Will insects be the next big thing for foodies? Once you get past the cringe factor you might be surprised to learn these crunchy critters are quite nutritious.
A recent report by the UN Food and Agriculture Organization finds that entomophagy, the practice of eating insects (and arachnids and myriapods), is a healthy and sustainable answer to mounting worldwide nutrition and environmental challenges. “Due to the rising cost of animal protein, food and feed insecurity, environmental pressures, population growth, and increasing demand for protein among the middle classes…alternative solutions to conventional livestock and feed sources urgently need to be found,” states the report. Edible insects may offer at least a partial solution.
If this sounds like a Malthusian dystopia story, reconsider. Insects are arthropods, like lobster or shrimp. “So popping a big juicy beetle, cricket, or cicada into your mouth is only a step away,” says entomologist Jenna Jadin.
Bugs are also nutritious. How nutritious? Interestingly, this is a methodologically difficult question to answer. Insect diets, even within the same species, vary based on where they live, and the nutrient composition of an individual insect varies throughout the metamorphic stages of its life. However, studies put most edible insects about on par with other animal protein sources, explains the FAO report.
A Source of Amino Acids
Furthermore, insect protein profiles can efficiently supplement diets lacking in specific amino acids. For example, according to the FAO,
“In the Democratic Republic of the Congo…lysine-rich caterpillars complement lysine-poor staple proteins. Likewise, people in Papua New Guinea eat tubers that are poor in lysine and leucine, but compensate for this nutritional gap by eating palm weevil larvae. The tubers provide tryptophan and aromatic amino acids, which are limited in palm weevils.”
In this post for The Atlantic, James Hamblin questions the safety of eating insects, pointing out the possibility of allergic reactions. This is a fair point, especially worth pausing over if you have an allergy to seafood or other arthropods, such as shellfish. The populations most at risk for developing insect allergies are, somewhat ironically, entomologists and insect cultivators, who may develop allergic sensitivity through long-term exposure. (If you’ve worked in a lab with rats, you may have noticed and lamented a rodent version of this phenomenon.)
However, according to the FAO, “for the great majority of people…eating and/or exposure to insects do not pose significant risk of causing allergenic reactions.” Moreover, there is some evidence that chitin, the principal component of insect exoskeletons, might boost the immune system and reduce allergic responses.
Food Defect Action Levels
If you’re still not convinced, you may be either chagrined or reconciled to know that you’re eating bugs already anyway. According to a slightly cringe-inducing Scientific American post by Layla Eplett,
“The Food and Drug Administration permits a certain amount of insects in food products because it’s practically impossible to keep them completely out. The Food Defect Action Levels outlines the permissible amount of bugs (and other natural contaminants) allowed in food. According to guidelines, pasta may contain an average of 225 insect fragments or more per 225 grams; a cup of raisins can have 33 fruit fly eggs and still make its way to shelves—it’s 34 or more that are unacceptable. While these levels represent limits and the actual amount consumed is probably lower, on average an individual probably ingests about one to two pounds of flies, maggots and other bugs each year without even knowing it.”
So, you might as well embrace it?
Once you get past feeling squeamish, the subject opens up an array of interesting questions. How would edible insects be cultivated? What would be the ecological ramifications? How would international food insect standards be regulated?
Following his new award, renowned immunologist Dan Littman, MD, PhD, explains his fascination with the immune system, as well as his hopes for the future of molecular medicine.
Published June 1, 2013
By Diana Friedman
Dan Littman, MD, PhD, received the Inaugural Ross Prize in Molecular Medicine from Betty Diamond, MD, a member of the Ross Prize Committee, and investigator & head, Center for Autoimmune and Musculoskeletal Diseases, The Feinstein Institute for Medical Research.
According to the committee for the Ross Prize in Molecular Medicine, Littman is an active investigator who produces innovative, paradigm-shifting research. He was recognized for his early discoveries, as well as his ongoing research to better understand viral, immune, and inflammatory diseases.
Below, Dr. Littman discusses his research, as well as his predictions and aspirations for the field of molecular medicine.
What drew you to the field of molecular biology?
I grew up during a time when molecular biology was in its infancy. I was interested in biology in general and I became interested in studying the immune system in college where we had a fantastic course that exposed us to new ideas in this area. We didn’t know, at the time, about T cell antigen receptors, and how they specified. So it was around that time that these really fascinating questions that could be addressed by molecular biology techniques started cropping up. In the late ‘70s and ‘80s the progress in molecular biology techniques started leading to breakthroughs in many fields, including immunology and virology.
How did you get involved in studying the molecular mechanisms of HIV infection?
I got interested in it because of a molecule called CD4 that I discovered in my postdoc. It became clear that it was a receptor for HIV, so we wished to understand how it is exploited by the virus to enter the cell and whether it might be possible to block its function to prevent infection and viral spread. We discovered that CD4 is not sufficient for the virus to enter the cell, but that a second molecule, CCR5, is also required on the cell surface for virus infection.
A drug that binds to CCR5 and blocks HIV infection has been developed. It’s not widely used today because it’s not the most effective therapy, but it can be used for those patients whose infection is refractory to the commonly used anti- retroviral drugs.
Our interest has shifted over the years as we try to understand how the virus depletes the cells of the immune system. Most people with HIV can mount an anti-viral immune response, but it’s not sufficient to eradicate the virus. Even people who are controlled with medication have a residual reservoir of HIV-infected cells. That reservoir often becomes reactivated once people go off therapy. The question is whether we could get rid of the reservoir, thereby curing patients of HIV.
Can there be a protective vaccine?
We are still interested in contributing to this important goal, and our work has been focused recently on trying to understand how the virus evades a branch of the immune system called the innate immune response. The virus does have an Achilles heel, but this Achilles heel is very well concealed as far as it is recognized by the innate immune system. We want to understand how to uncover it in people who are already infected with the virus or are given a prophylactic vaccine. If we can do that, we may be able to elicit much stronger anti-viral immunity.
What is your current research focus?
Dan Littman participates in a press briefing following his reception of the Ross Prize in Molecular Medicine.
The problems that are energizing me the most have to do with how the immune system is shaped to be able to deal with various environmental stresses and microbial challenges. We are trying to understand how the different branches of the immune system are kept in a homeostatic state in which they are ready to handle any kind of environmental threat, but at the same time, avoid being overly activated— as occurs in autoimmunity or inflammation.
The way we got to this is through our research of T lymphocytes, which are needed for establishing an adaptive microbial response to pathogens. We discovered a particular type of T cell in the intestine, where there is an enormous number of microbes that are required for these cells to appear. We have co-evolved with this commensal microbiota, which provides many benefits to us. There must be a balance where there is no threat to the host or to the microbiota. This evolutionary pas de deux is what we are interested in, from the point of view of the immune system.
What did your research on T cells teach you about autoimmune diseases and their relation to the microbiota?
In the process of studying T lymphocytes we found that there is a particular type that can be especially inflammatory and can cause tissue damage. These T cells are involved in autoimmune diseases, like rheumatoid arthritis (RA), multiple sclerosis (MS), and inflammatory bowel diseases like Crohn’s disease, but they are also important for protecting the mucosal barrier. It’s important that these T cells be kept in balance. If there is a shift in the microbiota, called dysbiosis, it can result in these T cells becoming harmful to the host.
This theory has been fully established in animal models, and now there’s some evidence in humans. We now have some hints that RA is associated with dysbiosis and that there may be particular bacteria that may be responsible for eliciting T cells that attack our own cells (within the joints, in RA). We think that there is a good possibility that this is precipitated by an imbalance in the intestinal microbiota.
How could further research on the microbiota impact disease treatment?
Right now, we’re at a very early stage. We have over 1,000 different types of bacteria that compose our intestinal microbiota and we know the functions of only a handful of them. Is it possible to rebalance the microbiota? Interventions like fecal transplantation do so, and are actually a highly effective way of treating certain types of infection and may also be effective in treating inflammatory diseases.
The hope is that in the future we will have a much better definition of the components of the microbiota and how they interact with the epithelial barrier and the immune system. This would allow us to essentially create and deliver a formula of specific bacteria to target certain diseases.
We think of the impact of this on classical autoimmune diseases, like MS and type 1 diabetes, but it’s very likely that this extends much further to other diseases that can be impacted by inflammatory processes, like Alzheimer’s disease, atherosclerosis, and possibly even behavioral disorders. We think that this type of research could have far-reaching implications.
What pressing question has yet to be answered in the field of molecular biology?
We still don’t understand fundamentally how the development of an organism occurs. Stem cell research is a huge exciting field these days, and it pertains to how an entire organism can be derived from a single cell (a zygote). The mechanisms by which organisms regulate their size and their function throughout a lifetime are things we don’t yet have a great grasp on.
One of the interests in our lab, and to biologists in general, is how interaction with the environment affects developmental and physiological processes, such as the onset of chronic diseases that can be precipitated by infection or induced stress. We want to know how the environment changes the expression of genes.
The big advances in the past 30 years have come from cell biology and understanding how genes work, but whole organism physiology has taken a backseat, and for good reason—we haven’t yet had the tools to study it in the ways that we can study cell biology.
Where do you see the field of molecular medicine in 20 years?
I think the technology is moving forward very fast with regard to genomics and detecting and identifying molecules relevant to disease processes. There will be much more rapid and precise molecular diagnosis, through both genetic approaches (identifying genetic lesions) and metabolomics, and hopefully better interventions as we better understand how these relate to disease.
A molecule found in breast milk may re-sensitize MRSA to antibiotics. This could be good news, especially considering the economic disincentives to develop new antibiotics.
Published May 16, 2013
By Diana Friedman
Researchers at SUNY University at Buffalo recently published a paper finding that a molecule called HAMLET, purified from breast milk, may re-sensitize antibiotic resistant bacteria to already existing treatments. This is potentially very good news.
Bacteria such as Methicillin-resistant Staphylococcus aureus (MRSA, orresistant staph) have evolved resistance to almost everything developed to combat infection. Studies place the number of MRSA-related deaths per year in the US at about 19,000. “The reason MRSA exists,” says Maryn McKenna, author of the book Superbug: the Fatal Menace of MRSA, “is the failure of previous attempts to treat staph. Methicillin was the first of the class of semi-synthetic penicillins. They were developed in the 1960s because staph became resistant to penicillin just one year after that drug was released to market.”
After methicillin came a series of “me too” drugs. These are so similar to methicillin in molecular structure that very slight adaptations were required for MRSA to develop further resistance. A drug called vancomycin was the next step in treatment options. “MRSA’s response to that drug was quickly to evolve vancomycin resistant staph. There are two different sets of mutations—one is resistant and one is intermediately resistant. That brings us almost to the end of the available drugs,” says McKenna.
Questions Over bacterial Resistance
So, if HAMLET can re-sensitize bacteria to already available treatments, it could be a literal life-saver. HAMLET is an adjuvant, an agent that modifies the effects of another agent. In this case, the modification increases antibiotic potency, though the exact mechanisms of the synergy are not yet known. It is known that HAMLET binds to hydrogen pumps in the cell membrane that create pH and energy gradients between the inside of a cell and its external environment. Disrupting these pumps interferes with a cell’s ability to produce energy and, potentially, to expel antibiotics, but more research is required to understand the biochemistry involved, explains Anders P. Hakansson, PhD, the Principal Investigator on the paper.
Given MRSA’s relentless record of survival adaptations, the question immediately comes to mind: will the bacteria just develop resistance to HAMLET? According to Dr. Hakansson, while this is always a possibility, signs so far are positive. “It’s very easy to make antibiotic resistant bacteria strains in the lab. You take a strain that is sensitive to methicillin, for example. Then you add your antibiotic at gradually-increasing concentrations over time and then let the bacteria adapt. We tried really hard to do this with HAMLET and haven’t succeeded,” he says.
Essential to Cell Physiology
Dr. Hakansson hypothesizes that this has to do with the hydrogen pump to which HAMLET bonds. The pump is so essential to cell physiology that HAMLET-evasive mutations render the bacteria “extremely unfit.”
HAMLET’s adjuvant function may prove to be economically advantageous. Despite increasing concerns about resistance to current antibiotics, there isn’t much work in the pharmaceutical industry on innovative treatments. Of seven new antibiotics in the pipeline, none utilize novel mechanisms. “There are only a few drugs left and they’re not great,” says McKenna. “It’s a symptom of market failure.”
A report by the President’s Council of Advisors on Science and Technology describes economic disincentives behind the dearth of antimicrobial R&D. The cost of drug development has increased exponentially about every nine years since 1975. Approval for new treatments is far from guaranteed, and resistance development can take an antibiotic out of the market well before a profit can be made. Furthermore, truly new antibiotics are likely to be shelved to be used as “secret weapons” when other options fail.
Dr. Hakansson is hopeful that work on HAMLET will be able to avoid, and even help counterbalance, these issues. “An adjuvant is great because you can use it with old antibiotics that are already well-characterized and known to be safe. There might be more of an interest in industry to develop this kind of agent.”
It’s fairly evident when flu hits a given area—employees start taking sick days, lines become longer at the doctor’s office, and emergency rooms fill up. But what if people, particularly healthcare workers and those not yet vaccinated, could get just a little more warning that flu was coming, or that the current flu season had not yet peaked? These were questions Rajan Patel, PhD, senior scientist at Google Inc. and two of his coworkers, Jeremy Ginsburg and Matthew Mohebbi, asked themselves in 2007.
While the CDC has its own method for estimating flu outbreaks—mainly by relying on select doctors around the country to report counts of influenza-like illness back to the CDC. But those reports must be collected, aggregated, and disseminated—which creates about a 2-week lag time between data collection and public reporting.
Patel and coworkers embarked on a project to create a real-time measurement of flu—measurable down to the city level, even in remote areas where it is hard to collect data from on-the-ground physicians—using the data source they knew best: search engine data.
Utilizing Search Engine Data
“We built a simple linear model that used the cumulative frequency of search terms, normalized for total search volume, to estimate the influenza-like illness rates provided by the CDC,” says Patel. They had to start by filtering billions of potentially flu-related search engine queries through a correlation analysis, determining which queries best related to CDC information on symptoms of influenza-like illness. “If we just guessed at the most likely search terms, we could have had misses,” says Patel.
The process of building, tuning, and validating the model took about a year. The results, published in a 2009 Nature paper, showed that data from the new model, called Google Flu Trends, was consistent with CDC data, although Flu Trends could often predict influenza upticks in a given area at least a few days earlier. Because the project was undertaken through Google.org, the search engine giant’s not-for-profit organization, Flu Trends results are completely open access, available at www.google.org/flutrends.
Patel has since moved on to other projects, including strengthening a core search algorithm that seeks to provide better search responses to users’ search engine queries (such as “What do I do if I have the flu?”). And other researchers have since created similar epidemic-tracking models for locations around the world.
Social Networks & Epidemic Forecasting
“I hope that other companies with social network data can think of ways to use it for good,” says Patel. Answering his wish, Lucky Gunasekara, founder of data firm Vulcan, is looking at using social network data for epidemic modeling. Gunasekara explains that in contrast to Google Flu Trends, which relies on large volumes of search engine data to capture incidence, models based on social networks could “look at the actual drivers and pathways of an epidemic.”
“If you know the topology of a network, essentially its structure, then you would just have to survey certain people—your canaries in the coal mine.” These people would allow you to predict who the flu might hit, based on their social interactions. The key, says Gunasekara, is identifying the right people and the right data—“it’s a very bad idea to collect all data from everyone and assume that because we have so much, we’ll be able to do something useful with it.”
“Say there is a potential bioterrorism alert in New York City. Would you need every person to check into emergency rooms to find out who is actually sick, inciting mass panic along the way? Or would it be better to figure out models of the epidemic within our social networks and to directly message or call a sample of potentially infected people to ask, ‘Are you feeling sick?’,” says Gunasekara.
A Tall Order
There are still large challenges to overcome before social network data can be successfully used for wide-scale epidemic forecasting, says Gunasekara, not the least of which is ensuring that forecasting doesn’t spill over into profiling territory.
“Technology should enable personal agency, not take it away.” It’s also necessary to distinguish between data that indicates online interaction (like commenting on a friend’s status) and data that could reasonably indicate real-life, person-to-person interaction (such as photo-tagging). “It’s also really hard to incentivize people to provide you with their personal data for something with such a high social stigma as being sick,” says Gunasekara.
But Gunasekara and other data scientists are not discouraged, rather energized, by the many challenges facing them. “Nicholas Christakis at Harvard has already started to put together a successful epidemic surveillance model using key individuals within social networks to identify the emergence of a new epidemic,” he says.
The Key Challenge
The finding emerged out of a campus-wide flu study conducted amongst Harvard undergraduates and published in PLOS One in 2010. The findings could be applicable, as Dr. Christakis articulated to the TED community, for not just the early detection of seasonal flu but also “viral” memes and fads in both the real and online world.
“People like Nicholas and myself are trying to build thoughtfully designed and scientifically rigorous social experiments and models that, yes, could lay the basis for massively beneficial public services and platforms. Scale though doesn’t equal scientific quality,” says Gunasekara.
“The key challenge in front of us is better understanding the science behind the dynamics of these epidemics and then translating those findings into the design of new services and products that we can all collectively benefit from through one common shared experience.”
It seems simple enough—pop into a doctor’s office or, increasingly, any neighborhood pharmacy, to get a shot or nasal spray and, poof, you’re protected from the nastiest dish on the cold-weather illness buffet—that ache- and fever-inducing slide into delusional daytime naps and tossing, turning nights that we know as seasonal flu. Receiving the flu vaccine takes just a few minutes. But what we don’t often think about—the process behind the vaccine—is a much longer affair. And how much protection does the vaccine really afford?
Earlier this year, in an NIH conference center in Rockville, MD, the Vaccines and Related Biological Products Advisory Committee (VRBPAC) convened its members. At this meeting, the VRBPAC, part of the FDA, announced the specific flu strains approved to be included in 2013/2014 U.S. flu vaccines, based on recommendations from the World Health Organization (WHO). While it may seem like a boon to get this information into the hands of researchers and vaccine manufacturers so far ahead of the next flu season (which typically begins in late Fall), many flu experts indicate that this early-decision process is simply an indication that vaccine production time is too long.
“We are always limping behind,” says Peter Palese, the Horace W. Goldsmith Professor and Chair in the Department of Microbiology at Mount Sinai Medical Center in New York. “We base our vaccine choices on strains that circulated in Australia during their winter, so they are already 6 months outdated by that point.” And, once vaccine strains are approved, the production process is still another 6 – 8 months away from being ready for an arm or nose near you.
Constantly Mutating
This feeling of always chasing an adversary just out of your reach is a familiar one for most flu researchers. The problem: seasonal flu mutates faster than we can adapt current vaccines. Every time the flu virus undergoes a significant mutation, it produces a new influenza “strain” (denoted by Hs and Ns). Vaccines must be tailored to the strains currently in the environment in order to be effective.
“We created a measles vaccine in the 1950s and we are still using that exact same vaccine because the virus doesn’t change. It’s the same with Polio and hepatitis B,” says Palese. “But you can’t do that with flu.”
Perhaps the skill most prized by military strategists is the ability to adapt—and seasonal flu, a worthy enemy to our bodies’ complex defense systems, has mutation down pat. Flu, formally known as influenza, is an RNA virus that uses its hemagglutinin (HA) protein to bind to, and infect, healthy cells. The HA molecule contains a head and a stalk, with the head being the most adaptation-skilled part of the virus, and not coincidentally, the part of the virus that attaches directly to healthy cells. Thus, the reason we require an annual flu vaccine: as flu adapts to our defenses, we require new weapons.
The body’s primary weapons are antibodies (or immunoglobulin), our cells’ first-line defense to invaders—the proverbial messenger pigeon sent to warn the troops. Antibodies are immune proteins that alert the rest of the immune system and, in some cases, attack unwelcome guests directly. Flu vaccines are designed to stimulate antibodies, allowing our bodies to build up reservoirs of antibodies for specific virus strains—akin to basic training at the cellular level.
How Vaccines Work
Current vaccines work in one of two ways. The most common vaccine, which comes in an injectable trivalent shot-form, inserts inactivated flu virus into the body, allowing the body to respond with antibodies, but without the threat of actually contracting flu. The same method is employed by the intradermal shot, which features a smaller needle injected into the skin. A nasal spray, Flu-Mist®, uses weakened flu virus to achieve the same goal: activate an army of antibodies before the body comes into contact with the real enemy, readying it to pounce when the time is right.
The antibodies produced are specific to the strains in the vaccine. If researchers, such as those who attended the recent VRBPC meeting, don’t select the right strains for the upcoming flu season, the population is at greater risk of contracting flu—a risk not taken lightly by those who are familiar with its high costs, whether measured in healthcare dollars, lost work hours, or, unfortunately, mortality. Choosing strains for upcoming vaccines is a gamble, but, for now, an essential one.
Despite the challenges, researchers have a good track record when it comes to predicting which strains will be circulating half a year to a year into the future, says Doris Bucher, PhD, Associate Professor of Microbiology and Immunology at New York Medical College. “But that’s what’s been so disappointing this flu season. We did have a match with regard to strains, but efficacy was still not great, especially for people over 65; seniors did not produce a good immune response to this year’s vaccine.”
Measuring Efficacy
There is reason to believe, however, that this year’s vaccine may not have been less effective than previous years; efficacy may simply have been measured more accurately this time around. According to a 2012 report from the University of Minnesota’s Center for Infectious Disease Research and Policy (CIDRAP) Comprehensive Influenza Vaccine Initiative (CCIVI), reports of vaccine efficacy were generally cited at about 70% to 90% from studies as early as the 1940s through 2012. The report also indicates that these estimates may have been significantly overstated.
It should be noted that vaccine effectiveness, or VE, is not measured in absolute terms. Tests for influenza, while available (the CDC’s real-time reverse transcription-polymerase chain reaction, or rRT-PCR, protocol is an example), are prohibitive to administer to large portions of the population. Instead, VE relates to the percentage that people who were vaccinated are less likely to need to see a healthcare provider for influenza-like illness symptoms.
By reviewing vaccine efficacy and effectiveness studies from 1967 to 2012, CCIVI researchers found that trivalent injectable vaccines protected healthy adults (aged 18 to 64) at a rate of about 59%; there was inconsistent evidence of protection in children and Seniors. Interestingly, these data match VE reports from the 2012/2013 season rather closely—estimated at 47% against influenza A (H3N2) and 67% against B virus infections, with lack of statistical efficacy for those over 65.
Producing Novel Vaccines
Is a VE of 60% for just part of the population good enough? Michael T. Osterholm, PhD, MPH, one of the lead authors of the CCIVI report, titled The Compelling Need for Game Changing Influenza Vaccines, doesn’t think so. “We need new influenza vaccines that work for everyone, most of the time.” Furthermore, he feels that overstating current vaccine efficacy could hamper efforts to produce novel vaccines. But what would those new vaccines look like?
In 2012 the FDA approved Flublok®, which is based on cell-based technology, namely a modified baculovirus from insect DNA in which the genetic sequence of hemagglutinin, the key antigen of the influenza virus, is inserted. This new method could offer several benefits over current vaccines, says Bucher, including the ability to produce HA for the vaccine in cell incubators instead of eggs, which can be both expensive and time consuming.
And, because the vaccine uses a genetic sequence rather than inactivated virus grown in eggs or cells, there’s no adaptation process required; a more antigenically similar hemagglutinin could mean better efficacy. “It’s truer to what’s out there in people,” says Bucher, who calls the FDA approval of Flublok, “quite an achievement.”
“Theoretically, you could ramp up production and create unlimited quantities, although the strains included in the vaccine will still have to be based on the decision of the VRBPAC, and the manufacturer can’t start making the vaccine without that recommendation,” says Bucher. And, this is where Palese gets hung up—“Flublok is a new production modality, but ultimately it’s an incremental improvement.”
The So-Called Universal Vaccine
What Palese, and scores of other researchers and companies, have been working on is the so-called universal vaccine—one that creates antibodies to the conserved portions of the HA stalk (those genetic sequences that remain constant across flu strains), not the ever-mutating head. If such a vaccine could be achieved, it could be effective across flu strains, and perhaps boosted only a few times throughout the life cycle.
Palese feels that such a vaccine is not only possible but imminent, pending FDA approval of human trials. “We can identify the conserved domains and we can protect mice, but there are many hurdles to [get to] human trials.” While he understands the concerns of moving to human testing and new vaccine production (very rare side effects may only present in a larger population, not in a small clinical trial, notes Bucher), he is eager to get away from imperfect animal models and start human trials. “In the meantime, tens of thousands of people a year are getting sick, and some are dying,” says Palese.
One of the great fears of vaccine researchers, a largescale novel influenza pandemic in which large portions of the population get very ill, came to fruition in 1957, 1968, and, most recently in 2009. While nightmarish for patients and the healthcare field, the 2009 pandemic “spurred the accumulation of data on epidemiology and risks of influenza,” according to the WHO.
Eliciting Stalk Antibodies
One of the novel findings researchers uncovered was that the pandemic strain of the virus elicited the creation of much sought-after stalk antibodies, and typical seasonal H1N1 influenza virus strains were all but eliminated that year. This gives rise to the theory that vaccinating with inactivated novel, pandemic influenza strains could be one possible way to elicit stalk antibodies. Other methods to obtain multi-strain immunity that are currently being explored include creating headless HA molecules, combining several conserved regions of influenza viruses into one molecule, and activating T cells in combination with antibody producing influenza proteins.
While current vaccine methods and their efficacy across populations are perhaps not ideal, the CCIVI report, as well as Drs. Palese and Bucher, are quick to note that vaccines are by far the best option we have for preventing influenza, and that every person who is eligible should get an annual flu shot. Vaccines have a very good safety record note the researchers, who are both quick to criticize anti-vaccine talk and lobbying efforts.
Just as polio has been eradicated in all areas of the world except for those areas in which vaccination efforts are actively thwarted, flu could be better controlled if more people got vaccinated every year, says Palese. According to the WHO, “Universal vaccination in pediatric groups can reduce disease burden in high-risk children.” In other words, flu vaccines don’t just protect the person getting vaccinated—they can have a group protective effect if enough people get them.
“Vaccines are the best we have,” states Palese. But that doesn’t mean that he won’t be hard at work in the lab trying to find a better way forward.
From genetic engineering and cell culture to regulations and ethics, researchers have a wide range of considerations when experimenting with animal models.
Since the earliest days of medical research, scientists have used model organisms to understand human biology. From ancient Greek analyses of comparative anatomy, to J.S. Haldane’s studies on decompression sickness, to the modern pharmaceutical development pipeline, animals have provided handy surrogates for measuring all types of biological phenomena.
For just as long, researchers have understood that no animal model is a perfect representation of humans. But while vivisection of prisoners may have been acceptable to Aristotle’s contemporaries, modern biomedical scientists must navigate an ethical mine field when working on animals and, especially, when working with human subjects.
At The New York Academy of Sciences (the Academy) conference on “Animal Models and Their Value in Predicting Drug Efficacy and Toxicity,” held September 15-16, 2011, researchers from around the world discussed the ways animal experiments inform—and sometimes misinform—the vast research effort that now underpins the regulation of drugs and toxic chemicals.
The meeting began with a keynote presentation by Jackie Hunter (OI Pharma Partners, Ltd.) who provided a broad overview of the problems facing researchers. While pointing out the numerous shortcomings of animal research, Hunter emphasized that such research remains at the heart of preclinical drug development and chemical toxicity testing: “We are concerned because we are not able to have models that are as predictive as we had hoped, but let’s not forget that…actually animal models have been very valuable in coming up with new medicines for a range of conditions and disorders.”
Regulations and Best Practices
After a set of concurrent workshop sessions, attendees reconvened for a joint discussion on regulations and best practices. Animal studies require careful ethical review in order to evaluate the work against a changing backdrop of rules, guidelines, and ethical norms. Research policy experts from both the U.S. and the European Union reviewed the current regulatory framework, and then an interactive panel discussion allowed audience members to share their own insights on ethical animal experimentation.
At another joint session the meeting’s focus shifted to new animal models, especially ones developed with the latest techniques in genetic engineering and cell culture. One of the most exciting developments in this area is the rapid advance in embryonic stem cell research, and the resulting potential for growing genetically engineered organs of one species inside bodies of another species. That work could lead to much more human-like laboratory models, but it also raises its own set of ethical concerns. “I think that’s an experiment that would, if it worked…potentially produce developing fetuses or…developing embryos with human tissues,” said Roger Pedersen of the University of Cambridge.
Presentations on new technologies for animal studies covered a wide range of approaches, including several talks that emphasized the potential for novel imaging and analytical techniques that could reduce the number of animals that are necessary for an experiment, while simultaneously providing higher-quality data. Other speakers talked about entirely computerized strategies that use sophisticated algorithms to simulate human biology without needing animals at all. While both approaches are clearly advancing, the talks and the subsequent panel discussion emphasized that the field is still in its infancy, and that animal models will remain an essential part of research for the foreseeable future.
It wouldn’t be surprising to find a world-renowned cardiologist at Gustave L. Levy Place in New York City or on First Street in Rochester, Minnesota. Sesame Street, however, might not seem like the logical destination for a cardiologist who has graced the halls of such esteemed research facilities as the Mayo Clinic and Mount Sinai Medical Center (MSMC).
But for someone who has made mentorship a cornerstone of his career, it seems almost fitting that Valentin Fuster, director of Mount Sinai Heart and physician-in-chief of MSMC, has inspired the latest Muppet. Dr. Valentin Ruster, the Muppet character that Fuster inspired, aims to guide children down a healthier path, with the idea that healthier habits learned early can head off later disease (particularly the devastating heart disease Fuster has spent a lifetime studying and treating).
In the first episode of Barrio Sésamo: Monstrous Supersanos (the Spanish equivalent of Sesame Street), Dr. Ruster enlightens Grover on the functions of the heart, while on another, he hosts a game show testing Cookie Monster on the difference between healthy and unhealthy food.
“The other Muppets look up to him as a leader and a role model,” says Fuster. Ironically, this fictional role mirrors Fuster’s real life and his belief in the power of individuals in setting us on the right path. He attributes his success to the presence of people guiding him toward good choices, perhaps in the same way an educational program might steer children to make wiser nutritional choices or exercise more frequently.
“We all need tutors”
“We all need tutors,” he says. “I strongly believe that in my life, in terms of self satisfaction in my career, there’s no doubt that it’s due in large part to the fantastic mentors I had. [We] all had something in common—chemistry. I had the feeling they would do anything for me.”
Spanish-born Fuster, the only cardiologist to receive all four major research awards from the world’s four major cardiovascular organizations, is quick to recall the bright minds that shaped his thinking from medical school to now. While at the University of Barcelona, Fuster met Pedro Farreras, a professor of medicine who wrote the major Spanish textbook on medicine and was considered the top physician in the country. “He really guided me. The critical issue of [our] chemistry was that he had a heart attack at age 42. He told me to be a cardiologist, so I did,” he says.
“A number of advisors gave me advice and I did it without questioning because I had a sense that their experience and care for me was pointing me in the right direction.” Farreras encouraged Fuster to go to England, where he met Harold Sheehan, a pathologist. There, Fuster recalls studying a tissue sample from a patient who suffered a heart attack. The blood clot was riddled with platelets. He asked Sheehan a question that launched his career: What do platelets have to do with the heart attack? Sheenan answered, “We don’t know if it’s the cause or the result. You should study this for your thesis.”
The Role of Platelets in Myocardial Infarction
So Fuster did just that, completing his thesis on the role of platelets in myocardial infarction at the University of Edinburgh, Scotland. He worked closely with another mentor, Desmond Julian, on the first coronary care unit in the world, and became the first cardiologist to go into hematology.
And then he headed to the United States, spending 11 years at the esteemed Mayo Clinic, meeting another mentor, Robert Frye, the chairman of cardiology at the Mayo Clinic. “Occupying high positions as they did,” Fuster recalls of the leadership in Rochester, Minn, “they were always dealing with us, the nobodies. But as people at the top, they believed in and supported the people on the bottom.”
As a mentee, Fuster learned the importance of setting the path for people like himself. For example, he started a program in Spain that identifies young people at ages 15 and 16 who have an interest in science. The program provides grants for these youngsters to spend a month with senior investigators in Madrid, where Fuster leads the Fundacion Centro Nacional de Investigaciones Cardiovasculares Carlos III (equivalent to NHLBI, USA). Once they get a taste of high-level research, the majority of these young scholars pursue scientific career paths, further shaping the future of scientific discovery.
Fuster also made a special point to develop a new Forum for Young Investigators while serving as the president of the American Heart Association. He also started a yearly symposium in Washington DC to teach those interested in the field how to become young investigators.
Succeeding as a Mentor
“When people ask me to be a mentor, the first thing they ask is how they can succeed,” he states. “I define success as development of full satisfaction, which is quite different than how general society defines success. I tell them the whole thing is to do the right thing with the right talent and to be fulfilled.”
This requires soul searching, and staying motivated—by helping others and learning. He teaches his mentees about the four Ts: time, talent, transmit positivity, and tutoring. This includes taking 15 minutes to reflect on your priorities every day and discovering your unique talent. He underscores the importance of measuring your worth by your own standards, and not measuring yourself against your neighbors. And tutoring provides that motivation to others, much the way Dr. Ruster could impact the lives of future adults.
While Fuster acts as a mentor to many individuals, from high school students to early-career doctors and researchers, he sees Sesame Workshop as a way to provide critical advice even earlier in life. Working as a medical advisor to Sesame Workshop since 2006 (with Plaza Sesame, the Latin American version of Sesame Street ), he developed a research protocol that focused on developing healthy habits in 2,000 children between the ages of three and six, giving them 40 hours of training on healthy lifestyles and how to control their emotions.
Always Making an Impact
The work isn’t purely for entertainment; Fuster applies his standard of academic rigor to his work with Plaza Sesame as well. Analysis of 1,000 children, who were randomized to the study approach or a conventional approach, showed that the interventions had a short-term impact on health habits and weight reduction. In addition, the children were able to influence the habits of family members, including parents. The impact of this training will be published in The American Journal of Medicine, and was so successful that the program is now being rolled out to 20,000 children in Columbia, as well as children in Spain and England.
“Sesame was so impressed with the impact that health training can have on children, that they decided to create a Muppet to teach children the importance of health,” Fuster says. Fuster recalls arriving at a meeting at Plaza Sesame and running into his own likeness, albeit in a furry form. “When I got there, a Muppet came up to me and said, ‘I am you.’” “I believe this world will only be changed by young people, and they are the only ones who can take care of this chaos,” he says. “Therefore, I really focus a lot of my efforts on motivation and mentorship and even health for young people.”
Fuster has made a lifetime of being led and leading. Whether researching, helping patients, or working with young researchers, colleagues, or a Muppet character that promotes vegetables instead of cookies, Fuster’s goal is always to make an impact.
First identified nearly a century ago for its essential role in maintaining bone health, vitamin D has recently undergone a renaissance of interest due to the resurgence of vitamin D deficiency and the identification of vitamin D receptors in tissues and cells outside the skeletal system. Indeed, a growing body of evidence indicates that vitamin D has several extraskeletal functions and plays a key role in the immune, cardiovascular, and nervous systems. Furthermore, a growing body of research links vitamin D status to health and vitamin D deficiency to the risk of developing certain diseases, including cancers, multiple sclerosis, type 1 diabetes, rheumatoid arthritis, hypertension, and cardiovascular disease. On September 21, 2012, basic science and clinical researchers gathered to discuss non-classical effects at the Vitamin D: Beyond Bone conference presented by the Abbott Nutrition Health Institute and The New York Academy of Sciences.
Speakers
Daniel D. Bikle, MD, PhD University of California, San Francisco and VA Medical Center
Ricardo Boland, PhD Universidad Nacional del Sur, Argentina
Sylvia Christakos, PhD UMDNJ–New Jersey Medical School
Luigi Ferrucci, MD, PhD National Institute on Aging
David G. Gardner, MD University of California, San Francisco
Martin Hewison, PhD University of California, Los Angeles
Lily Li Mount Sinai School of Medicine
Anastassios G. Pittas, MD Tufts Medical Center
Erica Rutten, PhD Ciro +, Centre of Expertise for Chronic Organ Failure
Igor N. Sergeev, PhD, DSc South Dakota State University
Carol L. Wagner, MD Medical University of South Carolina
Daniel D. Bikle University of California, San Francisco and VA Medical Center
Highlights
Two major forms of vitamin D are important for human health: vitamin D3, which is synthesized in sun-exposed skin, and vitamin D2, which is synthesized in certain plants.
Vitamin D is obtained through diet and sun exposure in the form of inactive precursors. The biologically active form of vitamin D, 1,25-dihydroxyvitamin D, is produced via a two-step enzymatic process, predominantly in the liver and kidneys.
The classical function of vitamin D is to maintain the integrity of the skeleton by modulating calcium homeostasis, but recent studies have uncovered several extraskeletal functions.
The current recommended dietary reference values for vitamin D may be inadequate, especially for those at risk for vitamin D deficiency.
Synthesis and metabolism of vitamin D
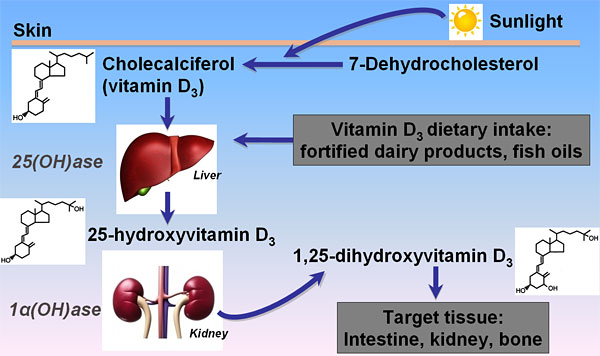
Vitamin D was first identified early in the 20th century as an essential nutrient. It is now recognized to comprise a group of fat-soluble prohormones, substances that are precursors to hormones but have minimal hormonal activity. Two major forms of vitamin D are important to human health—vitamin D2 (ergocalciferol) and vitamin D3 (cholecalciferol)—which differ chemically only in the structures of their side chains. Vitamin D3 is produced in the skin through the action of sunlight (in particular, UVB radiation) on 7-dehydrocholesterol; analogously, vitamin D2 is synthesized in some plants and fungi via photoconversion of ergosterol.
Although sunlight exposure is our main source of vitamin D, it can also be obtained through diet or dietary supplements. Very few foods, however, naturally contain meaningful amounts of vitamin D. Good sources include cod liver oil, salmon, tuna, and other fatty fish, as well as fortified foods, such as milk, yogurt, and orange juice.
Vitamin D metabolism. (Image courtesy of Sylvia Christakos)
Vitamin D obtained through diet, supplements, or sun exposure is biologically inactive and must undergo metabolism to become active. Vitamin D2 and D3 are transported in the blood by vitamin D-binding protein to the liver and enzymatically hydroxylated at carbon 25 to form 25-hydroxyvitamin D (25(OH)D). Although 25(OH)D is still biologically inert, it represents the major circulating form that is measured to assess vitamin D status. The active form of vitamin D, 1,25-dihydroxyvitamin D (1,25(OH)2D), is produced predominantly in the kidney but can also form in a variety of other tissues, including the skin and bone, and in immune cells. Compared with 25(OH)D, 1,25(OH)2D is generally not a reliable indicator of vitamin D status because it has a shorter half-life and its serum level changes in response to calcium, phosphate, and parathyroid hormone (PTH).
Vitamin D mechanism of action
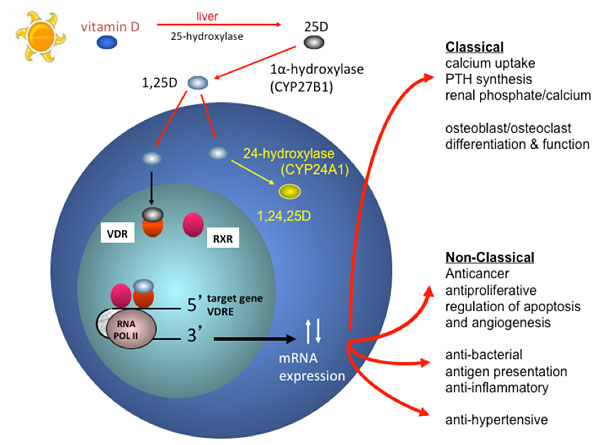
The classical function of the active form of vitamin D is to maintain the integrity of the skeleton by regulating calcium and phosphorus homeostasis. In response to low blood calcium levels, the parathyroid gland secretes PTH, which induces expression of CYP27B1, the enzyme that catalyzes formation of 1,25(OH)2D. This active form binds to the vitamin D receptor (VDR)—which regulates gene expression by binding predominantly to vitamin D-responsive elements in the promoter regions of target genes—stimulating intestinal absorption of calcium and phosphate, the release of calcium from bone, and calcium re-absorption in the kidney.
Classical and non-classical actions of vitamin D: mechanism of action. (Image courtesy of Martin Hewison)
Keynote address: Vitamin D dietary reference intakes
In 2010 the Institute of Medicine (IOM) evaluated health outcomes associated with vitamin D and calcium and proposed updated Dietary Reference Intake (DRI) values reflecting new data on optimal levels of these minerals. The IOM recommended a 25(OH)D serum level of at least 20 ng/mL (50 nM) but considered levels up to 50 ng/mL (125 nM) safe. A 600 IU daily intake of vitamin D is deemed adequate for most people but up to 4000 IU is considered safe. The IOM concluded that 97.5% of the U.S. population have 25(OH)D levels greater than 20 ng/mL and therefore do not need vitamin D supplementation.
Daniel Bikle from the University of California, San Francisco and VA Medical Center gave his perspective on these recommendations in his keynote address. He pointed out that the recommendations are for the general population, not patients, and are based only on studies of vitamin D’s classical effects on bone. Moreover, the IOM based its conclusion that nearly everyone in the U.S. population is vitamin D sufficient on data from National Health and Nutrition Examination Surveys (NHANES), which were weighted toward healthy Caucasians and excluded the population living in the northern part of the country in the winter. Bikle surveyed additional studies that question the adequacy of the vitamin D status in many populations, concluding, “I question the IOM conclusion that 97.5% of the population in the U.S. maintain 25(OH)D levels above 20 ng/ml.”
Bikle also questioned whether the IOM recommendations meet the needs of the elderly, a population that is particularly vulnerable to vitamin D deficiency due to age-related decreases in cutaneous vitamin D production, dietary intake, intestinal absorption, 1,25(OH)2D production, and intestinal response to 1,25(OH)2D. He surveyed data on the relationship between vitamin D status and bone density, mobility, fall rates, and fracture risk and concluded that, “50 nM or 20 ng/ml [may not be optimal] for the elderly individual who’s at the greatest risk of vitamin D deficiency on the one hand and of fractures on the other.”
Bikle recommended that particular subsets of the population be tested for vitamin D deficiency, including women and men over age 65 and 70, respectively; those who are institutionalized; those with dark complexions living in temperate latitudes; those who avoid the sun or dairy products; those with osteoporotic fractures; those with malabsorption; those undergoing bariatric surgery; those with chronic kidney disease; and those taking certain drugs that alter metabolism.
In recent decades researchers have uncovered several non-classical extraskeletal functions of vitamin D. The Vitamin D: Beyond Bone conference explored these, presenting vitamin D’s multifunctional role in immunity, cardiovascular health, cancer, pregnancy, infection, diabetes, cognitive function, and muscle function; its molecular mechanisms of action; and recent changes to nutritional guidelines. The conference encouraged cross-disciplinary dialogue, identified research gaps, and helped to build communities, develop partnerships, and translate basic research findings and epidemiological data into strategies that may promote public health.
Video Chapters 00:01 1. Introduction; The IOM recommendations 16:23 2. Vitamin D deficieny in the elderly 22:07 3. Recommendation adequacy 30:00 4. Who should be tested? 38:58 5. Therapeutic considerations 43:00 6. Summary and conclusions
Non-classical Roles of Vitamin D, Part 1
Speakers
Sylvia Christakos University of Medicine and Dentistry New Jersey (UMDNJ)–New Jersey Medical School
Martin Hewison University of California, Los Angeles
David G. Gardner University of California, San Francisco
Carol L. Wagner Medical University of South Carolina
Highlights
Vitamin D inhibits the growth of breast cancer cells in vitro.
Vitamin D reverses paralysis in a mouse model of multiple sclerosis.
Vitamin D modulates, directly or indirectly, the function of several immune system cells.
Vitamin D may exert a protective effect on the cardiovascular system.
Supplementation with 4000 IU of vitamin D per day appears to be safe and effective for pregnant women.
Vitamin D’s impacts on cancer and multiple sclerosis
In addition to its principal role in the regulation of calcium homeostasis, recent in vitro and animal studies suggest that vitamin D inhibits the growth of breast, colon, and prostate cancer cells and may provide protection against certain immune-mediated disorders, such as type 1 diabetes and multiple sclerosis (MS). Sylvia Christakos from UMDNJ opened the meeting by discussing her research into the molecular mechanisms that underlie its impact on breast cancer and the immune system. Her studies have revealed that 1,25(OH)2D3 inhibits the growth of breast cancer cells in culture, in part by inducing the transcription factor and potential tumor suppressor protein C/EBPα (providing evidence that C/EBPα may be a candidate target for breast cancer treatment).
Christakos also described research demonstrating that vitamin D suppresses the development of experimental allergic encephalitis (EAE), the mouse model of MS. She investigated vitamin D’s effects on a class of helper T cells that produce the inflammatory cytokine IL-17, which has been reported to play a critical role in mediating inflammatory responses and autoimmune diseases, including MS. 1,25(OH)2D3 inhibited the transcription of IL-17 in human CD4+ T cells in vitro and, in in vivo studies in EAE mice, down-regulated IL-17 levels in CD4+ T cells and reversed the onset of paralysis. These findings suggest that inhibition of IL-17 transcription may be one mechanism by which 1,25(OH)2D3 exerts its immunosuppressive effects. “Many of the same genes are present in humans and mice, and they act similarly, so minimally the findings … may suggest mechanisms involving similar pathways in humans that could lead to the identification of new therapies,” Christakos concluded.
Video Chapters 00:01 1. Introduction and overview 04:12 2. Vitamin D’s impact beyond the skeletal system 11:24 3. Vitamin D and breast cancer 18:11 4. Vitamin D and multiple sclerosis 25:32 5. Summary, acknowledgements, and conclusions
Vitamin D in immune function and disease prevention
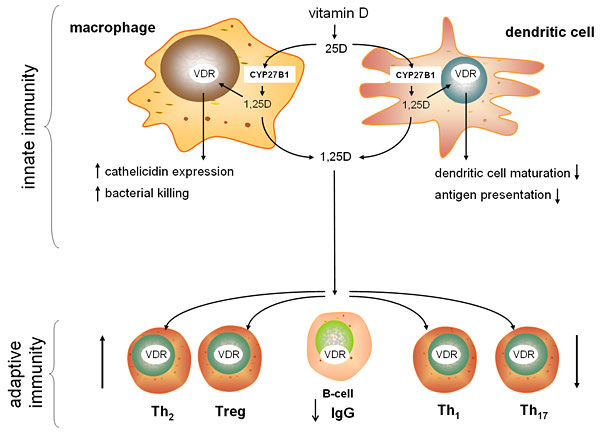
Martin Hewison from the University of California, Los Angeles expanded the discussion of vitamin D’s potent immunomodulatory effects, focusing on cellular machinery that mediates the activities of the adaptive and innate immune systems. Nearly all immune system cells express the vitamin D receptor (VDR); cells of the innate immune system, including macrophages and dendritic cells, also express the enzyme CYP27B1, and thus can activate 25(OH)D locally. Hewison’s research has shown that locally-activated vitamin D in macrophages can trigger the up-regulation of antibacterial proteins, such as LL37 (also known as cathelicidin), and can enhance the killing of bacterial pathogens. Ex vivo studies of human innate immune cells revealed that LL37 expression levels vary with vitamin D status, suggesting that vitamin D deficiency may potentially impair the LL37-mediated response to infection. Cytokines produced by other immune system cells enhance or suppress this vitamin D-mediated immune response by modulating vitamin D metabolism within innate immune cells.
Hewison’s group also discovered a similar intracrine vitamin D system in dendritic cells (DCs)—innate immune cells that primarily deliver bacterial antigen to cells of the adaptive immune system. In this case, locally-activated vitamin D inhibits DC maturation, thereby suppressing antigen presentation and indirectly modulating helper T-cell function. Hewison noted that the active vitamin D produced by DCs, as well as by macrophages, can also act in a paracrine fashion to directly regulate the function of all the various T-cell types by modulating the expression of key T-cell genes. Thus, vitamin D appears to promote immune tolerance and to suppress inflammation and autoimmunity.
Vitamin D affects the activity of macrophages and DCs to modulate adaptive and innate immunity. (Image courtesy of Martin Hewison)
Investigating the link between vitamin D status and autoimmune diseases, such as inflammatory bowel disease (IBD), Hewison’s lab found that inducing short-term vitamin D-deficiency in mice increased the severity of experimentally-induced IBD. Vitamin D-deficient mice exhibited decreased expression of an antibacterial protein in the gastrointestinal tract and increased levels of bacteria in the colon, suggesting an additional antibacterial function for vitamin D and a potential interaction between IBD and the microbiota.
Hewison ended his talk with a look at vitamin D’s immunomodulatory function during pregnancy. Pregnant women tend to be vitamin D deficient. Hewison’s research has uncovered antibacterial and anti-inflammatory actions of vitamin D in placental trophoblast cells, suggesting that vitamin D deficiency may have implications for fetal development, preterm birth, fetal programming of adult disease, and maternal blood pressure. Hewison concluded by suggesting that vitamin D deficiency might impact a wide range of immune-related disorders.
Video Chapters 00:01 1. Introduction 03:00 2. Vitamin D and bacterial killing; Tuberculosis and other disease studies 12:55 3. CYP27B1/VDR interactions; Inflammatory bowel disease and the microbiota 20:18 4. Vitamin D and pregnancy 26:12 5. Summary, acknowledgements, and conclusions
Vitamin D during pregnancy and lactation
Carol L. Wagner from the Medical University of South Carolina continued the theme of vitamin D action during pregnancy and lactation, focusing on the results of her recent vitamin D supplementation trials in pregnant women. Wagner and colleagues have found striking evidence of global vitamin D deficiency during pregnancy, particularly among darker pigmented individuals. Epidemiological studies have revealed that vitamin D deficiency is linked with a higher risk of maternal preeclampsia, an increased risk of gingivitis and periodontal disease in the mother, impaired fetal growth, impaired childhood dentition, and an increased risk of infection by respiratory syncytial virus (RSV).
To determine the most effective safe dose of vitamin D for pregnant women, Wagner and colleagues conducted studies with two different populations of pregnant women, each split into groups receiving 400IU, 2000IU, or 4000 IU of vitamin D3 per day until delivery. The studies found that 4000 IU/day is needed to achieve vitamin D sufficiency (the IOM currently recommends a daily dose of 600 IU/day for the general population). Perhaps more surprisingly, 25(OH)D levels had a direct and positive influence on 1,25(OH)2D levels throughout pregnancy, which has not been observed at any other time in life. No adverse events were attributed to supplementation; in fact, Wagner noted a trend towards lower rates of pregnancy complications in the 2000 IU and 4000 IU groups, compared with the 400 IU group, and towards lower rates of comorbidities during pregnancy with increasing 25(OH)D levels. She concluded that 4000 IU/day is safe and achieves vitamin D sufficiency in pregnant women.
Wagner is now investigating how vitamin D status affects immune function in the mother and her developing fetus and whether maternal D supplementation meets the requirements of both the mother and her nursing infant.
Video Chapters 00:01 1. Introduction; Earlier studies 05:50 2. Epidemiological data; The NICHD supplementation study 11:23 3. The Thrasher Study; Combined study datasets 18:25 4. The Kellogg Project; Supplementation and mother’s milk 23:23 5. Summary and conclusions
Vitamin D and the cardiovascular system
Recent studies suggest that vitamin D may have a protective effect on the cardiovascular system: vitamin D deficiency is associated with high blood pressure and heart enlargement in rats; patients with congestive heart failure have reduced levels of circulating vitamin D; and vitamin D and VDR activation inhibits heart enlargement in rodents. David Gardner from the University of California, San Francisco investigated the molecular mechanisms underlying vitamin D’s cardiovascular effects using mouse models with VDR selectively deleted in either cardiac myocytes or endothelial cells.
Deletion of VDR in myocytes resulted in myocyte enlargement and in expression of genes involved in hypertrophy. Deletion of VDR in mice genetically engineered to accumulate excess fat in myocytes—a condition known as cardiac steatosis that is associated with obesity and diabetes in humans—amplified the pathological effects of cardiac steatosis, suggesting that VDR deletion, and possibly vitamin D deficiency, may sensitize the heart to pathological stimuli. VDR deletion in endothelial cells in vitro impaired the vasorelaxation that normally occurs in response to acetylcholine neurotransmitter. Furthermore, VDR deletion in endothelial cells in vivo resulted in a greater increase in blood pressure in response to the vasoconstricting hormone angiotensin. Taken together, Gardner’s findings suggest that vitamin D and vitamin D analogues may be useful in the management of heart disorders that involve cardiac hypertrophy.
Video Chapters 00:01 1. Introduction 03:21 2. VDR activators and hypertrophy; Liganded VDR and the cardiac myocyte 12:25 3. VDR deficiency and cardiomyophathic stimuli 20:28 4. VDR deletion in murine endothelial cells 25:37 5. Summary, acknowledgements, and conclusions
Non-classical Roles of Vitamin D, Part 2
Speakers
Igor N. Sergeev, South Dakota State University
Erica Rutten, Ciro +, Centre of Expertise for Chronic Organ Failure
Lily Li, Mount Sinai School of Medicine
Highlights
Vitamin D induces apoptosis in fat cells, suggesting that it may one day be useful in the treatment and prevention of obesity.
Vitamin D may help to preserve lung function in patients with chronic obstructive pulmonary disorder.
Vitamin D reduces the erythropoietin requirements of hemodialysis patients with end-stage renal disease.
Vitamin D and apoptosis in obesity
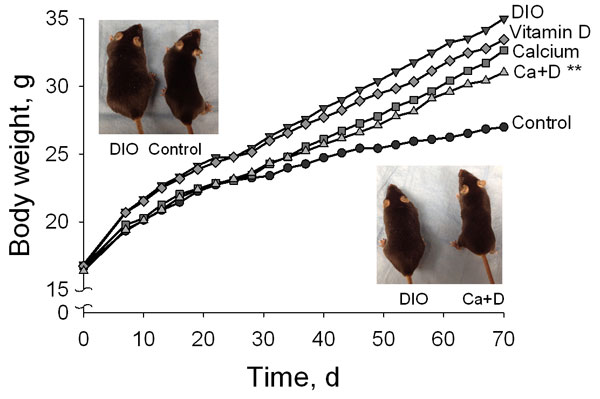
The discussion of the non-classical roles of vitamin D continued with a series of short talks by early career investigators. Epidemiological studies have associated low vitamin D status with an increased risk of obesity. Igor N. Sergeev from South Dakota State University has found that 1,25(OH)2D3 triggers programmed cell death in fat cells by inducing a sustained increase in calcium and by activating calcium-dependent proteases. He noted that inducing apoptosis in fat cells is emerging as a potential strategy for treating and preventing obesity. Using a mouse model of diet-induced obesity, Sergeev showed that supplementation with calcium and vitamin D reduced body fat and weight gain and improved biomarkers of adiposity. Sergeev suggested that vitamin D and calcium might prove useful in the treatment and prevention of obesity.
Vitamin D and calcium supplementation decrease body weight gain in diet-induced obese mice. (Image courtesy of Igor Sergeev)
Vitamin D and lung function
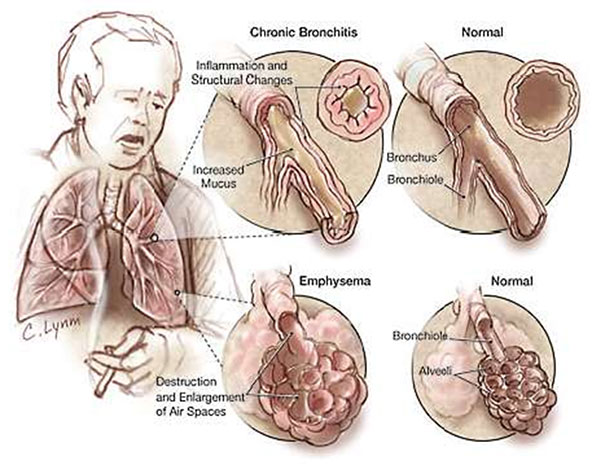
Recent studies have found that vitamin D deficiency is prevalent among people with chronic obstructive pulmonary disease (COPD), an irreversible lung condition that includes chronic bronchitis and emphysema and is primarily caused by smoking. The prevalence of vitamin D deficiency increases with the severity of COPD. Erica Rutten from the Ciro +, Centre of Expertise for Chronic Organ Failure conducted a cross-sectional study of patients with moderate to very severe COPD: 58% were vitamin D deficient. She observed that lung function was positively associated with plasma vitamin D levels, even after correcting for age, gender, and body mass index, and concluded that vitamin D may play a role in lung pathology in patients with COPD.
Vitamin D deficiency may play a role in lung pathology in chronic obstructive pulmonary disease (COPD). (Image courtesy of Erica Rutten)
Vitamin D and chronic kidney disease
Vitamin D deficiency is also common in hemodialysis patients with end-stage renal disease. Lily Li and colleagues from Mount Sinai School of Medicine are conducting an ongoing randomized controlled trial to determine whether correcting vitamin D deficiency decreases vitamin D-deficient hemodialysis patients’ requirements for erythropoietin, a hormone produced by the kidneys that is essential for red blood cell production. The group hypothesized that vitamin D deficiency causes dysregulation of innate immunity, leading to inflammation and altered iron metabolism and contributing to erythropoietin resistance. To date, vitamin D supplementation for 3 or 6 months has safely and effectively increased patients’ 25(OH)D levels and has reduced their requirements for erythropoietin. Ongoing studies aim to determine the immunologic effects of vitamin D repletion in these patients.
Policy and Clinical Applications
Speakers
Anastassios G. Pittas Tufts Medical Center
Ricardo Boland Universidad Nacional del Sur, Argentina
Luigi Ferrucci National Institute on Aging
Highlights
Low vitamin D status is associated with type 2 diabetes, but it remains unclear whether there is a causal relationship between vitamin D and diabetes.
Vitamin D regulates skeletal muscle cell proliferation and function via classical and non-classical molecular mechanisms.
Vitamin D status is associated with several aspects of physical and cognitive function in the elderly.
Vitamin D and type 2 diabetes
Vitamin D supplementation has emerged as a potential strategy for the prevention and management of type 2 diabetes. In his talk, Anastassios Pittas from Tufts Medical Center evaluated whether the available evidence supports a scientifically valid causal association between vitamin D and type 2 diabetes. Using observational data from the Nurses Health Study, Pittas has investigated the association between vitamin D and calcium intake and the development of type 2 diabetes. He found that women who reported the highest levels of calcium and vitamin D intake had a 33% lower risk of developing diabetes compared to those with the lowest intakes of both nutrients. He also observed an inverse relationship between plasma 25(OH)D concentration and risk of incident type 2 diabetes, such that women with higher levels of 25(OH)D had a lower risk of developing diabetes. Moreover, after repeatedly assessing vitamin D status over time in patients at risk for diabetes, he found that progression from pre-diabetes to diabetes declined with increasing concentrations of 25(OH)D.
These and other data suggest that vitamin D is associated with diabetes, but before accepting that a causal relationship exists, “we need to consider alternative explanations,” says Pittas. Because dietary intake of vitamin D and cutaneous synthesis of vitamin D are associated with healthy diets and behaviors, it is difficult to distinguish these potentially confounding factors from the effect of vitamin D itself, says Pittas. Furthermore, vitamin D status is associated with a variety of other factors, many of which are independently associated with diabetes, including physical inactivity, obesity, and dietary patterns. “So, is vitamin D simply a marker of increased risk for type 2 diabetes?” Pittas asked. “In other words, the strong association that we see with type 2 diabetes does not necessarily mean that supplementation would be beneficial.” Therefore, he says, randomized clinical trials are needed to test the hypothesis that vitamin D can modify diabetes risk.
Pittas’s randomized controlled trial—aimed to determine whether vitamin D supplementation would improve glucose homeostasis in patients at high risk for diabetes—showed that short-term vitamin D supplementation improved beta-cell function and attenuated the rise in glycated hemoglobin, a biomarker for diabetes. “In my mind, [vitamin D supplementation] for type 2 diabetes is a promising idea, but is yet unproven,” Pittas concluded.
Video Chapters 00:01 1. Introduction 03:14 2. Biological plausibility; Specificity 05:58 3. Temporal relationship, association strength, dose response, and coherence 11:00 4. Experimental evidence and alternative explanations; Studies 19:40 5. Vitamin D, diabetes, and ethnicity 23:38 6. Summary and conclusions
Vitamin D and muscle function
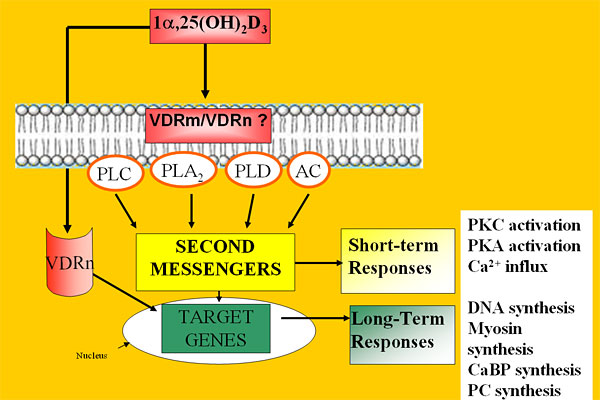
Multiple lines of evidence suggest that vitamin D plays a role in muscle function: muscle weakness and atrophy are common symptoms of vitamin D deficiency; 1,25(OH)2D3 stimulates muscle synthesis in vitamin D-deficient rats; and cellular studies have revealed the presence of the VDR in skeletal muscle. Ricardo Boland from Universidad Nacional del Sur, Argentina reviewed the molecular mechanisms by which 1,25(OH)2D3 regulates skeletal muscle cell proliferation and differentiation. In skeletal muscle cells, vitamin D can function via a classical genomic mechanism, triggering VDR-mediated changes in the expression of genes involved in muscle cell proliferation and differentiation.
Boland has discovered that vitamin D can also function in skeletal muscle cells via a non-classical mechanism involving the activation of transmembrane second messenger systems, calcium influx, and the growth-regulating signaling pathway known as the mitogen-activated protein kinase (MAPK) cascade. 1,25(OH)2D3 stimulates the translocation of VDR from the nucleus to the membrane, where it complexes with a calcium channel protein. At the cell membrane, VDR also forms a complex with the protein Src, which signals upstream of the MAPK cascade. These molecular mechanisms help to clarify how vitamin D regulates skeletal muscle cell growth and contractility and may aid the development of treatments for skeletal muscle disorders.
An overview of the genomic and non-genomic modes of action of 1,25OH2D3 in skeletal muscle cells. (Image courtesy of Ricardo Boland)
Video Chapters 00:01 1. Introduction and background 05:45 2. Calcium influx; Capacitative calcium entry; SOC, TRP, and VDR 13:30 3. INAD-scaffold protein; Src tyrosine kinase; The ERK1/2 pathway 26:20 4. Akt activation; 1,25-dependent Src activation 33:12 5. Summary and conclusions
Vitamin D and Physical and Cognitive Function in Older Persons
Luigi Ferrucci from the National Institute on Aging reviewed the connections between vitamin D and aging. He and others have demonstrated that low 25(OH)D status is associated with mobility limitation and disability in older adults. He explored the basic pathways that may mediate these effects on physical and cognitive function in older persons, focusing on four major aging phenotypes that are related to the biological functions of vitamin D: changes in body composition, imbalances in energy production and utilization, homeostatic dysregulation, and neurodegeneration.
Ferrucci addressed changes in body composition first, showing that low serum levels of 25(OH)D are associated with a higher incidence of obesity and a higher probability of developing obesity, although the mechanisms remain unclear. In muscle tissue, expression of the VDR declines with age, and epidemiological studies have linked low vitamin D levels with loss of muscle strength and mass. These studies reveal some of the ways in which vitamin D may influence body composition.
Next, Ferrucci addressed energy homeostasis. High vitamin D levels are strongly correlated with higher levels of aerobic fitness and peak aerobic capacity, suggesting that low vitamin D levels may give rise to imbalances in energy production and utilization. Furthermore, VDR appears to localize in mitochondria in human blood cells, suggesting that vitamin D may influence energy homeostasis by regulating mitochondrial function.
In terms of homeostatic dysregulation, Ferrucci focused on vitamin D’s anti-cancer and anti-inflammatory actions. At the molecular level, 1,25(OH)2D3 may reduce inflammation by blocking the synthesis and action of prostaglandins and pro-inflammatory cytokines. A systematic review of 219 cross-sectional studies in the literature—designed to evaluate whether vitamin D levels are associated with the risk for autoimmune diseases and whether vitamin D supplementation can modify the course of the diseases—revealed that supplementation with vitamin D may reduce the risk of autoimmune disease. However, randomized controlled trials are needed to establish the clinical efficacy of vitamin D supplementation.
Finally, in terms of neurodegeneration, Ferrucci showed that low levels of vitamin D are associated with an accelerated decline in cognitive function, while higher levels of vitamin D intake are associated with a lower risk of Alzheimer’s disease. Ferrucci has also identified an association between low serum levels of 25(OH)D and symptoms of depression in older men and women.
Ferrucci ended by calling for randomized, controlled intervention studies of vitamin D to determine whether it can slow the development of physical and cognitive disability.
Video Chapters 00:01 1. Introduction 06:02 2. Pathways to cognitive and physical frailty; Changes in body composition 16:24 3. Energy imbalance; Homeostatic dysregulation 20:15 4. Neurodegeneration; Going forward; Conclusions
Panel Discussion
Moderator
Mandana Arabi The Sackler Institute for Nutrition Science
Video Chapters 00:01 1. Does one size fit all? 09:22 2. Sun avoidance; Categorization; Interpreting study data 21:24 3. Prescribing dosage; Fortified foods; Vitamin D2 vs. D3 35:30 4. Vitamin K2; Serum 25-hydroxyvitamin
Open Questions
How do the extraskeletal biological responses observed in vitro and in animal models relate to human disease?
Does the adjustment of vitamin D status correct vitamin D-mediated immune dysfunction?
Does vitamin D status affect the composition of the gut microbiota?
What are the circulating biomarkers of vitamin D-related immune function?
What vitamin D supplementation level should be recommended for pregnant and lactating women?
Is vitamin D supplementation beneficial to vitamin D-deficient patients with chronic obstructive pulmonary disease?
Does vitamin D modify the risk of diabetes?
Can vitamin D supplementation slow down the development of physical and cognitive disability in the elderly?
When measuring vitamin D status, is it more meaningful to measure total 25(OH)D levels or only the fraction of 25(OH)D that is not bound to protein?
Does vitamin D supplementation provide any clinical benefit other than its well-documented effects on bone?
Heike Bischoff-Ferrari is an MD and clinical researcher with specialty board certifications in general medicine, geriatrics, and physical medicine and rehabilitation at the University of Zurich, Switzerland. After her clinical training at the University of Basel, she was a fellow at the Department of Rheumatology, Immunology, and Allergy at the Brigham and Women’s Hospital in Boston and was appointed to the faculty at Harvard Medical School. Bischoff-Ferrari holds an MPH from Harvard School of Public Health and a Doctor of Public Health from the Department of Nutrition at Harvard School of Public Health. Bischoff-Ferrari has an ongoing appointment as a visiting scientist at the Human Research Center on Nutrition and Aging at Tufts University. She holds a primary faculty appointment at the Department of Rheumatology at the University Hospital in Zurich, Switzerland and received a Swiss National Foundations professorship in 2007. In 2008, she became the director of the Center on Aging and Mobility at the University of Zurich. Bischoff-Ferrari’s research focus is improving musculoskeletal health among the senior population with a focus on falls, fractures, and osteoarthritis. One particular interest is to define the role of vitamin D in the context of aging and musculoskeletal health.
Martin Hewison is currently a professor in residence at the David Geffen School of Medicine at the University of California, Los Angeles (UCLA), where his group has an established interest in the role of vitamin D in human physiology, and in particular the interaction between vitamin D and the immune system. Hewison gained his PhD in biochemistry from Guy’s Hospital Medical School, London and spent nine years at University College London. After moving to the University of Birmingham he established the UK’s major vitamin D research group, leading to an appointment as a professor in molecular endocrinology in 2004. In 2005 he joined Cedars-Sinai Medical Center, Los Angeles and moved to neighboring UCLA at the end of 2007. Hewison has published over 160 peer-reviewed manuscripts focused on various facets of steroid hormone endocrinology.
Nabeeha Mujeeb Kazi is managing director of Humanitas Global Development (HGD). She has directed high-profile global food-security initiatives and designed advocacy, public–private partnership, community mobilization, behavior change, and stakeholder engagement programs. Kazi’s team has collaborated with numerous high-profile international organizations including Global Alliance for Improved Nutrition, World Bank, World Health Organization, Save the Children, and UNICEF, among others. Kazi served as Senior Vice President and Partner at Fleishman-Hillard, a global communications firm, and has worked for the Clinton Foundation’s HIV/AIDS Initiative, focusing on Caribbean and African countries, and for the International Maize and Wheat Improvement Center (CIMMYT) in Mexico. Kazi serves on the boards of FINCA International and United Neighborhood Centers of America and has served on several taskforces and committees with partners like Scaling Up Nutrition, Millennium Villages, Feed the Future, and the New York Academy of Sciences. Kazi has dual Master’s degrees in public health and international affairs from Columbia University.
Hawley K. Linke is a senior scientist in the Global Discovery Group at Abbott Nutrition. Her early expertise arose from postdoctoral studies in mitochondrial gene identification at Stanford University Medical School and from her study of human viral gene expression for her PhD from UCLA’s Molecular Biology Institute. She joined Abbott Laboratories Diagnostics Division, Hepatitis-AIDS investigation group, before transferring to Abbott Nutrition. Her contributions to nutrition research include the development and exploitation of industrial-scale expression technologies producing genetically modified and unmodified human proteins for nutritional applications and clinical studies demonstrating therapeutic innovations in infant formula. As an expert in vitamin D, she advises the division on nutritional products to optimize its pleiotropic health benefits. She focuses on technologies for women’s health, neurogastroenterology, and manipulation of the microbiome.
Rosemary E. Riley is senior manager for science programs at the Abbott Nutrition Health Institute, where she is responsible for developing and directing programs that educate health care professionals throughout the world on the importance of nutrition as therapy to improve patient outcomes. While at Abbott, Riley has worked on a variety of nutrition initiatives, including a comprehensive, multidisciplinary medically supervised weight management program, geriatric nutrition, sports nutrition, women’s health—with a focus on bone health—and diabetes. She also has experience in strategic discovery and evaluation of ingredients and technology to address these conditions.
As an academic neonatologist for more than 20 years, Carol L. Wagner has been involved in basic science, translational, and clinical studies. She holds an MD from Boston School of Medicine. She completed both her pediatric residency and neonatalñperinatal fellowship at the University of Rochester. She is a professor of pediatrics and the associate director of the Clinical and Translational Research Center at the Medical University of South Carolina. Wagner’s current research interests are vitamin D requirements during pregnancy and lactation and human milk bioactivity and its effect on gut maturation.
Daniel D. Bikle is a professor of medicine and dermatology at the University of California, San Francisco and co-director of the Special Diagnostic and Treatment Unit of the San Francisco VA Medical Center. He has a long history in the area of vitamin D, performing a number of the initial studies in its metabolism in the kidney and more recently its extrarenal metabolism in the skin. Much of Bikle’s recent research has focused on the molecular mechanisms by which 1,25(OH)2D and its receptor (VDR) regulate gene expression, in particular during normal epidermal differentiation, wound healing, and hair follicle cycling and on the pathologic changes underlying epidermal carcinogenesis. Bikle is also a practicing endocrinologist with particular interest in metabolic bone disease and has written extensively on the interface between the laboratory and clinic with respect to the implications of the recent research in vitamin D function and its impact on patient care.
Ricardo Boland is superior investigator of the National Research Council (CONICET) and director of the Biological Chemistry Laboratories at the Universidad Nacional del Sur, Argentina. Boland obtained his PhD in biochemistry at the University of Missouri–Columbia. He completed postdoctoral training at St. Louis University School of Medicine and the Max-Planck Institute for Medical Research. He served as president of the Argentinean Societies for Biochemistry and Molecular Biology and Bone and Mineral Research. Boland’s research career has been mainly focused on the actions of vitamin D3 on skeletal muscle functions. His major contributions are the identification of the vitamin D receptor (VDR) in this tissue; the characterization of signal transduction pathways involved in the regulation of the Ca2+ messenger system and myogenesis by 1,25(OH)2-vitamin D3; and the demonstration of a functional role of the VDR in these events.
Sylvia Christakos is a professor of biochemistry and molecular biology and at the University of Medicine and Dentistry of New Jersey (UMDNJ)–New Jersey Medical School. Christakos received her PhD from the State University of New York (SUNY) at Buffalo School of Medicine. She completed her postdoctoral training at the Roswell Park Memorial Institute, SUNY Buffalo School of Medicine, Department of Biochemistry and at the University of California at Riverside, California, Department of Biochemistry. Christakos has received continuous funding from the National Institutes of Health (NIH) and National Science Foundation (NSF) for the past 30 years. Her laboratory combines studies related to the functional significance of vitamin D target proteins using animal models with studies related to the molecular mechanism of 1,25(OH)2D3 action.
Luigi Ferrucci is a geriatrician and an epidemiologist who conducts research on the causal pathways leading to progressive physical and cognitive decline in older persons. Ferrucci has made major contributions in the design of many epidemiological studies conducted in the U.S. and in Europe, including the European Longitudinal Study on Aging, the “ICareDicomano Study,” the AKEA study of Centenarians in Sardinia, and the Women’s Health and Aging Study. He was also the principal investigator of the InCHIANTI study, a longitudinal study conducted in the Chianti geographical area (Tuscany, Italy), which looked at risk factors for mobility disability in older persons. Ferrucci has refined the design of the Baltimore Longitudinal Study of Aging to focus more on normal aging, age-associated frailty, and factors associated with exceptionally healthy aging and longevity.
David G. Gardner received an MS in biochemistry and an MD from the University of Rochester. He completed his residency training in Internal Medicine at the Massachusetts General Hospital before moving to the NIH to complete his fellowship in the Combined Endocrinology Training Program. He is the Mount Zion Health Fund Distinguished Professor of Medicine and chief of the Division of Endocrinology and Metabolism at the University of California, San Francisco. His research interests are concentrated in cardiovascular endocrinology, particularly on the regulation of cardiovascular and renal function by vitamin D.
Lily Li is a third-year medical student at the Cleveland Clinic Lerner College of Medicine at Case Western Reserve University. Li completed a one-year post-baccalaureate Intramural Research Training Award Program in immunology at the National Institutes of Health. She is currently pursuing a one-year Doris Duke Clinical Research Fellowship at the Mount Sinai School of Medicine.
Anastassios G. Pittas is an associate professor of medicine at Tufts University School of Medicine, an adjunct associate professor of nutrition and policy at Tufts University Friedman School of Nutrition, Science, and Policy, and a center scientist at the Jean Mayer USDA Human Nutrition Research Center on Aging at Tufts University. He received his MD from Cornell University Medical College, completed his residency at the New York Presbyterian Hospital, and completed a fellowship in endocrinology at Tufts Medical Center before joining the Division of Endocrinology, Diabetes, and Metabolism at Tufts Medical Center. Pittas is the co-director of the Gerald J. and Dorothy R. Friedman New York Foundation for Medical Research Diabetes Self-education Program and the associate director of the Endocrinology Fellowship program. Pittas also holds an MS in clinical research from Sackler School of Biomedical Sciences at Tufts University.
Erica Rutten holds a PhD from Maastricht University in Maastricht, the Netherlands, where she studied amino acid metabolism in patients with chronic obstructive pulmonary disease (COPD). At the Center of Expertise for Chronic Organ Failure (CIRO+) in Horn, the Netherlands, she leads research on body composition, nutrition, and metabolism. Rutten received a research grant from the Dutch Asthma Foundation in 2008. Her interests include malnutrition in COPD, obesity, osteoporosis, vitamin D, and nutritional intake in patients with chronic disease.
Igor N. Sergeev has over 25 years of experience in academic research in biochemistry and nutrition. Sergeev received his PhD from the Institute of Biomedical Problems and a DSc from the Institute of Nutrition, both in Moscow, Russia. As professor of nutritional sciences at South Dakota State University, he directs research program in nutritional biochemistry and molecular nutrition. Sergeev achieved international acclaim for his work on vitamin D metabolism, vitamin D receptors, and calcium signaling. In the last decade, he has been recognized for his research on the role of cellular calcium and vitamin D in the regulation of apoptosis.
Nicholette Zeliadt resides Washington, D.C., where she writes about science for scientists and non-scientists alike. She has a background in biochemistry and nutrition, and a PhD in environmental health sciences from the University of Minnesota. In pursuit of science, she has traveled by ship to the South Pacific Gyre, traversed the Willamette Valley by bike, and encountered 12 of the planet’s 13 climatic zones. She has written for Scientific American, Proceedings of the National Academy of Sciences, BioTechniques, and About.com.
Ferrucci L, Studenski S. Clinical Problems of Aging. In: Longo D, Fauci A, Kasper D, Hauser S, Jameson J, Loscalzo J, eds. Harrison’s Principles of Internal Medicine, 18th ed. New York, NY: McGraw-Hill; 2011:570-588.
Ross AC, Taylor CL, Yaktine AL, Del Valle HB, eds., Committee to Review Dietary Reference Intakes for Vitamin D and Calcium, Institute of Medicine. Dietary Reference Intakes for Calcium and Vitamin D. Washington, DC: The National Academies Press; 2010.
Rafael Pérez-Escamilla works to create and implement public health nutrition programs around the world, but realizes that effective programs must take both a global and local view.
“Good health” is more than a fortuitous platitude; a nutritious diet can help humans plot the course to lifelong wellness—a fact not lost to scientists and public health experts.
But despite efforts of governments and international organizations to equitably provide nutritious food supplies, more than 2 billion people worldwide are still malnourished. Working to further understand the variables at play, Rafael Pérez-Escamilla, professor of epidemiology and public health and director, Office of Community Health, Yale School of Public Health, has spent his career elucidating the roots of nutrition inequities—in addition to paving the way for practical solutions.
“Of course, it’s important to understand the mechanisms of nutrition at the molecular and cellular levels,” Pérez-Escamilla says. “But on the other hand, we have to be able to translate the vast knowledge that we now have into effective public health programs and there is a science to this too.”
Pérez-Escamilla has used the precision of science to track the impact of food insecurity in Brazil. His efforts started on a small scale with an experience-based household survey of some 120 households in the city of Campinas, which quickly grew into a national project. This major undertaking has not only helped the Brazilian government target and monitor the impact of its hunger eradication programs but has also allowed researchers to identify the causes of food insecurity and how this condition affects human development.
Improving Food Security Governance
Since being put into wide-scale use in Brazil, as well as Colombia and Mexico, the United Nations Food and Agricultural Organization has been disseminating the Latin America and Caribbean Food Security Scale, developed under the leadership of Pérez-Escamilla and colleagues, as a standard for the entire region. This is a major step forward for improving food security governance, as the scale allows key stakeholders to accurately measure strides in their efforts against household food insecurity and malnourishment.
“It’s fundamental to be able to compare progress across countries but also for countries to have simple but valid measures that they can trust and build policies around,” says Pérez-Escamilla. With funding from The Bill & Melinda Gates Foundation, Pérez-Escamilla has also recently led the development of a breastfeeding scale up model that encourages new mothers to breastfeed.
Exclusive breastfeeding for six months is one of the most cost-effective maternal-child health interventions, but many barriers have prevented the successful promotion of this optimal infant feeding behavior on a global scale. Pérez-Escamilla aims to overcome these barriers with well-coordinated, intersectoral strategies that engage new mothers in health facilities as well as in community settings.
A Goal to Help All
Whether analyzing the best way to promote breastfeeding or crafting metrics to realistically paint pictures of household food insecurity and malnutrition around the world, Pérez-Escamilla’s goal is to help “all people at all times to have access to sufficient, safe, nutritious food to maintain a healthy and active life.”
This seemingly simple definition of food security, crafted at the World Food Summit in 1996, provides an ideal expectation but in no way drafts a map to that end Understanding Household Food Insecurity Less-developed countries are increasingly inheriting some of the nutritional problems of more developed countries, largely because of the adoption of Western diets and lifestyles. For example, rates of overweight/obesity in some countries in Latin America and the Caribbean are now comparable to those in the United States, Pérez-Escamilla points out.
“In middle income countries food insecurity at the household level is not really related as much to food quantity anymore as it is to dietary quality. A low quality diet among the poor is often times the result of lack of economic or physical access to nutritious foods such as fruits and vegetables and easy access to highly caloric, unhealthy foods,” says Pérez-Escamilla. This reflects the alarming increases in obesity among the poor in these countries.
“Sadly, little is being done to try to apply lessons learned from countries more advanced in this nutrition transition to prevent the same outcome from happening in areas where the transition is less advanced, as in Sub-Saharan Africa. I believe addressing this gap should be a major global health focus.”
Developed Countries Not Immune
In addition, Pérez-Escamilla has learned that people in developed countries are not immune to nutrition-related health inequities. This motivated him to lead a National Institutes of Health-funded study examining the impact of community health workers at improving behavioral, metabolic, and health outcomes among Latinos with Type 2 diabetes in the United States.
“When I came to Connecticut in the early ‘90s and learned about the major health inequities affecting Latinos in the wealthiest state in the country, I decided to reconsider the single focus of my work in developing countries,” says Pérez-Escamilla. “As soon as I started doing this work, I realized how common the root of health inequities is regardless of geographical location. The root is what we now refer to as ‘the social determinants of health’ that calls for well-integrated, multi-level and multi-sectoral solutions developed and governed in strong partnership with affected communities.”
Just as systems biology analyzes the interplay between biological systems, the problems of malnutrition and global health are also complex. “Global health is local health. I understand global as a complex system and local as the cells that form the system. As a result of globalization, local communities, or the cells, are strongly interlinked with each other both within regions and countries and across countries and global macroregions,” says Pérez-Escamilla.
“If the architecture of global health governance continues to be fundamentally inequitable, then the ultimate global health goal of attaining ‘health for all’ regardless of where a human being is born becomes impossible to achieve.”
About the Author
Marci A. Landsmann is a medical writer in Philadelphia.
Academy member Chinua Akukwe answers the “call to duty” as he uses his public health expertise to combat the spread of HIV/AIDS, specifically in Africa.
Published April 16, 2012
By Diana Friedman
Chinua Akukwe, professorial lecturer in the Departments of Global Health and Prevention and Community Health in the George Washington University (GWU) School of Public Health and Health Services and former chair of the Technical Advisory Board of the GWU Africa Center for Health and Human Security, has been appointed to the independent Global Advisory Group on Funding Priorities for UNITAID. UNITAID is dedicated to scaling up access to treatment for HIV/AIDS, malaria, and tuberculosis by leveraging price reductions for quality diagnostics and medicines and accelerating the pace at which these are made available. Since 2006, UNITAID has committed over U.S. $1.5 billion to support projects in 94 countries.
“This appointment is a call to duty during one of the most important periods in global health and financing for international development,” says Akukwe. “UNITAID, with its focus on innovative mechanisms for scaling up access to medicines and other public health goods, can play a more significant role in leveraging scarce resources to reach more individuals and families in need,” he adds.
Akukwe is an expert on the global response to HIV/AIDS, with a particular focus on Africa. He developed the “Communicable Diseases Guidelines” of the Africa Development Bank that established HIV/AIDS, malaria, and tuberculosis as priority health conditions. He also developed the “Strategic Framework for the Implementation of Universal Access to HIV/AIDS, Malaria and Tuberculosis” for the African Union Commission, which was subsequently approved by the African Council of Health Ministers.