drivers of many cancers and other serious neurological conditions like Alzheimer’s disease, cannot be targeted by currently available therapeutics. These so called “undruggable” proteins lack specific surface areas required for treatments such as small molecule inhibitors or antibodies to bind with disease causing proteins and modulate their function.
However, an alternative therapeutic strategy known as targeted protein degradation has shown the potential to remedy these “undruggable” proteins. Utilizing small molecules known as PROTACs, this strategy harnesses the cell’s waste disposal system to promote the destruction of disease-causing proteins. Dr. Eric Fischer, Assistant Professor of Biological Chemistry and Molecular Pharmacology at Harvard Medical School, recently sat down with us to help create this primer on PROTACs, and their potential implications for treating disease.
What are PROTACs?
PROteolysis TArgeting Chimeras, or PROTACS for short, are two separate molecules bound together to form a two headed molecule. One end binds to an ubiquitin ligase, while the other end binds to the “undruggable” protein targeted by pharmacologists. In illustrations, PROTACs are often depicted as dumbbells, but it may be more helpful to think of them as flexible harnesses.
How do PROTACs work?
PROTACs are designed to take advantage of the cell’s waste disposal system that removes unneeded proteins. This system, known as the proteasome, is important for the cell to remove unneeded or damaged proteins and recycle their building blocks to make new proteins. The proteasome plays critical roles in cell growth, management of cellular stress, and in the immune system. One end binds to the targeted proteins, while the other end of the molecule binds to the ubiquitin ligase, which then marks the targeted protein for destruction. This lets the cell’s proteasome know that this specific protein can be destroyed. In this way the body’s regularly occurring mechanisms are co-opted to destroy disease-causing proteins.
Optimized degrader molecules will have fast rates of degradation and relatively short exposure with therapeutic doses that result in complete elimination of the target protein, which can result in a more durable and deeper effect.”
Eric Fischer, PhD
What makes PROTACs so unique?
Most therapies are divided between small molecule inhibitors or therapeutic antibodies/biologics. However, “PROTACs are small molecules and as such not restricted to targeting surface proteins, however, in contrast to traditional small molecule inhibitors, PROTACs are fundamentally different,” explained Dr. Fischer, “While inhibitors need to achieve an almost perfect degree of target engagement over an extended period of time to exert their pharmacologic effect, PROTACs follow more of a hit and run strategy.”
“Optimized degrader molecules will have fast rates of degradation and relatively short exposure with therapeutic doses that result in complete elimination of the target protein, which can result in a more durable and deeper effect,” he explained. “More importantly, however, small molecule degraders completely eliminate the disease-causing protein and as such can target the non-catalytic activity of enzymes but also scaffolding proteins, and other non-enzymatic targets.”
When will PROTACs be more widely available?
While researchers have demonstrated the potential of PROTACs in the lab, the first clinical trials are just opening. Still Dr. Fischer is very optimistic, “The technology has rapidly spread, and we can expect to see many more programs entering clinical development. Due to the pioneering work of a growing academic community spearheading this field, the concepts underlying protein degradation are largely public domain and widely available.”
What is the future of PROTACs research?
“I believe the field of targeted protein degradation is here to stay and will significantly expand our repertoire of therapeutic modalities,” said Dr. Fischer. “I also believe it is still in its infancy and many challenges lie ahead of us to broadly deploy this to the more challenging targets.” PROTACs could potentially prove the impossible is possible by allowing scientists to destroy disease-causing proteins that were previously considered beyond their reach.
Sthuthi Satish is exploring her interest in a variety of STEM fields through her participation in the Junior Academy, but her first experience with the wonders of science started very close to home.
Published May 1, 2019
By Mandy Carr
Sthuthi Satish
Sthuthi Satish can’t remember when she started dreaming of being a doctor. What she does remember is being seven years old and looking at her mother’s medical charts showing stage two cancer. Her mom underwent surgery and beat cancer and Sthuthi’s love for surgery began.
The 15 year-old, who attends Bangalore International School in India, admits to not understanding the complications of surgery then, but saw the possibilities of it. Today, she hopes to become a neurosurgeon.
“My love for the brain is rather recent,” she said. “I am fascinated by the fact that the brain controls pretty much all conscious actions in the human body, and yet we know so little about it.”
Building Upon Previous STEM Experience
Sthuthi had few opportunities to join STEM activities before participating in the New York Academy of Sciences’ Junior Academy program. She worked on many challenges focusing on sustainability and aerospace. She worked with other high school students from across the globe as part of the winning team for the Human-Wildlife Challenge.
Sthuthi was concerned that no one was addressing the negative effects of solar panels on wild birds. Her team believes that infrared sensors and speakers producing beeping noises at 3 kHz can deter birds from landing on solar panels.
During her first year in the Junior Academy, she saw a posting on Launchpad, the Academy’s virtual collaboration platform, about getting involved in a Girls in Science panel at the third annual International Day of Women and Girls in Science event at the United Nations Headquarters in New York City. She stayed in touch with one of the organizers, HRH Princess Dr. Nisreen El-Hashemite, Executive Director of the Royal Academy of Science International Trust which lead to an invitation from Dr. El-Hashemite to chair a panel at the 2019 event.
Finding What Drives Her
This is also how she became a Girls in Science Advocate for the Royal Academy of Science. Additionally, Sthuthi is one of the administrators on the Girls in Science 4 SDGs International platform, a program Dr. El-Hashemite made possible. For Sthuthi it’s all about priorities.
“I always believe that if I have enough time to watch Netflix, then I definitely have time to work on something I love,” she said. Sthuthi hopes to attend college either in the United States or Sweden.
The next decade will be a pivotal one for the integration of AI and Big Data into healthcare, bringing both tremendous advantages as well as challenges.
Suchi Saria, PhD
Published May 1, 2019
By Sonya Dougal, PhD
One of the most common causes of death among hospital patients in the United States is also one of the most preventable — sepsis.
Sepsis symptoms can resemble other common conditions, making it notoriously challenging to identify, yet early diagnosis and intervention are critical to halting the disease’s rapid progress. In children, for each hour that sepsis treatment is delayed, the risk of death increases by as much as 50 percent.
Novel innovations, such as the one pioneered by Suchi Saria, director of the Machine Learning and Healthcare Lab and the John C. Malone Assistant Professor at Johns Hopkins University, are helping to reverse this trend. In 2013, Saria and a team of collaborators began testing a machine learning algorithm designed to improve early diagnosis and treatment of sepsis.
Using troves of current and historical patient data, Saria’s artificial intelligence (AI) system performs real-time analysis of dozens of inpatient measurements from electronic health records (EHRs) to monitor physiologic changes that can signal the onset of sepsis, then alert physicians in time to intervene.
“Some of the greatest therapeutic benefits we’re going to see in the future will be from computational tools that show us how to optimize and individualize medical care,” Saria said. She explained that the emergence of EHRs, along with the development of increasingly sophisticated AI algorithms that derive insights from patient data, will fuel a seismic shift in medicine — one that merges “what we are learning from the data, with what we already know from our best physicians and best practices.”
Nick Tatonetti, PhD
Electronic Health Records: A Gold Mine for Computer Scientists
EHRs have become a data gold mine for computer scientists and other researchers who are tapping them in ways designed to improve physician-patient encounters, inform and simplify treatment decisions, and reduce diagnostic errors. Like many other technological advances, though, there are those physicians who regard EHR systems with less enthusiasm.
A 2016 American Medical Association study revealed that physicians spend nearly twice as much time engaged in EHR tasks than they do in direct clinical encounters. Physician and author Atul Gawande recently lamented in The New Yorker that “a system that promised to increase my mastery over my work has, instead, increased my work’s mastery over me.”
Yet, data scientist Nicholas Tatonetti, the Herbert Irving Assistant Professor of Biomedical Informatics at Columbia University envisions a day when such AI algorithms will enable physicians to deepen their interaction with patients by freeing them from the demands of entering data into the EHR. Tatonetti has designed a system using natural language processing algorithms that takes accurate notes while physicians talk with patients about their symptoms. Like Saria’s AI system, Tatonetti’s takes advantage of the vast amount of data captured in EHRs to alert physicians in real time to potentially dangerous drug interactions or side effects.
Unknown Interactions
Anyone who has filled a prescription is familiar with the patient information leaflet that accompanies each medication, detailing potential side effects and known drug interactions. But what about the unknown interactions between medications?
Ajay Royyuru, PhD
Tatonetti has also developed an algorithm to analyze existing data in electronic health records, along with information in the FDA’s “adverse outcomes” database, to tease out previously unknown interactions between drugs. In 2016, he published a study showing that ceftriaxone, a common antibiotic, can interact with lansoprazole, an over-the-counter heartburn medication, increasing a patient’s risk of a potentially dangerous form of cardiac arrhythmia.
As data-driven AI techniques become more accessible to clinicians, the treatment of conditions both straightforward, like hypertension, and highly complex, such as cancer, will be transformed.
A Paradigm Shift in Physician-Patient Interactions
Ajay Royyuru, vice president of healthcare and life sciences research at IBM and an IBM Fellow, explained that, “when a practitioner makes a patient-specific decision, the longitudinal trail of information from thousands of other patients from that same clinic is often not empowering that physician to make that decision. The data is there, but it’s not yet being used to provide those insights.”
In the coming years, physicians and researchers will be able to aggregate and better utilize EHR data to guide treatment decisions and help set patients’ expectations.
The ability to draw on information from tens or even hundreds of thousands of patients, in addition to a physician’s own experience and expertise, could represent a paradigm shift in physician-patient interactions, according to Bethany Percha, assistant professor at the Icahn School of Medicine at Mount Sinai, and CTO of the Precision Health Enterprise, a team that turns AI research into tangible products for the health system.
“Big Data offers us the promise of using data to have a real dialogue with patients — if you’re newly diagnosed with cancer, it means giving people a realistic, data-driven assessment of what their future is likely to be,” she said.
Biases and Pitfalls
Despite the surge of interest and investment in AI over the past two decades, significant barriers to its widespread application and deployment in healthcare remain.
AI systems that tap current and historical patient health data risk reinforcing well-noted biases and embedded disparities. Medical research and clinical trials have long suffered from a lack of both ethnic and gender diversity, and EHR data may reflect patient outcomes and treatment decisions influenced by race, sex or socioeconomic status. AI systems that “learn” from datasets that include these biases will inherently share and perpetuate them.
Percha noted that greater transparency within the algorithms themselves — such as systems that learn which features an algorithm uses to make a prediction — could alert users to obvious examples of bias. Removing bias from AI algorithms is a work in progress, but the research community’s awareness of the issue and efforts to address it mirror a greater push to eliminate bias and decrease inequities in medicine overall. Optimistically, Percha noted that Big Data and AI may ultimately help create a more level playing field in healthcare delivery.
“Clinical decisions made on the basis of data have the potential to be much more standardized across different health facilities, so people who are in a rural area, for example, might have access to the same decision-making benefits as someone in a city,” she said.
Patient Data Privacy
Ensuring patient data privacy is another hot-button issue. Training artificial intelligence systems requires access to massive troves of patient data. Despite the fact that this information is anonymized, some patient advocates and bioethicists object to this access without explicit permission from the patients themselves.
Another privacy issue looms equally large: how to safely collect and protect the streams of potentially useful health data generated by wearable devices and in-home technologies without making patients and consumers feel, in Royyuru’s words, “like they are living their lives in front of a camera.” Studies have shown that data from smartphone apps can provide valuable information about the progression of certain diseases, such as Parkinson’s.
Wearables and in-home IoT devices can also extend the realm of clinical observation well beyond the doctor’s office, revealing, for example, important details about a Parkinson’s patient’s ability to complete the tasks of daily living. Yet Royyuru emphasizes that unless patients trust that their data will be kept private and ethically utilized, these technologies will fizzle long before they’re widely adopted.
Building Trust
The next decade will be a pivotal one for the integration of AI and Big Data into healthcare, bringing both tremendous advantages as well as challenges. Some applications of AI, such as image recognition, are already especially well-suited to healthcare — AI algorithms often match or even outperform radiologists in interpreting medical images — while others are far from ready for widespread use.
Saria, who has deployed her system successfully at multiple hospitals says, “physicians often greet news of AI breakthroughs with skepticism because they’re being over-promised results without clear data demonstrating this promise. True integration and adoption of AI requires not just careful attention to physician workflows, but transparency into exactly how and why an algorithm has arrived at a particular recommendation.”
Rather than replacing or challenging a physician’s place in the healthcare ecosystem, Saria believes that AI has the ability to lighten the load, and as algorithms improve, generate diagnostic and treatment recommendations that physicians and patients can both deem trustworthy.
“We are still figuring out how to make real-time information available so that it’s possible for physicians or expert decision-makers to understand, interpret and determine the right thing to do — and to do that in an error-free way, over and over again,” Saria said. “It’s a high-stakes scenario, and you want to get to a good outcome.”
Mark Shervey, Max Tomlinson, Matteo Danieletto, Sarah Cherng, Cindy Gao, Riccardo Miotto, and Bethany Percha, PhD, Mount Sinai Health System, Icahn School of Medicine at Mount Sinai.
The Honorees of the 2019 Innovators in Science Award are tapping the potential of stem cells.
Published May 1, 2019
By Hallie Kapner
Stem cells are the ultimate asset in the body’s efforts to heal damage and repair wounds. These powerhouses of regeneration are responsible for maintaining the integrity of skin, bone and other tissues. The 2019 Innovators in Science Award, sponsored by Takeda Pharmaceuticals, recognizes two outstanding researchers in the field of regenerative medicine. The Senior Scientist and Early-Career Scientist winners are advancing our understanding of the miraculous inner workings and remarkable healing powers of stem cells.
Turning Stem Cell Research into Life-Saving Therapies
Michele De Luca, MD
Michele De Luca, MD, first encountered epithelial stem cells in the 1980s, during a research fellowship at Harvard Medical School in the lab of stem cell therapy pioneer Howard Green.
“I fell in love with the concept, the cell type, and the system,” he said, describing how the thrall of regenerative medicine — then in its infancy — would come to dominate the next thirty years of his career.
De Luca, winner of the Senior Scientist Award and director of the Center for Regenerative Medicine “Stefano Ferrari” at the University of Modena and Reggio Emilia in Modena, Italy, has made fundamental discoveries in the molecular and genetic characteristics of epithelial stem cells, translating those findings into therapies that change and save patients’ lives.
De Luca’s earliest clinical triumphs in skin regeneration were in the treatment of burn patients. Using the patient’s own epidermal stem cells, De Luca grew skin grafts in culture, then successfully used them to repair large lesions. In collaboration with Graziella Pellegrini, professor of cell biology at the University of Modena and Reggio Emilia, De Luca went on to pioneer new stem cell culture and grafting techniques, ultimately developing the first corneal regenerative therapy, Holoclar, which utilizes limbal stem cells to generate healthy corneal tissue for patients who have sustained chemical burns or other ocular injuries. The technique, which can restore lost sight in some cases, was approved by the European Medical Agency as a commercial stem cell therapy in 2015.
Decades of research, experimentation, and clinical trials prepared De Luca well for the day (later that same year) when he first learned of a seven-year-old boy in Germany suffering from a debilitating and often fatal skin condition, junctional epidermolysis bullosa, which is caused by a genetic mutation. Working against the clock, De Luca and a team of collaborators in Modena and Germany attempted a highly experimental epithelial stem cell gene therapy.
The team used a retroviral vector to introduce a functional copy of the mutated gene into the patient’s stem cells, then rapidly grew healthy sheets of skin for transplantation. Three years later, the transgenic skin grafts remain symptom-free. De Luca noted that his case has provided critical insights into epidermal stem cell biology and the potential for using gene therapy for other skin conditions.
“To me, this is the essence of regenerative medicine, and this is the future,” he said.
Decoding the “Crosstalk” Between Epithelial Stem Cells and the Immune System
Shruti Naik, PhD
Shruti Naik, PhD, assistant professor in the departments of pathology, medicine, and dermatology at NYU School of Medicine and winner of the Early-Career Scientist Award, is exploring the interplay between immune cells, stem cells, and resident microbes in epithelial tissues.
By eavesdropping on what she describes as a “vital conversation” between these groups, Naik hopes to better understand how their interplay with each other — and with the external environment — facilitates healing and regeneration. Her work is also providing insight into the devastating conditions that can result when these systems break down, such as non-healing wounds and ulcers.
Naik’s work aims to systematically decode the dialogue among various cell communities within barrier tissues as they encounter and respond to external stimuli or injury, with a particular focus on the role of epithelial stem cells, which play pivotal yet poorly understood roles in the body’s defensive and regenerative processes. Naik’s research has revealed surprising sensitivities and attributes of these cells.
“Stem cells are actually exquisite sensors of inflammation, and we’ve discovered that they can even remember inflammation and change their behavior accordingly,” she said.
This cellular memory can promote healing by “tuning” the stem cells to respond and regenerate tissue more quickly.
Understanding which immune signals modulate the activity of stem cells, and how the microbial communities of the skin, lung, and gut can influence the process of tissue repair, may lead to new therapeutic approaches for chronic ulcers and other wounds.
“We’re really at the beginning of a new era of understanding how stem cells sense inflammatory and stress signals and incorporate them into generating new tissues,” Naik said.
From a focus on immunotherapy to better understanding intratumoural heterogeneity, these researchers are making significant advances in cancer treatment.
Published April 15, 2019
By Marie Gentile, Robert Birchard, and Mandy Carr
According to the American Cancer Society, one in every six deaths worldwide can be attributed to cancer, more than HIV/AIDS, tuberculosis, and malaria combined. While steady research progress has saved the lives of countless cancer patients—much work remains. Two cutting-edge, cancer researchers are challenging traditional research paradigms to better inform new therapies.
Translational medicine or “bench to bedside” is the near universal method for developing cancer treatments, but Padmanee Sharma, MD, PhD, a professor at The University of Texas MD Anderson Cancer Center is reversing this time-tested approach.
Instead of bringing newly devised treatments from the lab to patients enrolled in clinical trials, she is first bringing patients’ clinical data into the lab for researchers to study. “We’re collecting samples from patients in clinical trials, especially immunotherapy trials, and trying to understand how their immune system is evolving,” explained Dr. Sharma. “The immune response is a very dynamic process, which means that the anti-tumor immune response has been evolving and differentiating in some cases for years before a patient presents with a finding of cancer.”
A Focus on Immunotherapy
Padmanee Sharma, MD, PhD
“Although we have great mouse models, these models are not able to mimic the longitudinal and dynamic human immune response that develops over years,” she said. “The patient remains the best model.” With the patient’s clinical info, researchers try to understand the patient’s immune system and generate hypotheses that they think will help improve the patient’s treatment regimen.
Dr. Sharma’s research is focused on immunotherapy approaches which, “unleash the power of the immune system to reject cancer,” she explained. “Immunotherapy is my idea of precision medicine. Most people think of precision medicine as therapies against specific ’driver’ genetic mutations, which are mutations in the cancer cells that enable development and survival of cancer cells, but since cancer cells are constantly evolving and developing new mutations, it may be difficult to develop targeted treatments against each new mutation.”
“Immunotherapy is a match for cancer because it targets the immune system, not the cancer cells, and the immune response is constantly evolving in each patient’s body generating precise and specific T-cell responses against the mutations, regardless of whether the mutation is a ’driver’ or ’passenger’ mutation.”
“Immunotherapy can also be combined with other treatments such as surgery, radiation, chemotherapy, and targeted therapy because we can take advantage of the fact that these therapies are helping to kill some cancer cells, with subsequent recognition by the immune system, which can be enhanced with immunotherapy agents to drive additional anti-tumor responses as well as elicit development of memory immune responses to enable protection against cancer recurrence,” finished Dr. Sharma.
Tracking the Evolution of Tumors
Part of the need for Dr. Sharma’s approach stems from the complex cellular makeup of cancer, referred to as tumor heterogeneity. Within every patient’s tumor is an opportunity for Darwinian evolution, where specific cancer cell populations (subclones) are selected based on advantageous characteristics like metastatic ability, drug resistance, or immune escape.
Charles Swanton, FRCP, FRS, PhD
“This becomes a problem as the cell to cell variation, and clone to clone variation leads to variation in tumors, and is the ultimate challenge in developing effective cancer treatments,” said Charles Swanton, FRCP, FRS, PhD from The Francis Crick Institute. This is why there are few successful one-size-fits-all approaches to therapy in oncology.
Together with a team of leading researchers, Dr. Swanton spearheaded the TRACERx (TRAcking Cancer Evolution through therapy (Rx)) lung study, which hopes to transform our understanding of non-small cell lung cancer in particular and cancer in general by identifying the relationship between intratumoural heterogeneity in lung cancer tumors and poor clinical outcomes.
“Intratumoural heterogeneity is the difference in tumor subclones within the same patient, either within the primary site, between the primary metastatic sites, or between metastasis,” explained Dr. Swanton. “We’re trying to understand how a lethal metastatic subclone evolves from a heterogeneous primary tumor, and whether we can detect and monitor evolution in real time in patients’ blood to track evolution during the disease…And ultimately use all of that information to develop better diagnostic approaches, better clinical trial designs, and hopefully better therapies; ultimately, to control the disease for longer.”
Combining Lessons from Different Fields
With their powers combined, the approaches taken by Drs. Sharma and Swanton are critical for building a complete picture of the inner workings of cancer. Knowledge of the evolution and origins of different tumor clones will provide new targets to prime the host immune system, allowing it to destroy cancer cells and reduce the chances of disease recurrence.
In fact, work in this direction is already underway as Dr. Swanton is involved in setting up a company that will develop immune-based therapies targeting the mutations identified in the trunk of the tumour’s evolutionary tree—so-called—clonal mutations. Thus, as Dr. Sharma states “The new realm of cancer immunotherapies should be seen as one of hope for all patients.”
Often cited as the “4th Industrial Revolution” big data has the potential to transform health and healthcare by drawing medical conclusions from new and exciting sources such as electronic health records, genomic databases, and even credit card activity. In this podcast you will hear from tech, healthcare, and regulatory experts on potential paths forward that balance privacy and consumer protections while fostering innovations that could benefit everyone in our society.
This podcast was produced following a conference on this topic held in partnership between the NYU School of Medicine and The New York Academy of Sciences. It was made possible with support from Johnson & Johnson.
Mental illnesses present a major health, social, and economic burden and affected individuals experience disproportionately higher rates of both disability and mortality. In fact, the CDC reports that nearly 50% of U.S. adults will experience a mental illness at some point in their lifetime. And according to the WHO, depression alone accounts for 4.3% of the total disease burden worldwide and is the single greatest cause of disability. Yet despite enormous unmet need, efforts to develop new therapies for mental illness have stalled in part because of a need for more clarity surrounding the biological underpinnings of these diseases. On October 9, 2018, the New York Academy of Sciences presented Advances in the Neurobiology of Mental Illness. The one-day symposium, sponsored by Janssen Research & Development, LLC, brought together scientists, clinicians, and policymakers to discuss the genetics, molecular biology, and neurobiology of a wide range of mental illnesses. Topics included novel targets for treating depression, using genetic profiles to assess the risk of experiencing mental illness, and broader questions about battling the stigma surrounding such conditions.
Speakers
Hilary Blumberg, MD Yale School of Medicine
David Bredt, MD, PhD Janssen Neuroscience
Wayne Drevets, MD Janssen Research & Development, LLC
Steve Hyman, MD Broad Institute of MIT and Harvard
Jeff Lieberman, MD Columbia University
Eric Nestler, MD, PhD Icahn School of Medicine at Mount Sinai
Maria Oquendo, MD, PhD Perelman School of Medicine at the University of Pennsylvania
Murray B. Stein, MD, MPH University of California, San Diego
Event Sponsor
The Molecular Basis of Mental Disorders
Speakers
Hilary Blumberg, MD Yale School of Medicine
Steve Hyman, MD Broad Institute of MIT and Harvard
Eric Nestler, MD, PhD Icahn School of Medicine at Mount Sinai
Highlights
Early-life experience changes response to stress into adulthood by affecting the expression of key genes
In people with bipolar disorder, brain structure and activity change during adolescence and early adulthood.
Polygenic risk scores are a promising tool for gauging a person’s likelihood of developing a psychiatric disorder such as schizophrenia.
Transcriptional and Epigenetic Mechanisms of Depression
Techniques measuring how genes are transcribed — in animal models and human post-mortem tissue — are providing new and valuable insight into depression, and potentially, new therapies, said Eric Nestler of Icahn School of Medicine at Mount Sinai. His team uses such techniques to explore the idea that behavioral experience, such as early life stress, can produce permanent changes in the genome structure and gene expression of brain cells; these permanent changes in turn contribute to shifts in behavior for a lifetime and predispose a person towards susceptibility to stress.
In 2016, Nestler and his colleagues subjected mice to a form of chronic stress and conducted RNA sequencing in four different brain regions. The stress made about half the mice susceptible to developing behaviors associated with depression and anxiety, while the other half remained resilient to mental health effects. The resilient animals tended to have bigger changes in gene expression, suggesting that susceptibility may be caused by the brain’s inability to make the needed changes.
Stress during one of two early life periods results in susceptibility to stress in adulthood.
The researchers then conducted a similar gene expression study on post-mortem tissue of people who had depression. They found a surprising result: Gene expression changes observed in women overlapped very little with those seen in men, suggesting that the biological underpinnings of depression differ in men and women. Animal models showed the same sex difference. “That really argues for drug discovery processes that will look at both sexes independently,” Nestler said. What’s more, three different types of chronic stress dysregulated different sets of genes, with little overlap between them.
Early life stress is one of the strongest biological risk factors for depression. Most people can withstand that stress and develop normally into adulthood, but they retain an increased vulnerability to later stress. To understand the molecular mechanisms involved, Nestler’s team investigated how early life stress affects gene expression in mice. Most studies deliver early life stress continually over the first three weeks of life, but in this case, the researchers delivered early life stress over two time periods. Animals stressed during the second period, but not the first, show abnormal social behavior when stressed later in life. Gene expression studies in three different areas of the brain suggest that stress during the second early life period changes gene expression to look as though the animal has experienced chronic stress in adulthood — again, with the changing genes being different in males and females.
This pattern was strongest in one of the brain regions studied, called the ventral tegmental area (VTA), in male mice. The largest portion of those gene expression changes were regulated by a gene called Otx2. When they overexpressed that gene in the VTA of young male mice after the mice had experienced stress during the second early life period, the animals were protected from stress in adulthood. In turn, impairing Otx2 expression during that time increases stress susceptibility and dysregulates the stress-related genes irreversibly.
Otx2 is probably just one of several genes regulating susceptibility to stress, but it provides a model for how early life experience can alter stress response for a lifetime. The researchers are now studying what Nestler calls “chromatin scars” — chemical markers in the dysregulated genes.
The Brain in Bipolar Disorder
Elevated mood episodes are considered a hallmark of bipolar disorder, and these symptoms generally emerge during adolescence. But the condition is also characterized by more primitive and less widely-studied symptoms such as changes in sleep, circadian rhythms, and energy levels, said Hilary Blumberg of the Yale School of Medicine.
These features may emerge earlier than emotional disturbances, and researchers are beginning to look closely at how such symptoms might be therapeutically targeted. Early intervention could prevent the progression of bipolar disorder, said Blumberg — this is especially crucial because about 50% of people with bipolar disorder attempt suicide, and 15%–20% die by suicide.
Most research on bipolar disorder has focused on the circuitry of emotional regulation. Blumberg described two key components of this circuitry: The amygdala, an almond-shaped region deep in the brain that gets excessively activated in people with bipolar disorder; and the ventral prefrontal cortex, the frontal part of the most recently-evolved part of the brain, the cerebral cortex, where activation can be lower in people with bipolar disorder. These regions are highly interconnected.
Many factors, both environmental and genetic, can influence the development of brain differences in bipolar disorder.
Blumberg’s lab hypothesized that by adolescence, functional and structural changes might be detectable in the amygdala, which matures earlier. The frontal cortex develops later, so the researchers predicted that its structure and function would progressively diverge from normal during adolescence and young adulthood. Blumberg and her team conducted three types of brain scanning to image the structure and function of the two brain regions, as well as the connection between them, and observed these changes. They also found that differences in a specific part of the frontal cortex correlate with attempts to commit suicide, regardless of whether subjects were diagnosed with bipolar disorder or major depressive disorder.
Additionally, Blumberg and colleagues are investigating adults with bipolar disorder to better understand how the aging process interacts with psychiatric conditions. Older adults often have a higher suicide risk; little research has focused on this developmental stage, but there is evidence that lithium may be effective in reducing suicide risk. They are also using brain imaging to explore the effects of genes thought to play a role in bipolar disorder, and identifying the effects of early life stressors, such as physical or emotional abuse or neglect, on brain structure and function in adolescence.
The group developed a behavioral therapy called BE-SMART that focuses on helping people with bipolar disorder improve their emotional regulation, and regularize their sleep and daily rhythms. Preliminary imaging studies show that after undergoing the therapy, patients have less activation in their amygdala and more in their frontal cortex. “In addition to pharmacological treatments, there are many other strategies that may help improve brain circuitry trajectories,” Blumberg said.
A New Molecular Map for Mental Disorders
In the 1960s, geneticists realized that psychiatric disorders were complex, but early researchers estimated that some 20 genes might underlie these conditions. Today, researchers are realizing that many thousands of variants in many hundreds of genes are involved, said Steve Hyman of the Broad Institute of MIT and Harvard. That underestimation may in part explain why only a handful of drug treatments exist for patients with these diseases — almost all of them discovered by chance. The field desperately needs new tools to identify molecular mechanisms that can be targeted with drugs, as well as biomarkers to help researchers identify which patients might respond to a therapy and which might not. Evolving genetic technologies provide those tools, Hyman explained.
Psychiatric diseases such as schizophrenia and bipolar disorder have a heritably of up to 80%; depression has a lower, but still strong, genetic component as well. However, while some diseases are caused by mutations in a single gene, these diseases tend to be driven by variants of many genes, with no single gene playing an outsized role. Humans have been evolving for about 200,000 years and share many common gene variants. Gene chips can scan up to one million locations in the genome to identify common variants for a given phenotype — whether it be a feature such as height or a disease like schizophrenia.
In schizophrenia, for example, some 280 spots in the genome carry variants that can each nudge a person towards or away from the disease. Researchers can calculate approximately how much risk each gene confers. One recently developed metric called the polygenic risk score combines the weighted contribution of each of these risk genes for a given individual and compares them to a baseline to estimate the probability that the person will develop the disease. This score is the first objective tool for determining whether someone might be a good candidate for a clinical trial. “It will just get better as the genetics advance,” said Hyman.
Most genetic samples come from people of European ancestry.
One problem with polygenic risk scores is that they are only as good as the population genetics data they are based upon. Most data come from white Europeans, so small deviations from the norm in that population are statistically detectable. But the collection of gene variants underlying a disease such as schizophrenia is likely to differ in people from Asia, Sub-Saharan Africa, and Latin and South America, so the polygenic risk scores of patients from these backgrounds are currently much less accurate. Geneticists are beginning to amass more diverse data, but much work on this front remains.
Genetic analyses of common variants are beginning to yield cellular and molecular clues about schizophrenia. Risk genes are not all expressed in all cell types in the body, and analyzing variants in individual cells may reveal which cell types are most affected in the disease. Early work from another team at Hyman’s institute has found that more risk genes are expressed in a cell type called pyramidal neurons in the brain’s cortex. As the technology improves, researchers hope to develop a cellular map of disease risk. Researchers can then use stem cell technologies to make different types of neurons and study how the disease affects them. “There are many years of work ahead of us,” said Hyman, “but I think we finally have a toe-hold.”
Wayne Drevets, MD Janssen Research & Development, LLC
Maria Oquendo, MD, PhD Perelman School of Medicine at the University of Pennsylvania
Murray B. Stein, MD, MPH University of California, San Diego
Highlights
Immune system molecules offer a promising target for novel depression therapies likely to help a subset of patients.
Drugs already approved for other psychiatric disorders may be effective treatments for post-traumatic stress disorder.
Studies point to at least two different phenotypes of suicidal behavior.
Neuroimmune Mechanisms as Potential Therapeutic Targets for Depression
Researchers know little about the underlying biology of mood disorders, so there is little to guide the field toward new treatments and biomarkers, said Wayne Drevets of Janssen Research & Development. However, emerging research suggests that some of the most reliable blood-based biomarkers for depression include immune molecules associated with low-grade inflammation, such as interleukin 6 (IL6), and proteins that react to inflammation, such as C-Reactive Protein (CRP).
Accumulating evidence points to Interleukin 6 as a promising target for treating depression.
Studies suggest that immune mechanisms play a role in roughly 33%–50% of patients with mood disorders, and that the adaptive immune system functions deficiently in depression. In a small subset of patients, autoantibodies to certain brain receptors and channels have been implicated in mood disorders. This suggests that at least some people with such conditions would benefit from therapeutics that target immunological mechanisms.
Several pharmaceutical companies formed a collaboration to explore this possibility (although currently, only Janssen and Glaxo SmithKline remain). Microarray data pointed to IL6 as a promising therapeutic target; IL6 levels remain high in people who do not respond to depression treatment and correlate with suicidality measures. They also predicted onset and severity of depression in children of parents with bipolar disorder. In animal models, antibodies against IL6 prevented depression symptoms in animals that experience a stressor.
The pharmaceutical company consortium pooled data from all trials to date and identified 18 trials that had drug targets and diseases with a prominent inflammatory component. Two of the tested drugs were Sirukumab and Siltuximab, Janssen compounds that target IL6. They then launched a double-blind placebo-controlled trial of Sirukumab as an adjuvant therapy in patients taking an antidepressant. The effects were not significant at 12 weeks, and a heightened infection rate in subjects suggested the need for a safer antibody or small molecule. However, additional analyses were encouraging. They showed that the antibody worked as intended, decreasing IL6 levels at the target, that the therapy did work in people with high CRP levels, and that a different, more sensitive depression measure hints that the treatment may work. “We do think this might be an important learning for future trials,” Drevets said.
It has long been unclear whether immunological therapies must work in the central nervous system or in the periphery to have an effect. To find out, the pharmaceutical company consortium is currently conducting a clinical trial of a small molecule that interferes with an ion channel called P2X7. The channel is expressed on the surface of brain cells called microglia and is activated by molecules produced by stress or inflammation. P2X7 activation causes depression-like behavior in animal models through the release of another interleukin called IL1-beta. Blocking the channel might therefore prevent stress-mediated IL-1beta release. If the small molecule works, Drevets said, it would validate the pursuit of central nervous system targets.
Neurobiology and Pharmacotherapy of Post-traumatic Stress Disorder
Although environmental factors often play a role in psychiatric disorders, post-traumatic stress disorder (PTSD) is the only psychiatric disorder that by definition involves exposure to a traumatic, life-threatening event, explained Murray Stein, from the University of California, San Diego. PTSD has four core features, but researchers calculate that there are more than 600,000 combinations of symptoms that can produce the disorder, and it often co-occurs with other conditions such as major depression and chronic pain.
Risk factors for PTSD vary widely.
Around 3% of people worldwide and 7% in the U.S. have the condition, but prevalence varies enormously by population. Women have PTSD at twice the rate of men, in part because of the types of trauma they tend to experience, and the rate for Native Americans living on reservations is 2–3 times that of the U.S. at large. Meanwhile, 30% of Vietnam veterans have the condition. Despite great unmet need, very few drugs exist to treat PTSD and none have been approved since 1999. However, certain psychotherapies do seem to help.
The lack of drug treatments may be partly due to a poor understanding of what causes the condition. Brain imaging studies suggest circuits involving emotional regulation, executive function, and threat detection is out of whack. Studies of soldiers deployed to Afghanistan and patients admitted to an emergency room have shown that traumatic brain injury sharply raises the risk of PTSD. Stein and colleagues recently showed in a small study that a drug called methylphenidate helps improve focus and alleviate hyperarousal in people with PTSD.
Using genome-wide association studies, researchers are beginning to identify genes associated with the disorder. Stein’s team led one such study, called ARMY STARRS, which found that a variant in a gene called ANKRD55 was associated with PTSD in African Americans. The gene’s function is unknown, but it is linked to multiple autoimmune and inflammatory disorders. He and others are collaborating with a large biobank called the Million Veterans Program in which DNA and survey results can be analyzed along with electronic health records. They identified a link between PTSD severity and the gene coding for corticotropin-releasing hormone receptor 1, which has already been associated with the disorder in other studies.
Finally, Stein noted that a few drug studies targeting dopamine receptors have shown promise, despite the fact that different studies have shown conflicting results. That could be because the effects of the drugs are uneven across PTSD symptoms, and therefore their benefits don’t register with the assessment tools used. Overall, he said, drug trials for PTSD have been limited, but combining genetics and bioinformatics may point to both new drugs and old drugs that deserve a second look.
Subtyping Suicidal Behavior: a Blueprint for the Development of Biomarkers
Maria Oquendo from the University of Pennsylvania described her work defining two distinct subtypes of suicidality. Suicide is a major epidemic, and identifying triggers and risk factors will help prevent deaths, she said.
The suicide rate varies widely between countries around the world, but overall, more people die by suicide (44,000 per year) than by automobile accidents (33,000). In the U.S., suicide has been on the rise since 1999. Some 5%–15% of the U.S. population experiences suicidal thoughts, and that number is thought to be much higher in adolescents. About four women attempt suicide for every one man; about three men for every one woman succeed.
Although nine out of 10 people who die by suicide have a psychiatric disorder, most people with a psychiatric disorder never attempt suicide — suggesting it is not enough to spur suicidality. Based on this observation, in 1999 Oquendo’s group proposed that some individuals are predisposed or pushed toward suicidality by behavioral factors such as aggression and impulsivity; mental factors such as cognitive inflexibility; biological factors such as dysregulated serotonin levels; or substance and alcohol abuse.
Oquendo’s lab proposed two distinct phenotypes of suicidal behavior.
In 2004, they interviewed about 300 people with depression three months, 12 months, and 24 months after an initial evaluation. High levels of either aggression and impulsivity or pessimism greatly increased the risk of a suicide attempt, supporting their model. In a later study of 415 people with depression, 27% of participants had borderline personality disorder (BPD), so the researchers analyzed them separately. In people without BPD, both major depressive events and stressors such as health, work, and family events precipitated suicidality. However, in those with BPD, life stressors did not seem to contribute — perhaps because people with BPD experience life stressors in a way not captured by the study.
Nonetheless, the results suggest at least two independent pathways to suicidality. Oquendo and her colleagues hypothesized that one type of suicide attempter, who often has experienced childhood abuse, now struggles to regulate their emotions, reacts aggressively to threats or frustration, and has higher levels of cortisol and other biological stress markers. In such a person, life stressors would provoke suicidal thoughts, and they would attempt suicide impulsively. Another type of suicide attempter is someone tormented by recurring suicidal thoughts. Such a person is not impulsive or aggressive and has good cognitive control, but might attempt suicide in the context of a depressive episode.
Accumulating data supports the existence of these two suicidality subtypes. For example, people with high reactive aggression who were abused as children show sharp and frequent spikes in suicidal thoughts, often in response to seemingly minor life stressors; while people with low reactive aggression and impulsivity, have more stable levels of suicidality. Those with high aggression and impulsivity also have a spike in cortisol levels in response to a social stress test in the lab. And people with BPD who had attempted suicide seemed less able to engage brain regions involved in decision-making and perspective, suggesting a difference in their emotional regulation. There are some hints that differences in serotonin receptor levels may be at play in these two groups.
Oquendo believes there may be at least three other subtypes of suicidality, and her lab is trying to identify them in a study that follows patients with depression over a two-year period. Ultimately, the aim is to identify clear biomarkers for all suicidality subtypes.
Stigma surrounding mental illness is alive and well, but eliminating it would revolutionize mental health care.
Imagine There Was No Stigma of Mental Illness
Suppose you had to give a toast for your boss at work one day, but you couldn’t make it because you were ill. Would you rather tell your colleagues you had a kidney stone, or that you were feeling suicidal? Jeff Lieberman of Columbia University opened his talk with this hypothetical scenario to illustrate that mental illness is still highly stigmatized.
Much of this stigma is driven by a decades-old skepticism and assault on the legitimacy of psychiatry, which came to a zenith when a doctor named Thomas Szasz — who wrote a book called the Myth of Mental Illness — joined forces with L. Ron Hubbard, inventor of an applied philosophy called Dianetics. The resulting belief system, Scientology, remains deeply opposed o psychiatry. The stigma of mental illness has real consequences — it is a serious deterrent to individuals seeking mental health care and has contributed a dysfunctional mental health delivery framework.
It also drives a funding disparity for mental health research. “If you do the math, 0.06% of the federal budget is spent on biomedical research that could advance our ability to understand and treat mental disorders and addiction,” Lieberman said — much less than for cancer, infectious disease, and cardiovascular disease. Because of that funding and attention, biomedical advances for these diseases made over the past several decades have led to effective treatments. Meanwhile, the World Bank estimates that by 2030, depression will be the most costly disease globally.
Medicine became a scientifically grounded endeavor in the 19th century and psychiatry formed one of he first professional organizations, now called the American Psychiatric Association (APA). At the time, the available tools limited progress in psychiatric research, and treatment for patients was often barbaric.
Psychiatry as a whole embraced Freud, and tried to apply his ideas to the broader population, despite the fact that they were irrelevant to specific illnesses such as schizophrenia and autism. “Theories were postulated that were preposterous and venal,” said Lieberman, such as that of the “refrigerator mother,” and overbearing parents as a cause of homosexuality, or orgone theory. By the 1950s and 1960s, when the number of patients in mental hospitals across the U.S. swelled to 550,000, the conditions under which most asylum patient lived were horrendous.
The turning point in the field’s validity came in the 1970s, when Columbia University psychiatrist Robert Spitzer was appointed chair of the APA’s task force to release the third edition of the Diagnostic and Statistical Manual of Mental Disorders (better known as the DSM, currently in its fifth edition). Although next to nothing was known about the biological basis of mental illness, he took a rigorous methodological approach, eliminating homosexuality as a diagnosis and describing post-traumatic stress disorder. The decades leading up to the 1980s were a scientific revolution of sorts, with the serendipitous discovery of psychotropic drugs and adoption of diagnostic methods. Today, it is a field wholly invested in scientifically driven methodology — the era of psychiatric neuroscience, Lieberman said.
It’s certainly possible to imagine eradicating the stigma surrounding mental illness — one stigmatized illness that succeeded in creating such a change is HIV. Without stigma holding back the field, and the institution of a health care system that provides mental health care from a public health standpoint, the results could be miraculous, Lieberman said. The system could target three distinct populations — the worried well, people with mild mental disorders such as anxiety and obsessive-compulsive disorder, and the severe mentally ill population — and offer them a variety of different avenues to care.
Jeffrey A. Lieberman and Ogi Ogas. Back Bay Books, 2016.
Panel Discussion
Speakers
Hilary Blumberg, MD Yale School of Medicine
Steve Hyman, MD Broad Institute of MIT and Harvard
Jeff Lieberman, MD Columbia University
Maria Oquendo, MD, PhD Perelman School of Medicine at the University of Pennsylvania
David Bredt, MD, PhD (Moderator) Janssen Neuroscience
Highlights
Complex chemistry and complex genetics are just two of the many challenges to developing drug therapies for mental illness.
There is conflicting data about whether people with bipolar depression should be treated with antidepressants.
The relationship between circadian rhythms and psychiatric disorders is poorly understood, but normalizing people’s sleep schedules may have therapeutic value.
The panel began by discussing the challenges in developing therapeutics for mental illness. Even in cases where the drug target is clear, the chemistry can be extremely challenging, said Hyman. There is also the issue of making sure the drug can be absorbed orally and then can cross the blood brain barrier. Also, he noted, psychiatric disorders are genetically very complex, and unlike cancers where researchers can identify a driver mutation to target with a precision therapy, many genes affected in psychiatric disorders converge on the same pathways.
On the other hand, said Oquendo, psychiatric illnesses have an advantage over cancer therapeutically, in that behavioral modulations can greatly help patients and can affect the underlying disease. In this field, she said, “there are many synergistic ways to skin a cat.”
In response to a question from the audience, Oquendo and Blumberg discussed the pros and cons of antidepressants for people with bipolar disorder. For a subset of patients, antidepressants might aggravate the condition, leading to a worse prognosis, Blumberg explained. Yet, if someone presents with depression, it is not always possible to determine whether they have major depressive disorder or bipolar disorder.
However, she noted, the literature is rife with conflicting data on whether antidepressants do in fact worsen the disease. Oquendo, meanwhile, said that the fear of giving bipolar patients antidepressants might actually have caused a good deal of suffering, and even suicides. In her experience, bipolar patients often strongly objected to being taken off antidepressants, and while epidemiologic and other studies don’t prove that antidepressants help, it’s not clear that they cause harm, either.
The panelists also discussed the role of circadian rhythms and sleep in bipolar disorder and other conditions. So far, chronobiological features have not been integral to the understanding of these diseases, but they may play a real role in their pathophysiology, said Lieberman. Researchers have long known that sleep deprivation can bring on a manic state, Blumberg noted, and shifting the sleep schedules of young adults with bipolar disorder often results in improvements to their condition. Another attractive dimension of targeting sleep and circadian rhythms, said Blumberg, is that “it’s a ‘do no harm’ intervention.”
Panel Discussion
Open Questions
How exactly does early life stress lead to behavioral changes in adulthood?
Can basic functions like sleep, daily rhythms, and energy levels serve as an early biomarker for bipolar disorder?
Can polygenic risk scores accurately stratify patients in clinical trials?
How should researchers design trials to test therapies that target immune molecules to treat depression?
How can genetics and bioinformatics data be combined to help identify new and repurposed drugs for PTSD?
How can researchers use accumulating knowledge on subtypes of suicidal behavior to develop effective interventions?
What can be done to eliminate the stigma of mental illness?
Phagocytes are cells best known for their role as immune cells that fight infection. However, recent research has identified broader functions for these cells in major human diseases.
Published November 29, 2018
By Andre Legaspi
Miriam Merad, MD, PhD is an eminent oncologist and immunologist. Her research combines laboratory studies of phagocytes with a patient-focused perspective to develop new cancer treatments.
What will be the biggest advance in cancer treatment over the next five years?
The landscape of care will be dramatically different in the next five years. It’s an exciting time for researchers, but more so for patients. We’re going to see the development of completely new cancer regimens where chemotherapy regimens will be revised to reduce suppressive activity, and combined with novel immunotherapy and likely also targeted therapies.
Why did you study the biology of phagocytes?
Miriam Merad, MD, PhD
During my residency in Hem/Onc I rotated in the allogenic bone marrow transplantation (BMT) unit and witnessed the power of allogeneic BMT to cure patients with leukemia and severe lymphoma which really represent the first success of cancer immunotherapy. The success of BMT convinced me of the potential of immunotherapy to treat cancer. Later during my residency, I met a now very famous cancer immunologist Laurence Zitvogel. She was using phagocytes as vaccines against cancer. As a resident with little time to do research, I became fascinated by these cells and their potential to instruct cancer immunity and this is why I decided to spend my PhD studying these cells.
Why are phagocytes such a promising target for cancer treatments?
Immunologists have successfully used vaccination to induce anti-tumor immunity, but these successes were very limited. Recently, checkpoint blockade therapy which enhance anti-tumor T cells have had significant clinical success even in tumors that have traditionally not responded to conventional treatment. Now T cells cannot kill a cancer without being instructed to do so. Phagocytes are uniquely able to instruct T cells to kill or not to kill — this enhances phagocytes function and can strongly enhance anti-tumor immunity.
What advice would you give young researchers?
Researchers in the biological sciences should study patients more. We have much to learn from patient lesions and need to bring this knowledge to the lab. In my lab, researchers are encouraged to start with the patient and then decide whether a prominent model is best for attacking the question they want to answer. This is not to say that we need to get rid of the model system. That would be a disaster. Instead, researchers should constantly be revising current models. We should not be working on the same models that our mentors have been using and should constantly improve them based on the knowledge gained from patients.


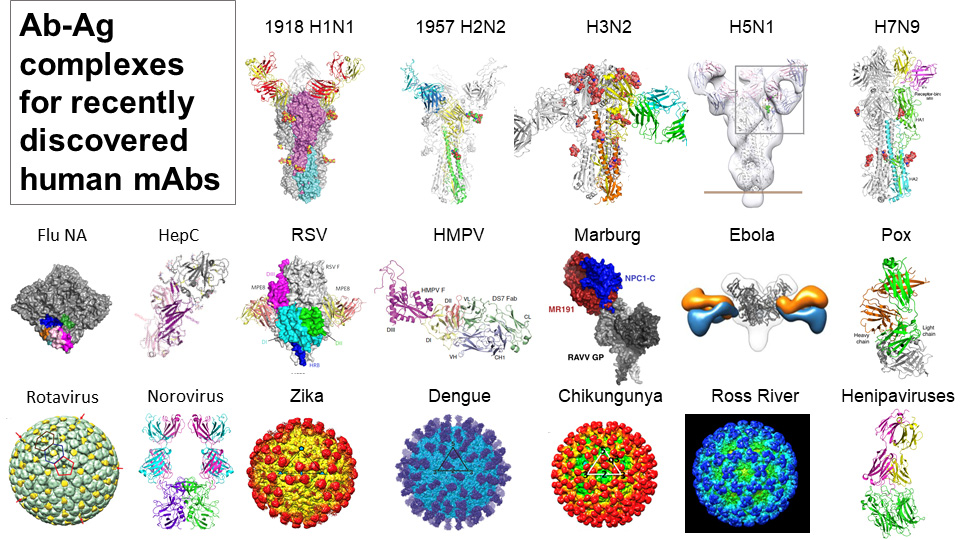
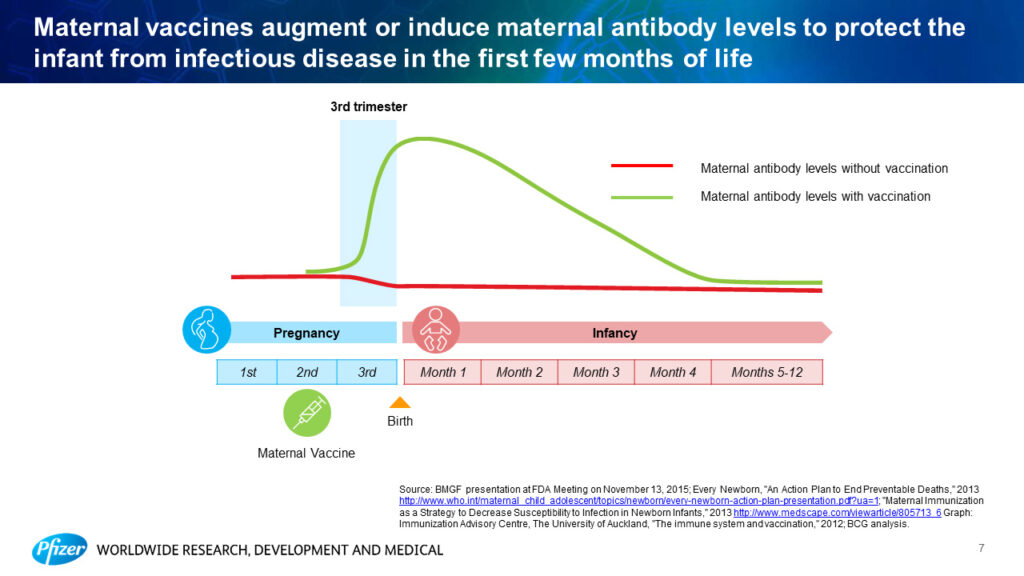
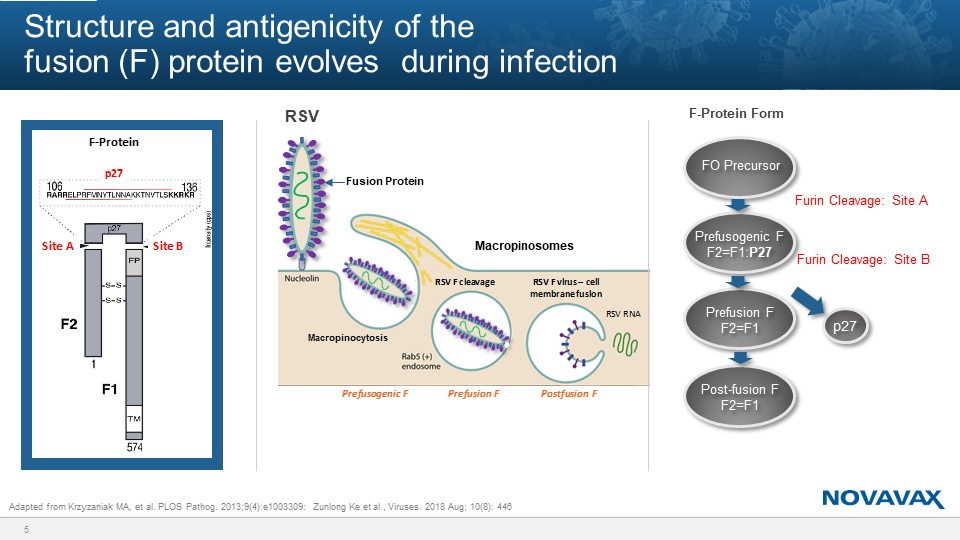
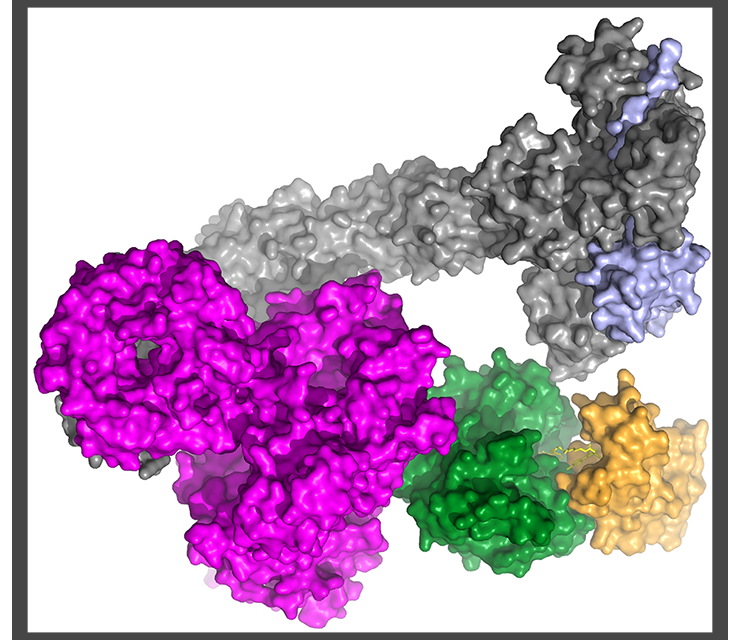
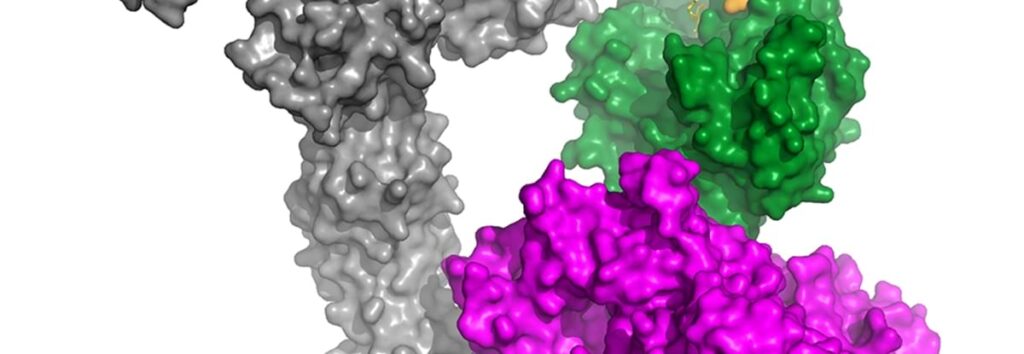














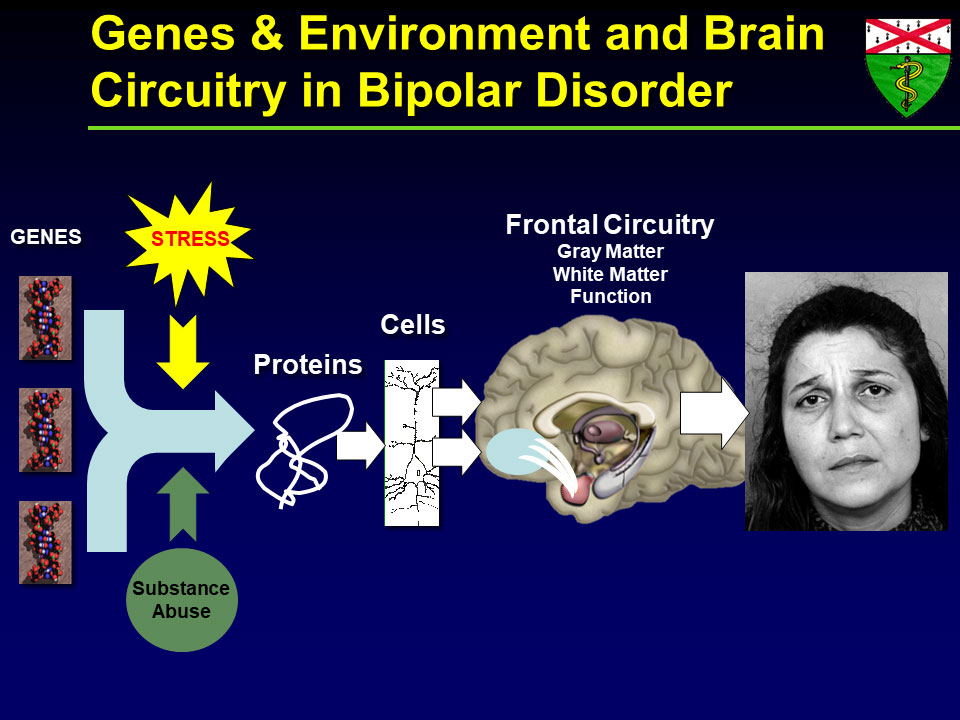
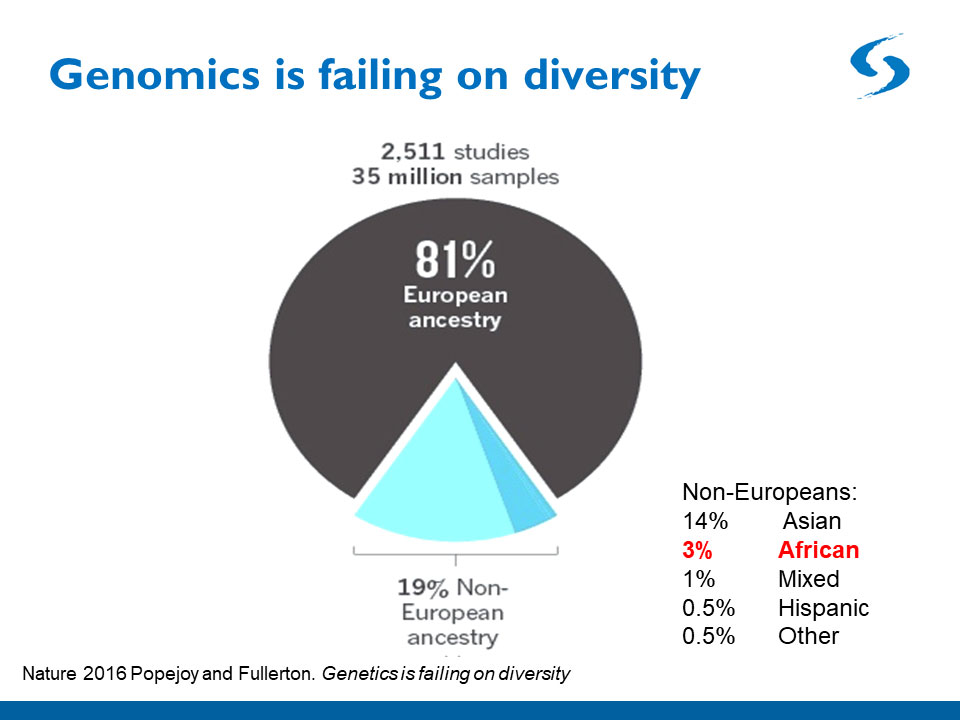


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}