Vijay Sankaran, MD, PhD, discusses recent developments in the treatment of sickle cell disease and other blood disorders, with a specific focus on gene targeting.
Published August 16, 2017
By Marie Gentile and Robert Birchard
Microscopic view of sicke cells causing anemia disease.
In 1973 the lifespan of a person with sickle cell disease (SCD) in the United States was 14 years. Today, the lifespan of a person with SCD has increased to 40-60 years. While diagnosis and care for people with SCD has improved, treatment options remain limited. In fact, before the recent approval of Endari there was only one FDA approved treatment for SCD, an inherited red blood cell disorder where red blood cells become rigid and sickle shaped impeding the flow of blood and oxygen through the body’s blood vessels.
Still, insights into the pathophysiology of SCD and other blood disorders has led to promising new treatment approaches. At the forefront of this research is Dr. Vijay Sankaran an Assistant Professor of Pediatrics at Harvard Medical School and Attending Physician in Hematology/Oncology at Boston Children’s Hospital and the Dana-Farber Cancer Institute.
Dr. Sankaran’s research into inherited blood disorders was inspired by his initial work in understanding the mechanisms behind fetal hemoglobin regulation. During gestation the fetus expresses a form of hemoglobin that helps extract oxygen from the mother. After birth this mechanism is silenced and fetal hemoglobin is no longer produced. People with SCD could benefit greatly from the continued production of the fetal form of hemoglobin.
Research on the SH2B3 Gene
“We knew that patients with a number of inherited blood disorders such as SCD and beta-thalassemia can actually do much better if they have higher levels of fetal hemoglobin. There were clear indications that inducing fetal hemoglobin could be effective, but we lacked the tools to reactivate fetal hemoglobin in adults,” he explained. This line of research eventually led Dr. Sankaran to identify and demonstrate that the BCL11A gene is a potential therapeutic target. BCL11A could be induced to produce fetal hemoglobin, which would produce healthier red blood cells and fewer sickled cells.
Related to Dr. Sankaran’s research into activating the BCL11A gene in adults is his research into the regulation of blood production more generally. For example, work from his group has shown that shutting down the SH2B3 gene which, “normally functions as a break on red blood cell production,” could be valuable for, “applications where people are interested in trying to produce blood cells outside of the body for transfusion or other purposes.”
If the SH2B3 gene “break” was removed more healthy red blood cells could be produced. This is tremendously important for people with SCD because, “Many of them cannot tolerate the blood from most donors, because they have developed antibodies against the donor’s blood antigens.” His research on the SH2B3 gene could lead to less expensive and more widely available methods for manufacturing red blood cells.
Take Risks and Find Multiple Mentors
Dr. Vijay Sankaran
The cost and time associated with the research and development of new treatments is immense and the length of the development pipeline represents a significant clinical challenge. As an example, Dr. Sankaran noted how the development of Endari began three to four decades ago. But, he believes these challenges can be overcome, “Using insights from human genetics and natural observation, can help in the development of new treatments for SCD. For many years it was unclear what clinical endpoints would be ideal to go after in SCD. There are many manifestations, but the more candidate therapeutics we identify, and the more clinical trials we perform, we can better learn how to measure the effect of these endpoints.”
Finally Dr. Sankaran offered some advice to future researchers, “I think the key is to not be afraid to take risks. It’s critical to find not just a single mentor, but many mentors to help shape your career. Find and talk to a number of mentors who can help guide you. Sometimes it’s very easy to lose focus in an area. I was very lucky as a graduate student to work with Stuart Orkin, who allowed me to take some risks and pursue research into fetal hemoglobin,” he said.
“I then continued this research as a post-doctoral fellow with Eric Lander at the Broad Institute and Harvey Lodish at the Whitehead Institute, while David Nathan and Sam Lux – among others – at Boston Children’s have helped me to develop as a clinician as well to make sure the work we pursue in the lab relates to the patients I care for.”
Two publications from The New York Academy of Sciences examine pre-approval access to investigational drugs from a range of stakeholders and perspectives.
Under expanded access (also called compassionate use), patients who suffer from serious or immediately life-threatening diseases for whom no comparable or satisfactory alternative therapy is available can access drugs and medical devices that are not approved by the FDA and are currently being tested in clinical trials. A total of 29 states have also passed “right-to-try” laws allowing terminally ill patients to access experimental therapies, but there are many questions about the safety and efficacy of such treatments that are not FDA-approved.
Recently the FDA announced significant changes to shorten and simplify the application process used by physicians to request expanded access to investigational drugs for individual patients. Some are predicting that the FDA may not approve a drug to treat Duchenne muscular dystrophy that is currently under review, but will allow compassionate use while additional studies are conducted.
Regardless of the FDA decision, the debate over compassionate use will continue and evolve as additional treatments are brought to the forefront of experimental medicine and research.
June 2, 2016 Patients with life-threatening illnesses face challenges in accessing potential therapies at the cutting-edge of R&D which have not yet been proven in a clinical trial. This podcast will explore the provocative and emotional stories of patients, family members, advocates, researchers, physicians, and the regulators charged with keeping medicines in the marketplace safe and effective.
Biotechnology and nanotechnology have given rise to a growing number of innovator-driven complex drug products and their copy versions. Biologics exemplify one category of complex drugs, but there also exist non-biological complex drug products (NBCDs), including many nanomedicines such as iron-carbohydrate complexes, several drug carrying liposomes or emulsions, and glatiramoids. These products are difficult to characterize—often the key features for efficacy and safety are not well understood. These factors pose unique challenges for pharmaceutical companies and regulatory agencies when comparing generic complex drugs to their branded counterparts.
On November 9, 2016, representatives from academia, industry, and regulatory agencies convened at the New York Academy of Sciences for the symposium Equivalence of Complex Drug Products: Scientific and Regulatory Challenges, an opportunity to discuss how to approach complex generics. Regulatory officials described how agencies approach evaluating complex generics for marketing approval, while industry speakers presented several examples that demonstrate the difficulties in characterizing complex drugs.
The symposium was presented by the Non Biological Complex Drugs Working Group, the Nanotechnology Characterization Laboratory, and the New York Academy of Sciences.
Lawrence Mayer, senior vice president of discovery at Jazz Pharmaceuticals, has played a lead role in the discovery and development of a number of oncology drugs, several of which eventually achieved market approval. He has also held senior management positions at The Canadian Liposome Company and QLT, Inc. before joining the British Columbia (BC) Cancer Agency, where he established and directed the Health Canada-accredited Investigational Drug Program. Celator Pharmaceuticals, now a subsidiary of Jazz Pharmaceuticals, was formed in 2000 as a spin-out of Mayer’s laboratory at the BC Cancer Agency. Mayer has authored more than 250 scientific publications and has more than 35 patent families awarded or pending. Mayer received his BS in both chemistry and biology, summa cum laude, from Wartburg College and his PhD in biochemistry from the University of Minnesota.
Daan Crommelin is professor emeritus at the Department of Pharmaceutics at Utrecht University. Until December 2011 he was scientific director of the Dutch Top Institute Pharma in Leiden. He is adjunct professor at the Department of Pharmaceutics and Pharmaceutical Chemistry at the University of Utah. Crommelin is co-founder of OctoPlus, a Leiden based company specialized in the development of pharmaceutical (mainly protein based) product formulations and advanced drug delivery systems. He published extensively and is on the editorial board of 10 peer reviewed journals in the pharmaceutical sciences. He is Editor-in-Chief of the AAPS book series Advances in the Pharmaceutical Sciences. He advises venture capital groups and acts as consultant. He chairs the UCAB Foundation: the Utrecht Center of Excellence for Affordable Biotherapeutics, a WHO supported initiative. He chaired the Board of Pharmaceutical Sciences of the International Pharmaceutical Federation (F.I.P.), was chair of the organizing committee of the Pharmaceutical Sciences World Conference 2007 in Amsterdam. He is past president of the European Federation of Pharmaceutical Sciences (EUFEPS) and past vice-chair of the scientific advisory board of the European Innovative Medicines Initiative (IMI).
A pharmacist by training, Beat Flühmann holds a PhD in molecular biology. In his current position Flühmann serves as global lead on non-biological complex drugs at Vifor Pharma Ltd Switzerland, with a main interest in regulatory aspects of nanomedicines. Previously, Flühmann led a global multidisciplinary research and development team at Roche/DSM nutritional products developing novel compounds for the prevention and treatment of diabetes. He also is a steering committee member of the Non-Biological Complex Drugs Working Group hosted at the nonprofit Lygature, a group set up to discuss science-based approval and post-approval standards to ensure patient safety and benefit with non-biological complex drugs. The working group engages in activities to publish and discus scientific evidence with authorities, experts, health care providers, and is involved in scientific education and training to relevant stakeholders. Flühmann also sits on the advisory board of the GoNanoBioMat project, a multinational research project in the field of nanomedicine.
Joseph L. Glajch is director of analytical development at Momenta Pharmaceuticals. He received his AB in chemistry at Cornell University and PhD in analytical chemistry at the University of Georgia under L.B. (Buck) Rogers. He has held technical and R&D management positions at DuPont, Bristol-Myers Squibb, Certus, and Momenta, with an emphasis on HPLC column and method development and pharmaceutical development and analysis. He has served as president and program chairman of the Analytical Division of the American Chemical Society and the Chromatography Forum of the Delaware Valley, as well as program chair of the Gordon Conference on Analytical Chemistry. He has served on the editorial advisory boards of Analytical Chemistry, the Journal of Chromatography, and LC/GC. He is a member of the USP Expert Committee on General Chemical Analysis and has over 40 publications, is co-author of three books, and holds six patents on HPLC column materials and medical imaging agents.
Elwyn Griffiths, PhD, DSc
World Health Organization and Health Canada publications
Elwyn Griffiths is currently a consultant in vaccines and biotherapeutics to WHO and a member of the WHO Expert Committee on Biological Standardization. He is also a member of the Clinical Trials, Biologicals and Vaccines Expert Advisory Group of the UK Commission on Human Medicines and of the Expert Advisory Group on Biological and Biotechnology products of the British Pharmacopoeia Commission.
In 2011, Griffiths retired as director general, biologics and genetic therapies directorate of Health Canada, an organization he joined in 2003 upon retirement from the World Health Organization. Griffthis holds a PhD and a DSc degree from the University of Wales. In 1980, he became a senior member of staff at the UK National Institute for Biological Standards and Control, and in 1994 was appointed chief of biologicals at WHO. From 1994 until the end of 2002, Griffiths was responsible for WHO’s program for providing international written and physical standards for vaccines, blood products and biotherapeutics.
Iris Grossman, VP, global head of the Personalized & Predictive Medicine (PPM) and Big Data Analytics unit for Teva Global R&D, is currently charged with defining and implementing Teva’s global PMP strategy, covering both discovery and development R&D programs. Israel’s leading financial magazine, Globes Magazine, selected Grossman as one of the country’s top 40 professionals under 40 years of age in 2013.
Prior to joining Teva, Grossman was CEO and president of the pharmacogenetics management consultancy IsraGene Ltd.. This followed several years of spearheading pipeline pharmacogenetic programs for industry and academia as director of pharmacogenetics at Cabernet Pharmaceuticals Inc. Grossman moved into consultancy having been responsible for running large-scale pharmacogenetic programs at GlaxoSmithKline, with an emphasis on infectious and neurological diseases.
Grossman received her PhD from the Technion–Israel Institute of Technology, where her research project, conducted in collaboration with the Weizmann Institute for Science, investigated pharmacogenetic markers of multiple sclerosis treatment response.
Wenlei Jiang, PhD
Office of Research and Standards, Office of Generic Drugs, US Food and Drug Administration website | publications
Wenlei Jiang is currently a senior science advisor in the Office of Research and Standards (ORS)/Office of Generic Drugs (OGD)/Center for Drug Evaluation and Research (CDER). She is mainly responsible for coordinating post-market generic drug safety investigation, representing ORS on OGD’s new international harmonization activities, and developing opportunities for scientific outreach. Previously, she served as the acting deputy director of ORS, where she provided oversight on Generic Drug User Fee Act (GDUFA) regulatory science research programs. She used to work in the Division of Chemistry, OGD to review the chemistry and manufacturing control (CMC) sections of ANDAs. Prior to joining FDA, she was at Novartis Pharmaceutical Corporation where her responsibilities included formulation development of conventional liquid and solid dosage forms, as well as advanced parenteral drug delivery systems. She received her PhD in pharmaceutics and pharmaceutical chemistry from Ohio State University in 2001.
Scott McNeil serves as director of the Nanotechnology Characterization Laboratory (NCL) for Leidos Biomedical Research and Frederick National Laboratory for Cancer Research, where he coordinates preclinical characterization of nanotech cancer therapeutics and diagnostics. At the NCL, McNeil leads a team of scientists responsible for testing candidate nanotech drugs and diagnostics, evaluating safety and efficacy, and assisting with product development. McNeil is a member of several working groups on nanomedicine, environmental health and safety, and other nanotechnology issues. He is an invited speaker to numerous nanotechnology-related conferences and has several patents pending related to nanotechnology and biotechnology. He is also a vice president at Leidos Biomedical Research.
McNeil’s professional career includes tenure as an Army officer, with tours as chief of biochemistry at Tripler Army Medical Center, and as a combat arms officer during the Gulf War. He received his bachelor’s degree in chemistry from Portland State University and his doctorate in cell biology from Oregon Health Sciences University.
Kouros Motamed, PhD has been the Director of Drug Development at NantBioScience, Inc. since April 2016. Prior to that, he has served as VP of Strategic Alliances and Clinical Communications and VP of Clinical Development and Nanomedicine at Sorrento Therapeutics from 2013 to 2016. He has also served as a co-founder and CSO/CTO of Igdrasol, Inc. and Biomiga Diagnostics start-up companies from 2011–2013. Dr. Motamed has also served as the MOA and Molecular Biology Group Head at Celgene Corp. and Abraxis BioScience Inc. from 2007–2011. Dr. Motamed held an Assistant Professorship position in the Department of Pathology and Vascular Biology Center at Georgia Health Sciences University from 2002–2007. He has over 30 original publications in peer-reviewed journals, over 50 conference presentations and has 5 issued patents. He has served on the Editorial Board of Journal of Nanomaterials & Molecular Nanotechnology since 2013. Dr. Motamed received a BS degree in Biology from University of San Francisco and a PhD degree from the University of California, Davis in Microbiology.
Stefan Mühlebach, regulatory science lead for non-biological complex drugs at Vifor Pharma–Fresenius Medical Care Renal Pharma Ltd. (Switzerland), chairs the Non-Biological Complex Drugs (NBCDs) Working Group at Lygature, a nonprofit, private-public partnership in the Netherlands. He is a university professor, medical faculty member, and member of the clinical pharmacy & epidemiology unit at the Department of Pharmaceutical Sciences at the Natural Sciences Faculty (Switzerland). Research activities, graduate and postgraduate teaching cover topics in pharmacology, clinical nutrition, hospital pharmacy, and regulatory sciences. He has authored over 100 peer-reviewed papers and several book chapters. From 1980 to 2005, he served as a chief hospital pharmacist in Switzerland. He is an honorary member of the Swiss Association of Public Health Administration and Hospital Pharmacists and a board member of the Swiss Academy of Pharmaceutical Sciences. In 2008, he joined Vifor Pharma Ltd as chief scientific officer.
Chetan Pujara is vice president, small molecule product development at Allergan, Plc. His organization is responsible for designing and developing pharmaceutical dosage forms intended for clinical trials and commercialization. SMPD develops topical sterile ophthalmic solutions, suspensions and emulsions, sustained-release ocular biodegradable implants, oral tablets/capsules, topical dermal gels & creams and other locally acting dosage forms. Prior to joining Allergan, Chetan was employed by Abbott Laboratories/Abbvie, where he held various positions in global pharmaceutical R&D, gaining experience in development of solid oral dosage forms and pediatric oral suspensions.
Pujara is also a member of the USP Dosage Forms Expert Committee and serves on the USP <771> Ophthalmic Preparation Expert Panel. He serves as a scientific advisor to the editors of Journal of Pharmaceutical Sciences and an adjunct professor in the Department of Industrial and Physical Pharmacy, Purdue University. Pujara has also contributed to the Physical Properties Working Group of Product Quality Research Institute.
Andre Raw, PhD
Center for Drug Evaluation and Research, US Food and Drug Administration website | publications
Andre Raw received his BS from the Massachusetts Institute of Technology and his PhD in chemistry from the University of California at Berkeley. He 2001, he joined the FDA as a reviewer within the Office of Generic Drugs, where he is currently acting senior scientific and policy advisor in the Office of Lifecycle Drug Products in the Office of Pharmaceutical Quality. Raw was involved in the development of several FDA initiatives, including the Guidance on Pharmaceutical Solid Polymorphism in Abbreviated New Drug Applications (ANDAs), Regulations on Listing of Polymorph Patents in the “Orange Book,” and Question Based Review – Quality by Design (QbD) Initiative, QbD Example for Generic Modified Release Products, and Guidance for Industry: Pharmaceutical Solid Co-Crystals. He has also been active in addressing scientific and regulatory issues raised in citizen petitions. He was instrumental in FDA’s recent approval of generic versions of complex active ingredients including Lovenox (enoxaparin sodium), and Ferrlecit (sodium ferric gluconate complex in sucrose).
Stephan Stern is acting deputy director and senior principal scientist at the National Cancer Institute’s Nanotechnology Characterization Laboratory (NCL), located at the Frederick National Laboratory for Cancer Research in Frederick, Maryland. NCL assists in all phases of the nanomedicine drug development process, from early preclinical to late stage clinical trials, working with academic laboratories and the pharmaceutical industry. At NCL, Stern oversees nanomedicine pharmacology and toxicology. Stern’s research interests include novel drug formulation, bioanalytical method development, and pharmacokinetic modeling. Prior experience includes a postdoctoral fellowship at the University of North Carolina–Chapel Hill in the Division of Drug Delivery and Disposition, and curriculum in toxicology, and work within regulated areas of the pharmaceutical industry. He received his BS in biochemistry from the University of Rochester and his PhD in toxicology from the University of Connecticut at Storrs. Stern is a diplomate of the American Board of Toxicology.
Wyatt Vreeland, PhD
The National Institute of Standards and Technology publications
Wyatt Vreeland earned his PhD in chemical engineering from Northwestern University, where he developed techniques for the electrophoretic separation of natural and synthetic polymers in microfluidic devices. Later, Vreeland joined National Institute of Standards and Technology as an National Research Council postdoctoral, where Vreeland focused on using liposomes to package chemicals and release those reagents at controlled times and locations in microfluidic systems. Additionally, during his postdoctoral fellowship he undertook the technical development of a field-portable electrophoresis system for forensic DNA analysis for the Department of Justice. Most recently, Vreeland’s research has focused on controlled synthesis and characterization of colloidal protein systems as can be encountered (usually undesirably) in many of today’s complex drug therapeutics. In 2015, Vreeland served as an U.S. State Department Embassy Science Fellow for the U.S. Embassy in Prague, Czech Republic, where he toured the country’s burgeoning biotechnology industry.
Gary West is currently a member of the board of directors of Azaya Therapeutics. A retired radiation oncologist, he graduated from the University of Colorado Medical School and did his radiation oncology residency at the University of New Mexico, where he was affiliated with New Mexico’s Los Alamos Meson Facility (LAMF), before completing his residency at the Joint Center for Radiation Oncology (JCRO), Harvard University. He completed a research fellowship at JCRO, where he investigated chemotherapy drug delivery in human tumor cells. While in the Air Force, he was chief of the radiation oncology department at Wilford Hall USAF Medical Center. He has also served as chief of staff at the University of Texas Health Science Center, Cancer Therapy, and Research Center (CTRC), in San Antonio and as a member of the CTRC board of governors. He is a retired member of the American Society of Clinical Oncologists and the American Society of Therapeutic Radiologists.
Elena Wolff-Holz is medical assessor at the Paul-Ehrlich-Institut and a member of the Biosimilar Working Party (BMWP) of the Committee for Medicinal Products for Human Use (CHMP) and a national expert to the Oncology Working Party (OWP) of the CHMP, where she contributes to scientific advice procedures and the development of guidelines and reflection papers. Wolff-Holz spent 14 years in the biotech industry, where she held various positions in clinical development and medical marketing functions at Centocor Inc (now J&J) and Amgen in the U.S. and in Germany, before joining the German national regulatory agency. In the area of biotherapeutics, she is responsible for advising companies on drug development issues, reviewing applications for marketing authorization in the EU and assessing clinical trial applications. She is also a lecturer covering training of experts and executives from academia, regulatory bodies and biopharmaceutical industry. Wolff-Holz has an MD degree from Heidelberg University and a postdoctoral fellowship at Harvard Medical School.
Gillian Woollett, SVP at Avalere, where she leads the FDA Policy and Regulatory Strategy Practice, an advisory services firm she launched in 2012 that supports clients throughout the healthcare system, from patients to biopharma companies and payers/providers. Woollett and her team translate into practical action all aspects of regulatory engagement strategy and policy development relevant to commercial success for multiple multi-national clients. Concurrently, she created the Avalere FDA Fellows Program to enable scientists to transition effectively into the policy environment with over 20 now having used this stepping stone to transition careers. Woollett earned her BA and MA in biochemistry from the University of Cambridge, and her DPhil in immunology from the University of Oxford. She was a postdoc in the Department of Molecular Biology at the University of Edinburgh, and at the Biomedical Research Institute, Rockville, MD funded by USAID.
Jon de Vlieger, PhD
Non Biological Complex Drugs Working Group and Lygature website | publications
Jon de Vlieger obtained his doctoral degree in bio analytical chemistry from Vrije University (the Netherlands). In 2011, he joined Top Institute Pharma, an independent nonprofit organization based that catalyzes the development of new medical solutions for patients by driving public–private collaboration between academia, industry, and society. Recently, a merger between leading Dutch technology institutes Center for Translational Molecular Medicine and Top Institute Pharma formed Lygature. For Lygature, de Vlieger coordinates several international public private partnerships, including the Non Biological Complex Drugs Working Group, an international network of scientific and clinical experts from academia, industry and regulatory bodies, with expertise in many aspects of the development and evaluation of NBCDs. He is a co-editor of the book on NBCDs in the American Association of Pharmaceutical Scientists’ Advances in the Pharmaceutical Sciences Series.
Organizers
Melanie Brickman Borchard, PhD, MSc The New York Academy of Sciences
Alison Carley, PhD The New York Academy of Sciences
Daan J.A. Crommelin, PhD Utrecht University
Wenlei Jiang, PhD Office of Research and Standards, Office of Generic Drugs, US Food and Drug Administration
Scott McNeil, PhD Nanotechnology Characterization Laboratory
Vinod Shah, PhD Non Biological Complex Drugs Working Group
Jon de Vlieger, PhD Lygature
Presented by
How to cite this eBriefing
The New York Academy of Sciences. Equivalence of Complex Drug Products: Scientific and Regulatory Challenges.Academy eBriefings. 2016. Available at: www.nyas.org/ComplexDrugs16-eB
Introduction
Speakers
Jon de Vlieger Non Biological Complex Drugs Working Group
Scott McNeil Lygature and Nanotechnology Characterization Laboratory
According to the Generic Pharmaceutical Association, almost 90% of prescriptions in the United States in 2015 were for generic drugs. Because generics are considered identical to their branded counterparts, pharmaceutical companies can forgo costly large-scale clinical trials. Instead, companies must demonstrate that a generic has pharmaceutical equivalence and bioequivalence to a licensed product. Pharmaceutical equivalence refers to the active ingredient, dosing, and strength, and can be confirmed via chemical and analytical methods. Bioequivalence refers to how a drug acts in the body and is evaluated via pharmacokinetic and/or pharmacodynamic studies. If these two conditions are met, regulatory agencies consider the generic to be safe and efficacious based on the clinical studies conducted on the branded drug.
Demonstrating the equivalence of generic complex drugs to their branded counterpart has unique challenges not encountered with small molecules.
Despite the success and advantages of generic drugs, users of certain drug categories, such as orally inhaled drugs used to treat asthma, currently have no access to generic counterparts. In addition, less than 50% of ophthalmic products and less than 40% of topical drugs have generic versions. That’s largely because these drugs represent complex drug products. In the newly released Generic Drug User Fee Act (GDUFA) “Regulatory Science Pritories,” the FDA defines complex drugs as those having complex active ingredients, such as peptides, polymers, or complex mixtures; complex formulations and/or dosages, such as liposomes, iron colloids, and long-acting injectables; complex routes of delivery, such as locally acting drugs, ophthalmic drugs, suspensions, emulsions, and gels; and/or complex drug–device combinations, such as nasal sprays and inhalers.
Demonstrating the equivalence of generic complex drugs to their branded counterpart has unique challenges not encountered with small molecules. First, the active components of complex drugs are often unknown, as are the critical attributes, i.e., the physical and chemical characteristics essential for efficacy and safety. Complex drugs are also difficult to fully characterize, and the products are very sensitive to changes in manufacturing, which is often proprietary.
In addition to above mentioned complex drug categories, the symposium also addressed biosimilars, generic versions of biologics, such as monoclonal antibodies, which share several of the hurdles to demonstrating equivalence.
Drugs can be classified into three categories. Small molecules are easy to characterize and to demonstrate equivalence. Biologics and complex drugs are more complicated, and it is difficult to demonstrate equivalence. (Image courtesy of Stefan Mühlebach)
Lawrence Mayer of Jazz Pharmaceuticals gave the keynote address on the development of a liposome-based drug delivery vehicle designed to maintain optimal levels of two cytostatics.
Several speakers spoke about the regulatory issues for biosimilars and complex drugs. Daan Crommelin of Utrecht University and Gillian Woollett of Avalere Health outlined some of the general issues to regulating generic complex drugs. Wenlei Jiang of the US Food and Drug Administration (FDA) and Elena Wolff-Holz of the Paul Ehrlich Institute provided the perspectives of the FDA and European Medicines Agency (EMA), respectively. Elywn Griffiths of the World Health Organization (WHO) outlined the WHO’s perspective.
There were several presentations on the approval of Glatopa (glatiramer acetate injection), a generic version of Copaxone (glatiramer acetate injection) for the treatment of multiple sclerosis. Andre Raw of the FDA outlined the evidence that the FDA required for approval of Glatopa while Joseph Glajch of Momenta Pharmaceuticals described the company’s approach to developing and characterizing it. Iris Grossman of Teva Pharmaceuticals presented data that show differences between the brand name drug and its generic counterpart.
Several generic versions of iron sucrose have been approved throughout the world. Stefan Mühlebach of Vifor Pharma presented evidence that several iron sucrose similars (ISS) are less effective than their branded counterparts. Beat Flühmann, also of Vifor, discussed his work on understanding pharmacists’ perspective on ISS.
Three speakers presented their approaches to evaluating the equivalence of complex drugs. Chetan Pujara of Allergan presented data on analyzing the equivalence of ophthalmic emulsions. Gary West of Azaya Therapeutics discussed regulatory hurdles to developing a generic form of Doxil (doxorubicin HCl liposome injection). Kouros Motamed of NantBioScience discussed the company’s efforts to develop a new drug delivery method for the cytostatic paclitaxel.
Two speakers focused on technical challenges to characterizing complex drugs. Wyatt Vreeland of the National Institute of Standards and Technology (NIST) described the advantages and caveats of several techniques to measure nanoparticle size. Stephan Stern of the Nanotechnology Characterization Laboratory (NCL) described a new technique to more accurately measure nanomedicines in the blood.
Speaker Presentation
Keynote Presentation
Keynote Speaker
Lawrence Mayer Jazz Pharmaceuticals
Highlights
Drug-delivery vehicles can control the pharmacokinetics of drug combinations to maintain a drug ratio that maximizes efficacy while minimizing toxicity.
Vyxeos, a nanoscale drug delivery system, was developed to deliver two chemotherapies, daunorubicin and cytarabine, in a 5-to-1 molar ratio.
In Phase 3 trials, Vyxeos demonstrated improved overall survival compared to daunorubicin plus cytarabine in patients with acute myeloid leukemia.
Built to scale
Lawrence Mayer described the development of Vyxeos (formerly CPX-351), a drug delivery system in Phase 3 trials for the treatment of acute myeloid leukemia (AML).
Vyxeos is a liposome-based drug delivery system that delivers the chemotherapies daunorubicin and cytarabine in a 5-to-1 ratio. In various cancer cell lines, this ratio was shown to have either additive or synergistic efficacy. Mayer described several of the technical features that can be altered to achieve the desired drug release rate, including membrane rigidity, charge, cholesterol content, and copper content.
The relative ratios of the chemotherapies cytarabine and daunorubicin can affect the combination’s efficacy. Some ratios are synergistic, while others are additive or antagonistic. (Image courtesy of Lawrence Mayer)
Vyxeos was compared to the current chemotherapy regimen of cytarabine and daunorubicin in two Phase 2 and one Phase 3 clinical studies in patients with AML. In all three trials, patients treated with Vyxeos had a significantly higher overall survival. Other indicators of efficacy, such as response rates and post-transplant survival were also better in patients treated with Vyxeos. Jazz Pharmaceuticals is pursuing FDA approval of Vyxeos. The FDA granted the drug breakthrough status earlier this year.
Mayer stressed the importance of a scalable manufacturing process and biophysical characterization early in drug development. A well-characterized biophysical profile ensures that the product produced in large-scale production is the same as that produced and studied during small-scale testing. It also ensures that the features of the product do not vary considerably from batch to batch.
Speaker Presentation
Video Chapters 00:00 Introduction 06:00 Key to exploiting drug ratio-dependent synergy 12:34 Leukemia cell update of intact liposomes 19:18 A robust commercial-scale nanomedicine 27:00 Conclusions
Regulatory Considerations
Speakers
Daan J.A. Crommelin, PhD Utrecht University
Elwyn Griffiths World Health Organization and Health Canada
Wenlei Jiang, PhD Office of Research and Standards, Office of Generic Drugs, US Food and Drug Administration
Elena Wolff-Holz Paul Ehrlich Institute
Gillian Woollett Avalere Health
Panel Discussion Moderator:
Scott McNeil Nanotechnology Characterization Laboratory
Highlights
Regulatory pathways for small molecule generics and biosimilars are well established, while requirements for non-biologic complex drugs are considered on a case-by-case basis.
The FDA is continually investigating new pharmacokinetic data and methods to assess the bioequivalence of complex drugs.
New guidance was released by the EMA in 2014 that expands the definition of biosimilar and provides additional direction to industry.
Regulatory pathways for generics and biosimilars
Daan Crommelin began by defining some key terms relating to complex drug products and outlining the regulatory pathways for different types of drugs. According to Crommelin, drugs can be divided into three main categories: small molecules; biologics, such as vaccines, blood and blood components, gene therapies, tissues, and recombinant proteins; and non-biologic complex drugs (NBCDs), synthetic drugs that do not have a single, homogeneous active substance and cannot be fully characterized. The composition, quality and in vivo performance of NBCDs are highly dependent on the manufacturing processes of the active ingredient as well as (in most cases) the formulation. They often consist of nanomedicines such as polymeric micelles, liposomes, or peptide-polymers. Crommelin pointed out that regulatory agencies do not always agree on these definitions; while the EMA considers low molecular weight heparin a biologic, the FDA considers it a complex drug.
The regulatory pathways for small molecules and biologics are relatively well defined. For small molecules, therapeutic equivalence (TE) is assumed by demonstrating pharmaceutical equivalence (PE) and bioequivalence (BE). For biosimilars, additional data, including pharmacokinetic (PK) and (pre)clinical data are required. Unlike small molecules, biosimilars are not considered identical to the branded agent. (Image courtesy of Daan Crommelin)
The regulatory approval process for generic small molecules is well established, and generics are considered interchangeable with their branded counterpart. A separate process has been created for biologics. Similar to generics, biosimilars can be approved via an abbreviated regulatory process that usually involves pharmaceutical equivalence, pharmacokinetic, and preclinical data. Biosimilars are considered highly similar, but not identical, to the original drug.
The regulatory process for NBCDs is often conducted on a case-by-case basis. Because NBCDs cannot be fully characterized and the critical attributes required for efficacy are often unknown, it is difficult to demonstrate bioequivalence for a generic NBCD. The FDA and EMA release guidance documents for NBCD classes outlining which analyses are needed to demonstrate similarity. These documents are continually reviewed and revised.
Multi-faceted considerations for regulatory approval of biosimilars and complex drugs
Gillian Woollett stressed that the considerations for biosimilars and complex drug similars are not only scientific, but also legal, regulatory, and economic. Regulatory agencies must balance the need for scientific and clinical evidence with the need to provide patients affordable drugs in a timely manner. According to Woollett, too high a standard can be as problematic as too low a standard if it prevents access to drugs. The FDA and EMA have an additional responsibility to set a standard for the rest of the world. A product approved in the EU and US can generally be approved anywhere; however, one approved in emerging markets, such as China, Russia, and Brazil, may not be approved in other markets. In the US, only four biosimilars have been approved; however, several agents have been approved under the definition of generic biologics. In comparison, 23 biosimilars have been approved in the EU.
The considerations for biosimilars and complex drug similars are not only scientific, but also legal, regulatory, and economic.
One issue surrounding biosimilars is that they must be compared to the reference biologic approved in a given market. This can make it difficult for companies to pursue approval globally. Another issue that may need to be addressed is the addition of orphan indications to reference biologics. Because the FDA gives exclusivity for orphan indications, these indications would not be included in the biosimilar’s product label.
The FDA’s perspective on determining the equivalence of complex drugs
Wenlei Jiang described how the FDA assesses the bioequivalence of complex generics. Jiang stressed the FDA’s commitment to complex generics through the abbreviated new drug application (ANDA) approval pathway and GDUFA, which employs regulatory science initiatives for generic drugs. Specifically, Jiang showed research efforts under GDUFA that have developed new bioequivalence methods for complex drugs.
Traditional pharmacokinetic studies to demonstrate the bioequivalence of complex drugs are difficult to conduct. For some drugs, such as long-acting polymeric microspheres, which are commonly used in drug delivery, their long-acting nature would require very long studies, which may be impractical. Based on pharmacokinetic modeling research conducted by Alkermes, the FDA updated its guidance on the bioequivalence requirements for long-acting polymeric microspheres to include drug exposure up to 28 hours.
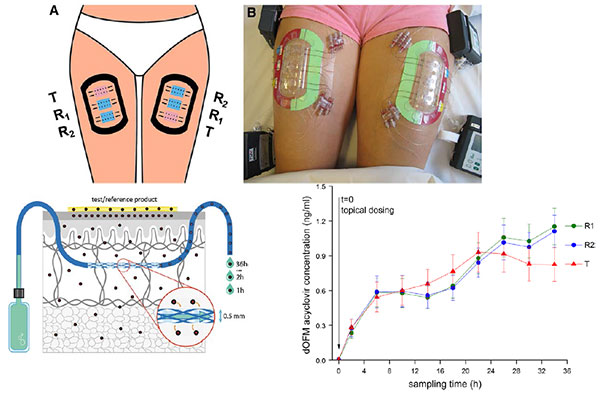
For complex drugs that act locally, such as topical skin products and nasal sprays, conventional studies that monitor drug blood levels may not be relevant. The FDA has sponsored research on new options for dermal pharmacokinetic studies, such as open-flow microperfusion (see slide).
Open-flow microperfusion can be used to monitor drug levels of topical creams in the dermis. (Image courtesy of Wenlei Jiang)
Jiang also presented a new analytic technique, morphology-directed Raman spectroscopy (MDRS), that can determine drug particle size and shape within a nasal suspension. MDRS has supported the recent approval of mometasone nasal suspension.
CHMP/EMA perspective on biosimilars
Elena Wolff-Holz described the EMA’s perspective on evaluating biosimilars and how the process has evolved over time. The EMA releases several overarching and product-specific guidelines, which are continually reviewed and revised. In a recent update to the overarching guidance (CHMP/437/04 Rev. 1), the EMA expanded the concept of a biosimilar to any biological medicinal product, including vaccines, allergens, and cell and tissue therapies, which were previously excluded. It also stressed that a biosimilar contains “a version of the active substance of an already authorized original biological medicinal product,” implying that biosimilars should not be used as reference products. In the new guidance, the goal of clinical data is to address slight differences in product characteristics, and safety and efficacy do not need to be re-established. Finally, if the reference biologic receives a new indication, the indication of the biosimilar may also be extended without the need for additional studies, if scientifically justified.
The evolution of biosimilars in the EU. New legislation is shown in red; new EMA guidelines are shown in green, and new authorizations are shown below the blue arrow. (Image courtesy of Elena Wolff-Holz)
Wolff-Holz noted that the approval process for biosimilars, which emphasizes physicochemical properties, can be difficult for clinicians, who want to know the clinical information for a drug, to accept. While clinical data for biosimilars are not included in the product’s Summary of Product Characteristics (SmPC), they are in the European Public Assessment Reports (EPAR), which clinicians are not as familiar with.
The WHO’s role in biosimilars and complex generics
Elwyn Griffiths described WHO’s role and position on biosimilars. While WHO is not a regulatory agency, it sets global standards for safety and quality. The WHO Expert Committee on Biological Standardization meets annually to establish recommendations and guidance on the quality, safety, and efficacy of biologics.
There are three major WHO guidance documents pertaining to biologics and biosimilars: Guidelines on the quality, safety and efficacy of biotherapeutic protein products prepared by recombinant DNA technology, published in 2013, Recommendations for the evaluation of animal cell cultures as substrates for the manufacture of biological medicinal products and for the characterization of cell banks, published in 2010, and Guidelines on the evaluation of similar biotherapeutic products, published in 2009.
The 2009 guidelines on similar biotherapeutics define similar biotherapeutic products (SBPs) as similar in terms of quality, safety, and efficacy to a licensed reference biological product (RBP). Similarity is established by characterizing the SBP and comparing it to the RBP in head-to-head studies. Comparison trials should be designed to detect differences in safety and efficacy between the SBP and RBP, not to establish the efficacy of the SBP. The guidelines also state that if an RBP has more than one indication, the indication of the SBP may also be expanded if scientifically warranted. One subject the WHO guidelines leave up to national regulatory agencies is whether SBPs should be considered interchangeable with RBPs.
Speaker Presentations
Video Chapters 00:00 Introduction 01:52 Complex drug products definitions 07:47 Three drug classes 13:16 What is the issue? 17:47 No access to biosimilar pathway for NBCD-similars
Video Chapters 00:00 Introduction 03:35 WHO biological standards 09:29 Regulatory oversight of biotherapeutics 15:13 WHO guidelines on evaluation of similar biotherapeutic product 23:38 Summary WHO standards
Video Chapters 00:00 Introduction 02:32 NDA versus ANDA 07:12 Consideration on PLGA sameness 13:24 Challenges for therapeutic equivalence of nasal spray products 15:13 Scientific rationale for weight-of-evidence approach 20:54 Summary
Video Chapters 00:00 Introduction 03:03 Scope includes next generation biosimilars 10:43 Manufacturing changes authorized by EMA 18:09 What if PK similarity is not convincingly demonstrated?
Video Chapters 00:00 Introduction 01:38 Working definitions for biologics 05:51 Biologic approvals have increased and are expected to rise 10:27 Biosimilars approvals across the world 18:58 Biosimilars represent a new and different business
Video Chapters 00:00 Introduction 00:50 Thoughts on the definition of the API and does it need to be updated 05:48 Measuring release of drugs 07:40 Critical factors, quality attributes for complex drugs 17:51 Looking forward to how further complexity affects biological responses 21:49 IP and open data review in a profit-driven industry
Comparisons of Copaxone (glatiramer acetate injection) with Its Generic Glatopa (glatiramer acetate injection)
Speakers
Joseph Glajch Momenta Pharmaceuticals
Iris Grossman Teva Pharmaceuticals
Andre Raw U.S. Food and Drug Administration
Highlights
Glatopa (glatiramer acetate injection), an FDA-approved generic of Copaxone(glatiramer acetate injection) is considered similar to the branded product based on the tests required by the FDA.
Additional comparisons have revealed differences between the drugs that may affect safety and efficacy.
Glatopa: a complex generic drug for multiple sclerosis
Glatopa was approved by the FDA in 1996 as a generic version of Copaxone for the treatment of multiple sclerosis. These drugs consist of glatiramer acetate, a complex mixture of polypeptides produced by polymerizing four amino acids and then partially depolymerizing the resulting peptides.
Scientific considerations to approaching complex generics
Andre Raw discussed the scientific considerations to approaching generic versions of Copaxone (glatiramer acetate) and Lovenox (enoxaparin sodium) injections, two of the complex active ingredients recently approved in generic versions by the FDA. Raw argued that understanding the nature of the complexity of these drugs is key to evaluating generic similars. For instance, the complexity of Copaxone comes from the polymerization of activated amino acids, which determines the sequences of the polypeptides, and the subsequent partial depolymerization.
To ensure similarity of Copaxone and Lovenox similars, the FDA drafted guidance listing four criteria that generic products must meet. First, the pharmaceutical company must demonstrate equivalence in its reaction scheme. Second, the FDA places constraints on several physicochemical properties, such as molecular weight distribution and amino acid composition. This also means that the structural signatures, which reflect the polymerization and depolymerization processes, and biological assays will be similar as well.
The third criterion requires that generic manufacturers identify “process signatures;” equivalence in these signatures ensures that the generic active ingredient is manufactured with effectively the same polymerization kinetic and cleavage biases as the brand name. Finally, the fourth criterion relies on the equivalence of biochemical and/or biological markers for activity to ensure sameness. Unlike the previous three criteria, which in their aggregate ensure equivalency of molecular diversity, this criterion serves as a confirmatory test to ensure equivalency in functional biochemical or biological markers.
Comparison of Copaxone and Glatopa for FDA approval
Joseph Glajch described the tests that Sandoz conducted to demonstrate the equivalence of Glatopa and Copaxone. In approximately 50 physiochemical and 10 biological tests, Glatopa fell within an acceptable range considered to be equivalent to Copaxone. Glajch stressed that these analyses must be conducted on dozens of lots to understand the diversity and variability within the drug. He showed the data from some of these analyses, including molecular weight distribution, amino acid composition, and structural signatures. He also showed that the drugs have similar effects on disease intensity in a model of autoimmune encephalomyelitis and similar results on histamine release from cells.
Additional comparisons of Copaxone and Glatopa
While Raw and Glajch showed that Glatopa and Copaxone are similar according to the methods required by the FDA, Iris Grossman described studies using higher-resolution techniques conducted by Teva Pharmaceuticals that reveal differences in surface charge and molecular weight density and distribution. In addition, Glatopa had greater batch-to-batch variability in these characteristics than Copaxone.
Copaxone and Glatopa are similar based on the physicochemical tests required by the FDA (rows 1, 2, and 4). However, other, higher-resolution methods demonstrate differences. (Image courtesy of Iris Grossman)
These differences may have consequences on efficacy and safety. In mice, of the thousands of genes affected by Glatopa and Copaxone, approximately 10% were different between the two drugs. The genes that differed were involved in pathways important for efficacy, including inflammation and immune response.
Based on these results, Teva has submitted comments on the draft FDA guidance on glatiramer acetate injections.
Speaker Presentation
Video Chapters 00:00 Introduction 02:37 Physicochemical differences relevant to mode of action 10:22 Relevance of differences to function and safety 13:50 Immunological triad 17:25 Functional effects summary and conclusions
Issues with Iron Carbohydrate Similars
Speakers
Beat Flühmann Vifor Pharma Ltd
Stefan Mühlebach, PhD Vifor Pharma Ltd
Panel Discussion Moderator:
Daan J.A. Crommelin Utrecht Universit
Highlights
Several approved generics of iron carbohydrate complexes are not as effective as their branded counterparts.
Hospital pharmacists are not aware of the differences between iron carbohydrate products and often substitute these products without informing a patient’s physician.
Iron carbohydrate similars
Iron carbohydrate products are used to treat anemia in patients with chronic kidney disease. Several iron carbohydrate generics were approved in Europe in the mid-2000s. According to Stefan Mühlebach, there was no regulatory process for complex similars at this time, and the drugs were approved via the small molecule generic route. Researchers and regulators were not aware that the active pharmaceutical ingredient was not fully characterized, and iron carbohydrate similars were deemed identical to and interchangeable with the original drugs without additional efficacy or safety studies. Since then, real-life clinical studies have shown that show the approved iron carbohydrate similars are not clinically identical to the original formulations.
The EMA and FDA have reacted to these data and have published several guidance papers on iron carbohydrate similars.
The hospital pharmacist’s approach to iron complex carbohydrates
Beat Flühmann of Vifor Pharma described the pharmacist’s perspective of complex generics using iron sucrose, a type of iron carbohydrate, as an example. In a survey hospital pharmacists in France and Spain, Flühmann found that pharmacists substitute 30% to 50% of branded iron sucrose prescriptions with a generic version. Approximately 40% of pharmacists believed that the products have the same efficacy and safety, while the remaining 60% had no opinion. In addition, many pharmacists did not inform the physician that they had dispensed the generic version.
Despite clinical data that show significant differences in efficacy and safety among iron sucrose similars, most pharmacists are not aware of these differences. (Image courtesy of Beat Flühmann)
Flühmann stressed the importance of educating pharmacists on the differences in biosimilars and complex generics. Vifor conducted a roundtable discussion earlier this year with leading hospital pharmacists throughout Europe to discuss how to select nanosimilars for hospital formularies. The roundtable added several criteria for hospital formulary committees to consider when selecting a nanosimilar, including particle size and size distribution, pharmacokinetics, and stability of ready-to-use formulations.
Speaker Presentations
Video Chapters 00:00 Introduction 04:40 Therapeutic equivalence from manufacturing to efficacy and safety 09:32 Current situation for follow-on approval 14:48 NBCD product evaluation 18:32 Landscape of drugs follow-ons
Video Chapters 00:00 Introduction 03:11 Making biosimilars available globally 08:25 The unbound drug vs release and release mechanisms 12:11 Interchangeability and acceptability in the market 16:27 Proposed systems for biosimilars and for currently approved biologics 20:12 Concluding thoughts
Other Case Studies of Complex Generics
Speakers
Kouros Motamed NantBioScience, Inc.
Chetan Pujara Allergan
Gary West Azaya Therapeutics
Highlights
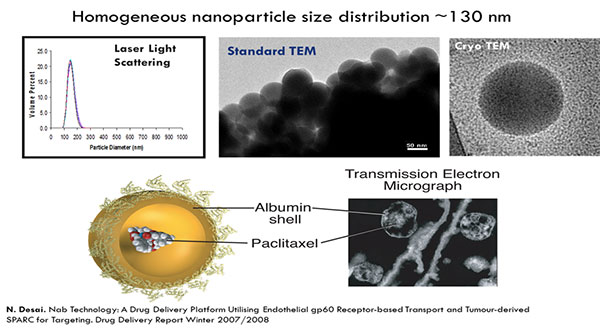
The bioequivalence of Cynviloq, a polymeric micelle formulation of the chemotherapy paclitaxel, and Abraxane (paclitaxel protein-bound particles for injectable suspension), an approved albumin-bound paclitaxel, is being investigated in the study TRIBECA.
Robust criteria are needed to ensure the equivalence of different ophthalmic emulsions.
Greater harmony between the FDA and EMA could streamline the approval of a generic version of Doxil (doxorubicin HCl liposome injection).
Cynviloq: a new formulation of paclitaxel
Kouros Motamed discussed a polymeric micelle formulation of the chemotherapy paclitaxel, Cynviloq, which is approved in several Asian countries for breast and lung cancer under the brand name Genexol-PM. These approvals were based on comparisons to Taxol (paclitaxel), a formulation of paclitaxel containing the excipient Cremophor EL. In the US and EU, approval requires comparison to Abraxane, an albumin-bound formulation of paclitaxel approved for breast, lung, and pancreatic cancer.
Evolution of paclitaxel therapies. (Image courtesy of Kouros Motamed)
In in vitro studies, Abraxane and Cynviloq had similar pharmacokinetic properties at therapeutic doses. At higher doses, the Abraxane concentration sharply increased, resulting in increased toxicity. The concentration of Cynviloq, however, did not increase as quickly, and therefore may be less toxic at higher doses.
A pharmacokinetic bioequivalence study, TRIBECA, was conducted in patients with metastatic breast cancer. Sorrento Therapeutics issued a press release stating that TRIBECA demonstrated bioequivalence of Abraxane and Cynviloq. In 2015, Cynviloq was acquired by NantWorks and has been renamed Nant-paclitaxel.
Demonstrating equivalence of ophthalmic emulsions
In 2013, the FDA released draft guidance on cyclosporine emulsions. To test whether this guidance was sufficient, Allergan tweaked its manufacturing process to make nine cyclosporine emulsions similar to Restasis (cyclosporine ophthalmic emulsion). Chetan Pujara showed that although these emulsions met the FDA criteria for similarity, there were key physicochemical and biological differences. For example, the cyclosporine distribution between the phases of the emulsion varied between the drugs. This corresponded with differences in the drug’s ability to permeate human corneal cells. Allergan also saw variability in the amount of cyclosporine in tears in rabbits.
The updated FDA guidance, released in 2016, incorporates suggestions by Allergan based on these data. However, Pujara stressed that further research on linking in vitro results to in vivo performance and on robust methods to characterize emulsions is still needed.
Regulatory barriers to a generic version of Doxil
Gary West called for harmony between regulatory authorities, citing the recent difficulties that Azaya Therapeutics has had in gaining approval for its generic doxorubicin. Doxorubicin, a treatment for ovarian cancer, is marketed by Janssen in the US under the brand name Doxil and in the EU under the brand name Caelyx (pegylated liposomal doxorubicin hydrochloride for injection).
Can international regulatory agencies work together to remove barriers facing approval of generic drugs?
Currently, Caelyx is the reference drug for doxorubicin in the EU. In the US, the FDA established a generic version of doxorubicin, ANDA 203263, as the reference drug for doxorubicin due manufacturing concerns with Doxil. However, the FDA discovered that the plant manufacturing the generic version was not complying with several guidelines, which led to contamination. West argued that due to these issues, the FDA-approved doxorubicin generic may not be the best comparator. He showed certificates of analysis from the sole manufacturer that made both Caelyx and Doxil in 2013 that demonstrate that, at that time, the two drugs were the same product with a different label and argued that they should therefore be considered interchangeable by regulatory agencies.
Azaya Therapeutics’ investigational doxorubicin generic, dubbed ATI-0918, was shown to be bioequivalent to Caelyx. However, because the EMA requires that Caelyx be sourced within the EU, and the FDA requires generics to be compared against the reference standard ANDA 203263, the company faced regulatory hurdles from both agencies. West called upon the agencies to work together to remove the barriers facing approval of generic drugs.
Speaker Presentation
Video Chapters 00:00 Introduction 03:21 A triple-down, unintended, regulatory catch 22 09:52 Lipodox versus Sun product 18:28 Regulatory barriers 22:29 Conclusions
Analytical Techniques for Characterizing Complex Drugs
Speakers
Stephan Stern Nanotechnology Characterization Laboratory
Wyatt Vreeland The National Institute of Standards and Technology
Highlights
Choosing the right analytical method is important when measuring the size of nanoparticles.
A new method to measure plasma drug concentration for nanomedicines is being validated by the NCL.
Techniques to measure nanoparticle size
Wyatt Vreeland described the advantages and disadvantages of several techniques to measure nanoparticles size.
The most common technique for measuring nanoparticle size is batch light scattering. In this method, the particle size is determined based on their ability to scatter light waves. This method is quick, simple, and nondestructive. However, because larger particles scatter light much more than smaller particles, a small amount of large particles can drown out the signal due to smaller particles, resulting in significant errors.
To avoid this complication, mixtures can be separated by size by either size-exclusion chromatography (SEC) or field flow fractionation (FFF) and then measured by light scattering. One advantage of FFF over SEC is that it can separate delicate or soft colloidal particles, which are often components of complex drugs. FFF can be used to separate particles of a few nanometers to 1000 nanometers.
Vreeland also discussed several new techniques that measure particle size by monitoring individual particles. In nanoparticle tracking analysis (NTA), particles are imaged directly with a laser, and their size is determined by tracking the extent of diffusion over time. While NTA is a robust tool to measure particle size, it is only effective within a narrow concentration range. A second technique, resonant mass measurement measures the change in frequency a particle causes as it flows through a vibrating cantilever. In addition to size, this technique, unlike others, can also measure buoyant density; however the cantilever is prone to clogging and cannot be used to measure liposomes. Finally, electrical sensing zone measures the change in electrical conductivity as a particle travels through a pore between two electrodes. This technique is similar to Coulter counter, which is used to measure bacteria and viruses. This is a very new technique for nanoscale particles.
A new method to measure nanomedicine plasma levels
The concentration of drugs administered via nanoparticles can be divided into three forms: the nanoparticle-encapsulated form, the unencapsulated free form, and the unencapsulated protein-bound form. Current methods to separate the encapsulated from unencapsulated drug promote un-encapsulation and do not differentiate protein-bound from encapsulated drug.
In two pharmacokinetic studies of Caelyx, the measured levels of unencapsulated drug differed by 6-fold, while the levels of unencapsulated drug differed by almost 12-fold, likely due to problems in fractionation methods.
Stephan Stern presented a new stable isotope tracer technique being developed by the NCL to separate and measure nanomedicine drug fractions. NCL is working with the FDA to evaluate this method for determining the bioequivalence of generic nanomedicines. As part of this effort, the NCL is conducting in vitro bioanalytical studies as well as bioequivalence studies in rats of Abraxane and Genexol-PM, discussed by Motamed, and doxorubicin HCl and Doxil, discussed by West.
In the stable isotope tracer method, an isotopically-labeled drug is added to the blood sample. The free and bound drug forms are then separated through a semi-permeable membrane. The percentage of labeled drug that does not pass through the membrane is used to determine the percent of bound drug, which can then be used to calculate the concentrations of bound and unbound drugs. (Image courtesy of Stephan Stern)
Speaker Presentations
Video Chapters 00:00 Introduction 03:48 Nanomedicine pharmacokinetics 08:39 Sources of intra-subject variability 13:43 Novel stable isotope tracer method 19:26 Measuring unbound drug in evaluating nanomedicine pharmacokinetics
Video Chapters 00:00 Introduction 02:50 Batch light scattering 08:11 How laminar flow works in FFF 13:18 Dynamic light scattering 17:52 Resonant mass measurement 20:18 Future directions
Open Questions
How can researchers determine the critical attributes for complex drugs?
What are the best methods to characterize complex drugs?
What are the most appropriate pharmacokinetic methods to evaluate bioequivalence of complex drugs?
Should biosimilars and complex generics be considered interchangeable with their branded counterparts? What criteria are necessary to demonstrate interchangeability?
How can regulatory agencies balance the need for robust scientific and clinical evidence with the need for affordable medications when evaluating complex generics?
How can regulatory agencies reach agreements on how to evaluate complex drugs?
How can companies and regulatory agencies communicate the potential clinical differences between original and generic complex drugs?
Teva Pharmaceuticals Industries Ltd. [press release] Teva Files Citizen Petition with the U.S. Food and Drug Administration (FDA) Regarding the Complexity of COPAXONE® (glatiramer acetate) Following the Agency’s Guidance. July 3, 2014.
Wenlei Jiang
Babiskin A et al. Pharmacokinetic modeling and simulation of naltrexone for extended-release injectable suspension to derive alternative BE metrics. ACoP. 2015.
Ambardekar and Stern. NBCD Pharmacokinetics and Bioanalytical Methods to Measure Drug Release. In Daan Crommelin D and de Vlieger J (ed) Non-Biological Complex Drugs; the Science and Regulatory Landscape. Springer, New York, NY; 2015: In-press.
Charles Serhan’s groundbreaking research is changing the way we view inflammation and the strategies for its therapeutic resolution.
Published October 1, 2016
By Daniel Radiloff
The 2016 Ross Prize in Molecular Medicine was awarded to Charles N. Serhan, PhD, DSc, who serves as the Simon Gelman Professor of Anesthesia, Perioperative and Pain Medicine at Harvard Medical School and Professor of Oral Medicine, Infection and Immunity at Harvard School of Dental Medicine.
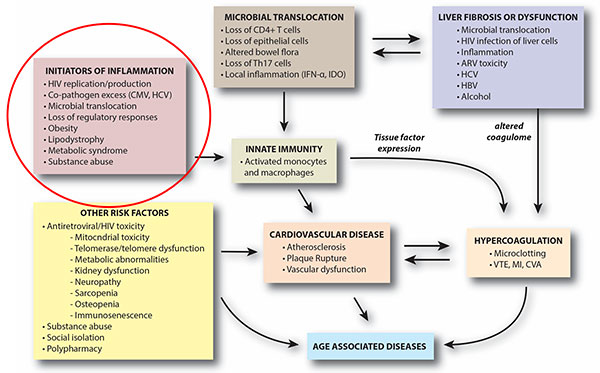
Dr. Serhan received the Award, which is conferred by the Feinstein Institute for Medical Research and Molecular Medicine, at a scientific symposium held at the Academy on June 13, 2016, in his honor. A pioneer in the field of inflammation resolution research, Dr. Serhan was the first researcher to identify anti-inflammatory cellular mediators, including resolvins and lipoxins, which are critical in regulating the pro-inflammatory pathway. These discoveries have paved the way for increased understanding of how the resolution of inflammation can be translated into therapies for a variety of human diseases.
We sat down with Dr. Serhan to discuss the award, the scope and impact of his research, and the importance of mentorship in developing the next generation of scientists.
What is the current research focus of your laboratory?
The main research focus of the lab is the elucidation of the mechanisms involved in the resolution of inflammation and structural elucidation of the mediators in order to understand organ protection and collateral tissue damage, as this is the basis of many diseases and the collateral stress and damage for surgical interventions.
How did you choose mediators of the inflammatory response as the basis of your work?
I have always been interested in chemistry and biochemistry. The notion of chemical mediators orchestrating the immune response intrigued me from learning about things like histamines and the early prostaglandin research. You could say I have stuck with this research through my entire career, as there were enough questions to ask to go deeper and deeper which led to resolution, which no one had really studied before in a mechanistic fashion.
What was the “eureka” moment, when you realized that your research on these pathway could be used for therapeutic purposes?
It has been a steady progression. I have to say that at one point I did have an epiphany about the whole system—that it was a straight line that has yet to be fully realized, and we could use each one of the mediators we have identified to serve as a backbone for therapeutics. I would say another moment was rewriting the errors in the biochemistry textbooks on how essential fatty acids were actually regulating inflammatory responses. Overall, it has been an incremental process and a lot of slow, hard work—more than one moment.
What will be the next injury whose treatment will be influenced by your and others’ research in the inflammation field?
The stress of surgery is well recognized among surgeons as an acute inflammatory response, as is reflow injury, when blood reflows to tissue. These are two areas we can have a big impact on. Demonstrations are currently underway at a clinical trial level focused on ocular dry eye inflammation using a resolvin E1 mimetic. This work is based on a company I was involved in starting in 2000, but I am no longer actively involved in this venture.
Additionally, an orphan disease of great public health importance focused on by my lab is periodontal disease, which is inflammation-induced bone loss around the peridontium. We were able to go from a mouse model to a rabbit model thanks to NIH funding and have been able to develop a GMP-synthesis and pro-resolving mouth rinse.
A trial is on, with more than sixty people enrolled at the Forsyth Institute, to see if we can stimulate resolution of inflammation in the early stages of periodontal disease. This is being done in collaboration with Tom Van Dyke and his colleagues at the Forsyth Institute, with support from NIH/NIDCR. So I have a focus in my lab on periodontal disease, thinking that if we control local inflammation, what would be the impact on systemic inflammation. There is evidence in a lot of papers showing links to all sorts of systemic diseases resulting from periodontal disease.
What do you hope will be the long-term impact of your research from a global perspective?
One aspect we haven’t really touched on, but which is really important, is having a better education about the role of nutrition in an appropriate innate immune response. Some of our work underscores how important fatty acid nutrition is—a different side of our work that is still very important.
Did you always envision yourself as a scientist, or did you dream of being something else as a youth?
As you know, no one really sees themselves as a geek growing up. I really enjoyed chemistry when I was younger, tinkering around with chemistry sets and microscopes, but as I got older really wanted to be a musician. I even spent time on the road touring with bands, but I had a very swift change of heart and went back to my roots, deciding to study biochemistry at Stony Brook, and had a great experience as an undergraduate. Today, I still don’t really see myself as a scientist but rather a biomedical investigator. I always have seen scientists as people who work on rocket ships.
Do you think your musical training has had any influence on how you approach scientific research?
Yes, most definitely, it does play a role in science. The way I organize the laboratory projects is analogous to orchestration of music. Also, I would compare developing patience, skill and rigor in the scientific process to developing musical skills through continual practice. The more proficient you become mastering scales and rudiments in music, the more confident you become in your skills, and I see scientific research the same way.
Were there any individuals in your life that steered you towards science or played an important role in you becoming a scientist?
Yes, I had great science teachers in elementary school and absolutely loved them and loved science. When I was at graduate school at NYU I frequently visited high school science classes and told them how exciting scientific research was.
Were there any major challenges you had to overcome in your career to becoming a successful scientist?
Oh yeah, trying to remain continually funded is a real challenge. Other than that, overall, I have been very lucky, having great mentors and a supportive family. I’ve also had great trainees over the years, with about 90% of them successfully moving on to the next steps in their career.
Speaking of mentors, what is the most valuable lesson that you have learned from your mentors over the course of your career?
Anyone that does reasonably well in science has to have not only one mentor but a half a dozen mentors. I was lucky enough to work with the Lasker Award Winner Michael Heidelberger, the father of immunochemistry, when I started graduate school at NYU, who was retired at the time and in his 80s.
I learned two things from him that made a large impact on me: 1. You have to work on something you love to get you through the difficult times, and 2. You have to write everything down and make observations, because you will get distracted and forget things. To this day, I make people in my lab have two notebooks—an electronic one for detailing their experiments and one for writing down their ideas.
What do you hope that your mentees will pass along to their own mentees one day?
Of course, almost everyone would say the passion for experiments, but I would say steadfastness, commitment, and rigor are the key, because there are many things that can lead you astray these days.
What does winning the 2016 Ross Prize in Molecular Medicine mean to you?
I can’t even find the words to express it, I am so humbled and makes me very proud. On a personal level it’s nice for the people in my lab as they can see something to aspire to.
As the Academy approaches its bicentennial, we’re reaching out to top minds in emerging fields to get their opinions on the future of the sciences. What emerging fields do you think are the most exciting?
That’s a hard one. There are a lot of emerging areas of science that are exciting. Science drives technology and technology drives science. Lately, I have been working on tissue regeneration, and am interested in nanotechnology and local drug delivery systems, and I believe these approaches will revolutionize medical treatment and improve life. Also, from my perspective, I would say personal metabolomics is another emerging field, which may help us to understand collective health and behavior as well as personalized medicine.
About the Ross Prize in Molecular Medicine
The annual Ross Prize in Molecular Medicine was established in 2013 in conjunction with the Feinstein Institute for Medical Research and Molecular Medicine. The winner is an active investigator who has produced innovative, paradigm-shifting research that is worthy of significant and broad attention in the field of molecular medicine.
This individual is expected to continue to garner recognition in future years, and their current accomplishments reflect a rapidly rising career trajectory of discovery and invention. The winner receives an honorarium of $50,000. Previous Award winners include: Lewis C. Cantley, PhD, Weill Cornell Medical College (2015); John O’Shea, MD, National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS), National Institutes of Health (2014); and Dan Littman, MD, PhD, New York University (2013).
From study design to patient engagement, Gary Bennett, PhD, shares his insight on what is and is not effective in applying technology to obesity research.
The need for interventions to prevent and treat obesity is extremely urgent, as over one-third of adults and 17% of children in the United States are considered to be obese based on body mass index (BMI). From wearable devices to smartphone applications for tracking diet and exercise, consumer technologies are aiming to make a positive impact on changing lifestyle behaviors and potentially decreasing obesity rates.
Gary Bennett, PhD, of the Duke Global Digital Health Science Center, is bringing digital health to obesity interventions to measure and evaluate the effectiveness of technology in increasing patient engagement and improving long-term health outcomes, such as weight maintenance. Recently Dr. Bennett shared some of his best practices when designing studies applying technology to obesity interventions, surprising study results on weight and co-existing conditions, and the most promising element for obesity tech research (that is also commonly ignored).
Considering User Engagement
According to Dr. Bennett, one of the most significant mistakes made in research on health technology and patient engagement is not taking into consideration the user experience. “We as researchers can easily get hyper-focused on theory, evidence, and innovative new functionality. However, apps are only useful if they’re actually used by patients,” he stated. User engagement is the best predictor of positive outcomes, which is why it is so important to manufacturers of consumer technology.
“Commercial smartphone application developers are constantly testing and iterating through design and functionality changes to optimize user engagement. The (research) field far too frequently adopts the ‘someone-can-make-it-pretty-later’ approach, which results in outcomes that underestimate their true effect.” Dr. Bennett also noted that creating more consumer technologies isn’t necessarily the solution to increasing patient engagement and improving health outcomes. “The existing suite of apps do a fine job of collecting data, but they’re less useful for changing behavior. What we need are creative, theory- and evidence-based tools that integrate with existing apps and leverage their data to improve patient outcomes and make clinical care (whether that’s from a primary care provider or other clinician) more efficient and effective.”
Gary Bennett, PhD
Surprising Results, Long-term Outcomes
Dr. Bennett’s research on technology and obesity has led to some surprising results with long-term outcomes. “Our Shape trial was a test of weight gain prevention app for medically vulnerable patients in primary care. Many in this group have exceedingly high obesity risk, but very little interest in weight loss. We predicted that the app would help patients avoid weight gain during the 18-month trial. However, we were surprised to find that they kept the weight off for up to four years.”
A second unexpected outcome was a nearly 70% decrease in depression among patients with high rates of depression at the start of the study, he added. The relationship between depression and obesity has been suggested to be a reciprocal one, as obesity has been shown to increase the risk of depression and depression to be predictive for developing obesity.
When it comes to a promising consumer technology for obesity research, for Dr. Bennett the most encouraging one is one we take for granted-human beings. “Nearly all of our apps work better when combined with human coaching, counseling, or care. Although most thought that digital health technologies would render us humans irrelevant, we’re now finding that they’re most useful-particularly with complex conditions like obesity-in making clinical care more efficient and effective. Ultimately, we should be focused on the data, using it to better deliver real-time personalized feedback, reminders, and notifications to patients, while identifying the ways that it can best inform clinical care.”
The processes associated with aging may be risk factors for age-related diseases. Conversely, many age-related chronic diseases accelerate aging. However, because most research is focused on specific diseases, the broad mechanisms of disease as a driver of aging have not been well studied. Understanding how disease drives aging could not only help people live longer but also improve health and quality of life during old age.
On April 13–14, 2016, researchers studying aging and three disease areas—HIV/AIDS, oncology, and diabetes—met at the New York Academy of Sciences for the Disease Drivers in Aging: 2016 Advances in Geroscience Summit. The meeting expanded on the National Institutes of Health’s 2013 Advances in Geroscience Summit, examining how chronic diseases and their treatments affect aging. The meeting also aimed to stimulate collaboration between researchers studying aging and researchers studying disease. The summit was presented by the Gerontological Society of America, the American Federation for Aging Research, the Trans-NIH GeroScience Interest Group, and the New York Academy of Sciences.
The meeting opened with four keynote presentations from geroscience researchers, followed by a series of short talks and panel discussions featuring researchers focused on HIV/AIDS, diabetes, and cancer. This eBriefing reviews the panel discussions on each disease area and the overarching discussion on common themes and ideas for collaboration between researchers studying aging and disease.
Presentations available from:
Timothy Ahles, PhD (Memorial Sloan Kettering Cancer Center) Kathryn Anastos, MD (Albert Einstein College of Medicine) Steven Austad, PhD (University of Alabama at Birmingham) James Becker, PhD (University of Pittsburgh) Caroline Blaum, MD (New York University) Judith Campisi, PhD (Buck Institute for Research on Aging) Harvey J. Cohen, MD (Duke University) Wendy Demark-Wahnefried, PhD (University of Alabama at Birmingham) Jan van Deursen, PhD (Mayo Clinic) Elissa Epel, MD (University of California, San Francisco) Kristine Erlandson, MD (University of Colorado) Brooke Grindlinger, PhD (The New York Academy of Sciences) Jeffrey Halter, MD (University of Michigan) Richard Hodes, MD (National Institute on Aging, NIH) Peter Hunt, MD (University of California, San Francisco) Beth Jamieson, PhD (University of California, Los Angeles) C. Ronald Kahn, MD (Joslin Diabetes Center) Balakuntalam Kasinath, MD (University of Texas Health Science Center) Gretchen Neigh, PhD (Virginia Commonwealth University) Rosario Scalia, MD, PhD (Temple University) Marissa Schafer, PhD (Robert and Arlene Kogod Center on Aging) Felipe Sierra, PhD (National Institute on Aging, NIH) Mary Sehl, MD, PhD (University of California, Los Angeles) Christopher Wiley, PhD (Buck Institute for Research on Aging) Panel Discussions
Presented by
How to cite this eBriefing
The New York Academy of Sciences. Disease Drivers of Aging: The 2016 Advances in Geroscience Summit. Academy eBriefings. 2016. Available at: www.nyas.org/Geroscience2016-eB
Media
00:01 1. Introduction and overview 04:25 2. What we know from basic research 11:58 3. Progress made; What we want to know; Conclusion
00:01 1. Introduction and overview 08:20 2. Chronic stress and cell aging 13:04 3. Telomeres and disease risk 15:55 4. Disease drivers; Conclusion
00:01 1. Presentation by Beth Jamieson 10:20 2. Presentation by James Becker 19:52 3. Presentation by Gretchen Neig
00:01 1. Presentation by Kathryn Anastos 10:16 2. Presentaton by Peter Hunt 20:23 3. Presentation by Kristine Erlandson
00:01 1. Introduction; HIV and aging 08:25 2. HIV and macrophages; Primate studies; Where to intervene 16:21 3. Maximizing control group resources; Biomarkers for stress 23:48 4. Regarding Alzheimer’s; Mitochondrial dysfunction; Aging and viral dormancy; Data set creation 28:56 5. Supressor mutations; Cognitive dysfunction; Conclusion
00:01 1. Presentation by Marissa Schafer 11:07 2. Presentation by Christopher Wiley 22:09 3. Presentaton by Mary Sehl
00:01 1. Presentation by C. Ronald Kahn 10:29 2. Presentation by Balakuntalam Kasinath 20:47 3. Presentation by Rosario Scalia
00:01 1. Presentation by Caroline Blaum 10:35 2. Presentation by Jeffrey Halter
00:01 1. Treatment with CDK4 inhibitors; What is accelerated aging? 09:03 2. Increased phosphorylation; Obesity, asthma, and diabetes 13:55 3. Amino acids and insulin secretion; More on accelerated aging 18:52 4. Regarding astroglial cells; The blood-brain barrier 26:40 5. Treatment with metformin; Diabetes and immunodeficiency; Rapamycin; Conclusion
00:01 1. Introduction; Choosing the right journal 04:20 2. General manuscript preparation; Discussion and introduction 11:44 3. The abstract; The title 14:38 4. Authorship; The cover letter 21:44 5. Referees; Peer review 27:44 6. Decisions; Common reasons for rejection; Revision and resubmission 34:35 7. Preparing a response; Appealing a negative decision 39:12 8. Parting thoughts; Conclusion
00:01 1. Presentation by Jan van Deursen 11:48 2. Presentation by Harvey Jay Cohen 22:09 3. Presentation by Judith Campisi
00:01 1. Presentation by Wendy Denmark-Wahnefried 10:29 2. Presentation by Timothy Ahles
00:01 1. Introduction 07:48 2. Synergy between aging and cancer research models; Aging in animal models 17:30 3. Disease interplay across disciplines; Dietary restriction; Senescent T-cells 24:12 4. Computational and systems biology; Chemotherapy and senescence; Funding 31:11 5. Anti-depressants before chemo; Intervention 40:15 6. Regarding exosomes and evolution; Conclusion
00:01 1. Panelists’ opening remarks 13:17 2. Disease treatment and lifespan extension; Targeting senescenct cells 21:06 3. Embracing complexity; Developmental manipulation in aging research; Inflammation 33:20 4. Review and funding 41:00 5. Metabolic reprogramming; Healthspan vs. lifespan; Regarding data sets 48:18 6. Mitochondrial dysfunction; Going forward; Common tools 61:28 7. Aging as disease; Stress and trauma; Drug discovery; Influence of local environment 69:28 8. Exercise; Incentivizing collaboration; Policy and funding 82:06 9. Focus on gene expression; Big data; Public perceptions 87:27 10. Cohort development; Conclusion
Sierra F, Kohanski R (eds). Advances in Geroscience. Springer International Publishing. 2016. [Ebook] Provides a comprehensive overview of geroscience.
General aging resources: journal articles
National Institute on Aging (NIA) NIA, one of the 27 Institutes and Centers of NIH, leads a broad scientific effort to understand the nature of aging and to extend the healthy, active years of life.
Jennifer Cable lives in New York City, where she experiments with different outlets to communicate science. She enjoys bringing science to scientists and nonscientists alike. She writes for Nature Structural and Molecular Biology, Bitesize Bio, Under the Microscope, and the Nature New York blog. She received a PhD from the University of North Carolina at Chapel Hill for her research in investigating the structure/function relationship of proteins.
Funding for the eBriefing of this conference was made possible, in part, by 1 R13 AG 053043-01 from the National Institute on Aging. Co-funding has been provided by the National Institute of Diabetes and Digestive and Kidney Diseases, and the National Cancer Institute. The views expressed in written conference materials or publications and by speakers and moderators do not necessarily reflect the official policies of the Department of Health and Human Services; nor does mention by trade names, commercial practices, or organizations imply endorsement by the U.S. Government.
This activity is supported by an educational grant from Lilly. For further information concerning Lilly grant funding visit www.lillygrantoffice.com
Although age is an important variable in clinical research, the effects of aging are often understudied.
Improving the quality of life during aging is as important as increasing longevity.
Short-term stress can promote resilience to aging; however, chronic stress accelerates aging.
Introduction
Aging is often accompanied by chronic diseases including heart disease, cancer, diabetes, and Alzheimer’s disease, to name a few. Many processes associated with aging may be risk factors for these diseases. While aging occurs in the absence of disease—a steady decline in health is expected as a person ages—chronic diseases also accelerate aging, exacerbating normal physical and cognitive decline.
As people age, a steady decline in health is expected (red line). Some diseases cause a temporary decrease in health followed by full recovery (first black dip). However, other diseases can change the trajectory of aging, leading to a faster decline in health (fuchsia line). (Image courtesy of Felipe Sierra)
The field of geroscience has focused on how aging affects disease, and this topic was the theme of the first geroscience summit, “Advances in Geroscience: Impact on Healthspan and Chronic Disease,” which took place in October, 2013, in Bethesda, Maryland. Papers related to that summit were published in a supplement to the Journals of Gerontology in June, 2014. However, the reverse question—how disease affects aging—has gone largely unstudied, and this topic was the theme of this 2016 meeting.
The 2016 summit examined how three diseases—HIV/AIDS, diabetes, and cancer—affect the major pillars of aging established at the first Geroscience Summit: macromolecular damage, stress response, epigenetics, stem cells, proteostasis, inflammation, and metabolism.
The meeting opened with four keynote presentations from geroscience researchers who described successful interventions to delay aging and increase life span in animal models. They also noted the need for multidisciplinary research, challenging attendees to work across disease states. Understanding common mechanisms in aging and chronic diseases could help people live not only longer but also healthier lives.The keynote presentations were followed by a series of short talks and panel discussions featuring researchers focused on HIV/AIDS, diabetes, and cancer. This eBriefing reviews the panel discussions on each disease area and the overarching discussion on common themes and ideas for collaboration between researchers studying aging and disease.
The seven pillars of aging. (Image: Kennedy BK et al., Cell 159: 709-713 [2014])
A multidisciplinary approach to aging
Richard Hodes of the National Institute of Aging (NIA) outlined the multidisciplinary structure at the NIA and National Institutes of Health (NIH) to raise awareness of the role of aging in disease and to fund aging-based research. Targeting aging may reduce the incidence of age-related diseases. The divisions of the NIA span basic biology to clinical and behavioral studies. Because aging touches so many fields, the NIH also created the Geroscience Interest Group (GSIG), with members from 21 institutes. Hodes called on researchers to step outside the silos of their specialties and to study features of aging common to disparate disciplines and diseases.
Hodes also presented evidence of the importance of considering age when choosing treatments for patients, and highlighted the need to include elderly subjects in preclinical and clinical studies. In the Diabetes Prevention Program, both medication and lifestyle changes reduced the risk of developing diabetes in at-risk patients younger than 60 years. However, in subjects older than 60, only lifestyle changes were effective. In a pre-clinical study, elderly mice with cancer died sooner when given immunotherapy than those who did not receive treatment.
Felipe Sierra, also from the NIA, pointed to the need to re-examine our approach to disease. The elderly often present with several comorbidities. Instead of considering each disease individually, researchers should consider interactions between diseases, and between disease and aging.
The keynote speakers also described efforts to promote aging research. In late 2015, the NIA released a request for applications to test whether the age of laboratory animals affects outcomes in studies investigating disease. In the NIA’s Interventions Testing Program (ITP), researchers can submit compounds to be tested for an effect on extending life span in mice.
Increasing health span as well as life span
Steven Austad of the University of Alabama at Birmingham emphasized that increasing longevity is not the same as improving health. Several interventions can extend life span in animals. In some cases, such as the use of rapamycin in mice, health span is also improved. Indeed, rapamycin extends life and delays Alzheimer’s disease, cancer, atherosclerosis, and heart dysfunction in mice. However, genetic mutations that increase life span in the worm Caenorhabditis elegans do not extend the period of good health. Furthermore, life-extending interventions are not without side effects. In mice, dietary restriction and rapamycin have been linked to low bone density, immunosuppression, cataracts, diabetes, and hyperlipidemia.
Life expectancy (gray) and health expectancy (blue) of men and women at age 65. An increase in life span does not always correlate with improved health. (Image: Kennedy BK et al., Cell 159: 709-713 [2014])
Longer human life expectancy with improved treatments for fatal diseases often comes at the cost of declining quality of life and increased disability—Alzheimer’s disease, dementia, frailty, vision loss, pain, joint replacement, and other conditions. Treating the underlying causes of aging may prevent this deterioration in quality of life.
Telomere length as a marker of aging
Elissa Epel of the University of California, San Francisco, discussed the relationship between stress and cell aging. Epel uses telomere length—stretches of repeat DNA at the end of chromosomes—as an indicator of aging. Chronic disease can accelerate telomere attrition; while there are myriad biochemical alterations in each disease, many diseases of aging feature the triad of oxidative stress, inflammation, and hyperglycemia / insulin resistance. For example, in diabetes the disease processes of impaired β-cell function, and resulting higher levels of biochemical stressors, further shorten telomeres.
Psychiatric diseases, particularly major depression and anxiety disorders, are also associated with shortened telomeres. Given the high comorbidity of medical and psychiatric conditions, Epel noted, it is important to consider that depression may affect aging biology, not just the physical disease condition. Treatments for diseases may further affect the rate of telomere attrition, either speeding it up or slowing it down. For example, statins and possibly metformin, used in diabetes treatment, may prevent telomere attrition, while HAART therapy in HIV may accelerate telomere attrition. Chemotherapy can work through telomere damage of cancerous as well as healthy cells. Childhood traumas followed by chronic stressors in adulthood result in shortened telomeres, which correlate with several diseases of aging, including diabetes, cardiovascular disease, stroke, and cancer. Shortened telomeres might be both a cause and a consequence of chronic disease, although this has yet to be fully confirmed.
Disease Drivers of Aging: HIV, Diabetes, and Cancer
Chairs
Ronald Kohanski
National Institutes on Aging and Geroscience Interest Group, NIH
Steven Deeks
AIDS Research Institute; University of California, San Francisco
Claudia Gravekamp
Albert Einstein College of Medicine
Arti Hurria
City of Hope National Medical Center
Jeffrey Halter
University of Michigan
Kevin High
Wake Forest University
Nir Barzilai
Albert Einstein College of Medicine
Highlights
Each person has a unique fingerprint of chronic viral infections—HIV is one example.
HIV treatment normalizes some markers of aging.
Some manifestations of diabetes are relevant to aging, others are not.
Insulin resistance in the brain may accelerate age-related cognitive impairment.
Both cancer and cancer therapies promote cellular senescence and inflammation, which contribute to aging and disease.
Cancer treatment affects areas of the brain that are also changed by aging; these treatments can promote cognitive decline.
Aging with HIV
Despite the success of antiretroviral (ARV) therapy in improving health and increasing life span, people living with HIV are at an increased risk for many age-related diseases, such as cardiovascular disease, cancer, osteoporosis, liver disease, and cognitive impairment. Several panelists stressed the need for a multidimensional approach to investigate HIV and aging, saying that researchers should consider interactions between the seven pillars of aging described during the keynote presentations and focus on possible root causes driving aging.
Although the molecular pathways of aging in people living with HIV are well understood, the field lacks high-quality biomarkers to assess the effectiveness of interventions in clinical trials. The panelists advised aging researchers to make use of the large cohorts established in HIV, particularly MACS, WIHS, and VACS. Researchers have been following both infected and uninfected subjects in these cohorts for up to 30 years, and several types of samples, including serum, DNA, plasma, and urine, are available for study.
Many factors associated with HIV infection and treatment affect pathways involved in aging. (Image courtesy of Steven Deeks)
Gretchen Neigh of Virginia Commonwealth University discussed social stress and HIV. Her work in a rhesus monkey model, used to mimic human infection, showed that previous social stress increased the viral load of simian immunodeficiency virus (SIV) and delayed ARV response. The audience was curious as to whether this effect was attributable to the virus itself or to the illness that SIV causes. This question is difficult to answer in current animal models. Neigh added that the rhesus monkey model could be useful for studying the psychosocial aspects of HIV infection and for studying how social stressors affect viral reservoirs.
Beth Jamieson of the University of California, Los Angeles, showed that ARV therapy can partially normalize DNA methylation patterns, a hallmark of aging. She would like to explore this area further to find out how factors such as duration of infection and early treatment influence this effect. One attendee suggested targeting mitochondrial dysfunction to mitigate the effects of HIV on aging. The panelists pointed to the dearth of studies linking mitochondrial dysfunction to end-organ disease and noted that several older ARVs are mitochondrial toxins, complicating such analyses. Another area of investigation is infection of macrophages by HIV. While most of the panelists focused on infection of T cells, HIV infects macrophages during later stages of disease and could be a source of persistent inflammation.
The effects of type 2 diabetes on aging
It is difficult to establish which complications of type 2 diabetes accelerate age-related effects and which are specific to hyperglycemia, unrelated to aging. For example, patients with diabetes may experience vascular complications, such as neuropathy and nephropathy. However, these effects do not occur with normal aging and are likely a specific consequence of hyperglycemia. However, as Nir Barzilai of the Albert Einstein College of Medicine reminded attendees, researchers are not starting from scratch. Metformin, a common diabetes medication, also prevents several age-related diseases. Understanding this mechanism could be a starting point from which to investigate the effect of diabetes on age-related diseases.
Several audience members asked about the role of insulin resistance in the brain. During his presentation, C. Ronald Kahn of the Joslin Diabetes Center showed that knocking out the insulin receptor in the brain increased measures of anxiety in elderly mice but not in young mice. Kahn’s data also showed the importance of astroglia in insulin signaling. Attendees asked whether there were different families or subsets of astroglia in terms of insulin receptor expression or whether the cells had increased epigenetic variance with age. Kahn replied that he has not seen either effect, but added that he had not specifically looked for them.
One attendee questioned whether a homozygous knockout, which eliminates insulin signaling, is the best model for diabetes, noting that patients with diabetes retain some insulin signaling. Kahn replied that a heterozygous model may better recapitulate the biology of insulin resistance and that it may be worthwhile to use such a model.
There are many pathways and sites through which insulin resistance can affect aging in the brain. (Image courtesy of C. Ronald Kahn)
Another attendee asked about the use of CDK4 inhibitors, which are approved to treat some types of cancer. Jeffrey Halter of the University of Michigan showed that knocking out CDK4 in mice destroys β cells, which are responsible for producing insulin. Halter suggested that oncologists monitor for signs of β-cell dysfunction in patients taking CDK4 inhibitors for cancer. In addition, data from clinical trials of CDK4 inhibitors could be assessed retrospectively to evaluate whether these drugs have negative effects on β-cell function in humans.
One attendee asked the panel about the effects of asthma and decreased oxygen in obese people with diabetes and asthma. While no one on the panel has specifically investigated this relationship, the panelists cited studies in obese diabetics in which sleep apnea was shown to exacerbate insulin resistance. Improving sleep apnea decreased insulin resistance and diabetes.
Diabetes causes a subtle immunodeficiency. In other immunodeficiency models, such as HIV and transplant, cytomegalovirus (CMV) has been shown to play a role in driving vascular disease. One attendee postulated that CMV infection could be a good model to study the interaction between diabetes and aging in terms of vasculature, leukocytes, and endothelial function.
Premature aging caused by cancer and chemotherapy
Jan van Deursen of the Mayo Clinic explained that, in addition to apoptosis, chemotherapy can also induce cellular senescence in tumor cells. The panelists further explained that senescent tumor cells can be cleared by the immune system and that their ability to persist depends on the type of chemotherapy administered.
In patients with cancer, cellular senescence can occur as a consequence of normal aging or as a consequence of disease or treatment-related factors. (Image courtesy of Jan van Deursen)
Timothy Ahles of Memorial Sloan Kettering Cancer Center described how cancer and its treatment result in cognitive decline. One attendee remarked on how brain imaging in normal aging has evolved to not only monitor damage but also to look at compensatory mechanisms that may result from more serious brain damage. Ahles explained that cancer researchers have learned a lot from imaging studies of both normal aging and cognitive impairment because many of the systems affected by normal aging are also affected by cancer treatment. Wendy Demark-Wahnefried of the University of Alabama at Birmingham presented data on accelerated adverse body composition changes that occur as a result of cancer treatment, with chemotherapy inducing gains in fat and losses in muscle in the year following diagnosis that are comparable to 10 years of normal aging.
There are many good mouse models of cancer, but the disease is often studied in young animals, and studies using these models cannot investigate how aging affects cancer. The panelists noted that there has been a push in the research community to use models that develop cancers more slowly, and for researchers using models to induce cancer in older animals. However, achieving these goals can be difficult because it is time consuming and costly to maintain elderly animals. To defray some of these costs, the trans-NIH Geroscience Interest Group (GSIG) put out an RFA, joined by several other Institutes including NCI, to age animal models of disease. Funding for these research projects will be provided jointly by NIA and other relevant NIH institutes. The panelists encouraged researchers to look outside mouse models; a recent review described studies of naturally occurring cancers in pet dogs. The panelists also suggested studying cancer in nonhuman primates.
Several attendees asked about how to mitigate the effects of chemotherapy. Some patients undergo short-term fasting before chemotherapy, which has been shown to promote tumor shrinkage in mice. However, researchers have not studied whether this strategy promotes longevity, similar to the effect of dietary restriction in mice. Similarly, researchers have not systematically studied the effects of antidepressant use before chemotherapy, which has been shown to prevent negative cognitive outcomes of chemotherapy in animal models.
The panelists recommended early interventions, such as exercise during chemotherapy, to prevent or reverse decline in physical function in cancer patients. However, they also noted that later interventions can be effective. In the RENEW trial, an international sample of 641 older, long-term cancer survivors at least 5 years out from diagnosis who received materials and counseling on good dietary and exercise habits had a slower decrease in physical function than those who did not. In another initiative, cancer survivors paired with a gardener had healthier habits, improved function, and improved biomarkers of aging after one year of gardening.
The Way Forward
Moderator
Felipe Sierra
National Institute on Aging, NIH
Highlights
There is a need for a uniform definition of accelerated aging and standardized biomarkers to monitor aging.
Researchers should identify and focus on the root causes that drive aging instead of downstream effects.
Funding agencies should ensure that suitable aging-related experiments are included in grant proposals.
A call for uniformity
The meeting ended with a panel discussion on common themes and open research questions to advance therapies for chronic diseases and aging. Several attendees mentioned the need for a uniform definition of accelerated aging. There are many ways to define aging, ranging from molecular and cellular processes to functional ability and population age. In many animal models of aging, life span is the primary outcome for aging. However, this outcome would not be informative for clinicians; it does not reveal whether a patient is experiencing accelerated or normal aging or whether a treatment is improving the effects of aging. One attendee suggested creating an NIH toolbox of biological markers of aging to provide a common vocabulary for researchers. Currently, the best biomarkers of aging are composite measures that usually include function. The panelists recommended that studies measuring aging should include data representing at least two pillars of aging, such as DNA methylation and resistance to a stressor.
Several attendees also suggested that the research community create a single database, such as those housed at WikiPathways, to organize the biological pathways involved in aging and disease. Websites that currently house this information for aging do not include information on the relationships between aging and disease.
The big picture
Several panelists noted the importance of interactions between the seven pillars of aging. However, they cautioned against focusing on any single pillar and advised that the pillars be used as a guide and not as rigid categories for aging research. It is nonetheless clear that cellular senescence and inflammation are among the most important features of aging common to the three diseases discussed at this meeting. Cellular senescence has many forms, and targeting one form may not prevent others. Several attendees pointed out that therapeutic targeting of any one marker of inflammation or cellular senescence may not remedy their underlying cause(s) and their subsequent effects on aging and disease.
Funding and resources
The panelists also noted the need for more aging studies in general. One reason that investigators are hesitant to study aging is the time and expense of using aged animal models. While some larger centers, such as the Pepper Institute at Florida State University and the Shock Center at the University of Washington, have the infrastructure to do so, smaller institutions do not. Audience members recommended that the facilities at these centers be made available to researchers, particularly junior faculty, to help recruit more people to the aging field. The panelists also noted that datasets of relevance to aging are available on the NIA website.
Another reason for the lack of aging studies is the difficulty of acquiring funding for long-term, complex studies. The panelists remarked that grant reviewers sometimes ask that aging-related experiments be removed from proposals. Instead, aging experts on review committees should ensure that such complexity is included in proposals and confirm that an appropriate model system is being used so that studies on diseases that affect the elderly are not conducted in young mice. One audience member suggested supplements to existing grants be made available to fund extra samples for aging research. For example, ancillary studies could make use of specimens collected in clinical trials to analyze predictors of aging.
Open Questions
General
How can we best bring together those who study disease and those who study aging?
How should clinicians define aging and accelerated aging?
What biomarkers can be used to evaluate accelerated aging in the presence of chronic diseases and to assess the effects of interventions?
What are the best animal models to study accelerated aging in the presence of chronic disease?
Are life-extending therapies that work in animal models relevant to humans, and will they also extend health?
How can funding agencies, such as the NIA, encourage investigators to consider the effects of aging in their model systems?
Effects of HIV on aging
What is the role of senescent T cells in age-related diseases?
What can epigenetic changes in T cells tell us about the link between these cells and diseases of aging?
How does psychosocial stress affect HIV pathogenesis and response to treatment in humans?
What information can be gleaned from established HIV cohorts with respect to HIV and aging?
Future research questions for HIV and aging
How do disease factors, such as duration of infection and time of treatment, influence the effects of ARV therapy on markers of aging?
What can primate models of HIV infection tell us about psychosocial aspects of disease and how social stressors affect disease reservoirs?
What role might mitochondrial dysfunction play in HIV’s effect on aging?
How does infection of macrophages contribute to inflammation?
Effects of diabetes on aging
How do some diabetes therapies (eg, metformin and acarbose) increase longevity?
Which complications of diabetes are relevant to aging, and which are specific to increased blood glucose?
Could insulin resistance be a protective mechanism against accelerated aging?
Future research questions for diabetes and aging
How do CDK4 inhibitors affect β-cell function?
How do conditions that decrease the supply of oxygen, such as asthma and sleep apnea, influence insulin resistance?
What role might the immunodeficiency caused by diabetes play in driving vascular dysfunction?
Effects of cancer on aging
What are the different signs of, effects of, and treatments for cancer-related and chemotherapy-related senescence?
How can we definitively show that inflammation and coagulation affect function and survival?
Future research questions for cancer and aging
Can lifestyle changes improve cognitive function in older cancer patients?
How might short-term fasting prior to chemotherapy affect aging?
Can taking antidepressants before initiating chemotherapy mitigate cognitive decline?
The term “bioelectronic medicine” may seem to be more science fiction than medical reality, but this field of science has recently made significant strides in translating research from the lab to the clinic with promising results. From implantable devices to treat autoimmune diseases without medication to microchips to help quadriplegics regain movement, bioelectronic medicine is quickly moving into the forefront of scientific applications.
The premise of bioelectronic medicine is that nearly all cells in the human body are in some way regulated via information communicated from electrical signals from the nervous system. Similar to how implantable artificial pacemakers emit electrical impulses to regulate a heartbeat, various technologies have been developed to block, stimulate, or regulate the body’s neural signals to control the underlying molecular targets of many diseases.
Bioelectronic Medicine: A Viable Therapeutic Field
Bioelectronic medicine would not have emerged as a viable therapeutic field without the work of Kevin J. Tracey, MD, President and CEO of The Feinstein Institute for Medical Research-specifically, a key discovery in May of 1998. At the time it was believed that there was no communication between the nervous system and the immune system, but Tracey devised an experiment to test his own hypothesis on a link between the two systems.
Kevin J. Tracey, MD
Tracey predicted that stimulation of the vagus nerve with electrical impulses would reduce production of tumor necrosis factor (TNF), a cell signaling protein linked to inflammation. Electrical impulses were delivered to an exposed vagus nerve in a rat and after the cut was closed, Tracey administered endotoxin to trigger inflammation.
Seventy-five percent of TNF production was blocked, through activation of what Tracey coined as “the inflammatory reflex.” Since these research findings were published in Nature in 2000, Tracey has co-founded SetPoint Medical to develop an implantable device to stimulate the vagus nerve as a treatment for rheumatoid arthritis (RA) that is intended to last for 10 years. Results from a pilot study reported that patients with this implant experienced symptom improvements comparable to those taking medications for RA and a long-term study is currently underway.
A Chip Implanted in the Brain
Chad Bouton, also from The Feinstein Institute for Medical Research, was recently the lead author in a landmark study appearing in Nature on a neuroprosthetic device that, for the first time in a 24-year-old man with quadriplegia, allowed a paralyzed man to move his hand using only his brain. First, functional magnetic resonance imaging (fMRI) scans of Ian Burkhart’s brain were taken while he attempted to complete a range of hand movements; once Bouton and his team identified from the fMRI the areas of the motor cortex associated with the movement attempts, a chip was implanted in Burkhart’s brain.
This chip is designed to note the electrical activity from the motor cortex that is linked to movement and to transmit this information to a computer, which eventually translates these signals and sends them to a flexible sleeve on Burkhart’s arm. The result? Burkhart’s muscles were stimulated, and over time with training he has been able to make isolated finger movements and complete six different wrist and hand motions. There are limitations to the technology, as it can currently only be used in a laboratory for a limited amount of time and requires recalibration before each use.
Regardless, Burkhart sees great value in bioelectronic medicine. “Even if it’s something that I can never take home in my lifetime, I’m glad I’ve had the opportunity to take part in this study. I’ve had lots of fun with it. I know that I’ve done a lot of work to help other people as well,” Burkhart told Nature.
Patients with life-threatening illnesses face challenges in accessing potential therapies at the cutting-edge of research and development, which have not yet been proven in a clinical trial. Some pharmaceutical companies produce and provide medicines on a case-by-case basis through expanded access or “compassionate use” programs. The tension among principles of fairness, equity, and compassion are explored in this podcast through a case study about a social media campaign led to an expedited clinical trial for an investigative antiviral medicine. Guests will explore the provocative and emotional stories of patients, family members, advocates, researchers, physicians, and the regulators charged with keeping medicines in the marketplace safe and effective.
This podcast was a collaboration between The Division of Medical Ethics at NYU School of Medicine and The New York Academy of Sciences.
It’s difficult to imagine a world without antibiotics-since the discovery of penicillin by Alexander Fleming in 1928, antimicrobial drugs and substances have saved millions of lives and controlled the spread of countless infections and diseases. But with the alarming increase in strains of drug-resistant bacteria and questions about the link between antibiotic use in animals and human health, new strategies are needed.
An important element of this holistic approach is to complement the control of antibiotics prescribed to humans with strategies to judiciously use antibiotics consumed by animals in food production. Natural fruit extracts and gasses have been explored as means for curbing the spread of bacteria and initiatives to more accurately track the prevalence of drug-resistant bacteria are just a few of the ideas for reevaluating the use of antibiotics in the food system.
François Malouin, PhD, and colleagues have evaluated cranberries and their compounds as a novel antibiotic alternative for bacteria like methicillin-resistant S. aureus (MRSA), although exactly how the flavonoids work against bacteria is not clear. One poultry study also observed that adding 40mg of cranberry extracts per kilogram of feed led to 40% fewer early deaths in birds. James L. Marsden, PhD, has also analyzed interventions for controlling the genus of bacteria Listeria monocytogenes that is connected to three multistate outbreaks of listeriosis this year alone.
For controlling L. monocytogenes on food-contact surfaces, Ozone may be an effective yet inexpensive means for controlling the spread of potentially dangerous bacteria in food production. Marden’s research showed that when applied to stainless steel surfaces for 15 minutes, an advanced oxidation technology was successful in reducing multiple strains of L. monocytogenes on the previously contaminated surfaces.
A Global Public Health Issue
Antibiotics are also given in feeds for food-producing animals to promote faster growth while also reducing the amount of feed needed. However, in 2006 the European Union banned the use of antibiotics for promoting growth in animal production and since 2013 the Food and Drug Administration has called for the industry to voluntarily phase out the use of antibiotics for food production purposes.
Rebecca Irwin, DVM, MSc, and colleagues from the Canadian Integrated Program for Antimicrobial Resistance Surveillance (CIPARS) reported in 2005 that high levels of cephalosporin-resistant Escherichia coli were detected in chicken samples purchased from grocery stores in Quebec and Ontario and in chicken and human Salmonella Heidelberg samples from humans. Chicken hatcheries in Quebec agreed to a voluntary suspension of ceftiofur, a cephalosporin-type antibiotic. Unfortunately, after the voluntary ban was lifted cephalosporin-resistant E. coli and S. Heidelbergonce again re-emerged in chicken and human samples assessed by CIPARS. As of 2013, CISPARS reported that resistance to ciprofloxacin among S. Typhi human infections increased to 18%, up from 10% in the previous year.
As the demand for animal food products continues to increase while drug-resistant bacteria remain a threat, developing evidence-based interventions and antibiotic alternatives has become a significant public health need at the global level. Although antibiotics may be at times necessary in animals for food production, these alternatives could signal a systemic shift for improved food safety and both animal and human health.
Cancer researcher Christopher Vakoc, PhD, goes “above the genome” in search for leukemia drug targets. His work falls within the emerging field of epigenomics.
Published April 19, 2016
By Diana Friedman
Christopher Vakoc, PhD
If cells in the human body contain identical DNA, why are skin cells so different from lung cells? If identical twins have the same genome, what accounts for differences in their physical characteristics? Enter epigenetics-a term literally meaning “above the genome”- to refer to biological processes that impact gene expression, without altering the underlying DNA sequence. The idea behind epigenetics is that if researchers can first identify the proteins that play a crucial role in tumor cell survival, they may then be able to find means to inhibit these proteins and cut cancer pathways off at the pass.
Epigenetics is particularly appealing to cancer researchers because it could give insight into why some patients experience significant side effects, do not respond to conventional cancer treatments, or have recurrent cancer. The emerging field of epigenomics has led to the critical identification of pathways that are not only disrupted in cancer, but are also selective enough to leave the ‘normal’ cells behind, unharmed, while also contributing to treatment response.
Cold Spring Harbor Laboratory’s Christopher Vakoc, PhD, and his research team have been studying the epigenome and acute myeloid leukemia (AML); in 2011, they discovered that a protein called BRD4 (which is known to inhibit proteins responsible for “reading” the epigenome, a key step in the expression of all proteins in a cell) was found in abundance in AML, and was necessary for cancer cell replication. A drug called JQ1 was being tested as a possible treatment for other conditions but Vakoc’s team discovered that it suppressed BRD4, leading to the death of the cancer cells while normal cells survived. How exactly the drug worked was still a mystery.
A Long and Difficult Road Ahead
Vakoc’s lab suspected that the long form of an enzyme called NSD3 played a critical role in BRD4 suppression in AML, but Chen Shen, MD, PhD, a researcher in Vakoc’s lab, conducted a series of experiments with surprising findings. In stark contrast to the dogma, the unassuming NSD3-short was shown to be critical for AML cancer epigenetics. “It’s a David-and-Goliath story,” Vakoc stated. “We figured the long, or full-length, form of NSD3 was of interest because it has a portion, or domain, that enables it to act as an enzyme, and another that suggests its involvement in epigenetic gene regulation.”
When applied to AML cells, JQ1 caused NSD3-short and BRD4 to break apart, along another protein called CHD8. Not only did the researchers gain greater insight into how JQ1 worked, but they also identified CHD8 as an additional protein that could be a target in AML treatment.
Although Vakoc and his team will have a long and difficult road ahead of them in further investigating if JQ1 and other protein inhibitors are effective enough to one day become treatments approved by the Food and Drug Administration for AML, even the most modest of proteins hold promise for epigenetics. In epigenetic research, the epigenome continues to reveal the complexities of tumors but revelations about fighting cancer above and beyond the genome.