While the development of vaccines against infectious diseases has had a profound impact on life expectancy, there remain many resistant and emerging infections for which no effective vaccines are available, such as malaria, HIV, and Zika. Recent advances in biotechnology and our understanding of human immunity hold great promise for conquering new diseases. For example, advances in structural biology allow for the discovery of new antigens that can target broad viral families, such as influenza, or complex parasites like malaria. Novel clinical trials for maternal immunizations have shown encouraging results for reducing dangerous diseases in newborn infants. Furthermore, recent progress in DNA- or RNA-based vaccines holds promise for inexpensive and fast production, which is especially favorable for responding to emerging epidemics. Learn more about recent breakthroughs in vaccine development in this summary of our May 20, 2019 symposium, which gathered the world’s leaders in vaccine development.
Symposium Highlights:
Emerging infectious diseases can be treated quickly with a passive vaccine containing human monoclonal antibodies isolated from the blood of an infected patient.
Targeting multiple stages of the malaria life cycle is a promising strategy for the development of a successful vaccine targeting this complex parasite.
Clinical trials show promise for maternal immunizations in protecting newborn infants from respiratory syncytial virus (RSV) and Group B streptococcus.
A vaccine containing the influenza hemagglutinin (HA) fusion protein without the head domain can elicit protection against a broad group of influenza viruses.
Synthetic DNA and mRNA vaccines are simple to manufacture and show promise for treating a wide range of diseases, including Ebola, HIV, Zika, influenza, and malaria.
A promising new adjuvant, AS01, has contributed to breakthrough vaccines for Malaria, tuberculosis, and shingles.
Speakers
James E. Crowe, Jr., MD Vanderbilt University Medical Center
New Approaches for Understanding the Immune System for Vaccine Development
Speaker
James E. Crowe, Jr. Vanderbilt University Medical Center
Human Antibodies and Repertoires for Emerging Infectious Diseases
James Crowe, of Vanderbilt University Medical Center, discussed his lab’s work developing treatments for emerging infectious diseases using monoclonal human antibodies. “Antibodies essentially are a passive vaccine,” explained Crowe. Currently, it takes about two years to develop a vaccine for an infectious disease agent, which is not quick enough for outbreak response. Therefore, Crowe argues that antibodies are the “most appropriate public health measure for most emerging infections.” Crowe’s group is working on two strategies for developing human antibody drugs: one focuses on speed, whereas the other aims to develop broad antibodies ahead of an outbreak.
The Rapid Rational Antibody Design and Delivery (RRADD) project uses ultra-fast techniques to respond to a specific outbreak in the moment. They recently used Zika as a test case. Starting with a blood sample from a surviving patient, their facility used single-cell RNA-sequencing to produce a list of antibody genes within a day. These antibodies were quickly produced and then tested in a high-throughput real-time cell culture system to assay for protection against Zika infection. Leading candidates were tested in mouse and primate models, leading to the discovery of protective antibodies within 78 days.
Illustrations of antibody (Ab)- antigen (Ag) complexes for human monoclonal antibodies (mABs) recently discovered in the AHEAD100 project.
The second strategy is the Advanced Human Epidemic Antibody Defenses (AHEAD100) project, a methodical approach that aims to develop antibodies for the 100 most likely infectious diseases ahead of any future outbreaks. Interestingly, they found broad antibodies that work across viruses of a related class, such as noroviruses, alphaviruses, and flu.
Taking on the Big Challenges Facing Novel Vaccine Development
Adrian Hill University of Oxford
Wayne Koff Human Vaccines Project
New Generation Malaria Vaccines
Adrian Hill from the University of Oxford presented his work on the development of a malaria vaccine. Malaria causes 500,000 deaths each year, but developing an effective vaccine is challenging. “Even if you get a good antigen, you need remarkably high immunogenicity,” Hill explained. Therefore, Hill’s group aims to develop a vaccine that targets multiple stages of the malaria parasite life cycle.
In the first stage, mosquitos introduce malaria sporozoites into a human host. Hill’s group and others have been developing vaccines that combine malaria antigens with virus-like particles to induce antibody production against sporozoites. Hill and colleagues are developing R21, a more potent version of the RTS,S vaccine currently in Phase III trials. In R21, 100% of the molecules encode the sporozoite antigen. Studies show that this formulation allows for a lower dose, as antibody titers are indistinguishable between a 10 µg dose of R21 and a 50 µg dose of RTS,S. Furthermore, R21 shows a more durable response, with higher titers at six months versus RTS,S. By 2020, they expect efficacy results from the first Phase IIB trial.
As the malaria life cycle progresses, sporozoites infect liver cells, where the parasite matures. “[To target] the liver stage, you need T-cells” said Hill. Inducing T-cells requires a viral vector approach. Research on mice and clinical studies from Hill’s group show that the ME-TRAP antigen viral vector can induce high levels of resident memory T-cells in the liver. There are ongoing field clinical trials for this vaccine.
The Future of Vaccine Development
Wayne Koff, the president and CEO of the Human Vaccines Project, described the nonprofit’s research decoding the human immune system. Vaccines for complex infectious and non-communicable diseases such as HIV, tuberculosis, and cancer have been difficult to develop. Koff believes that a better understanding of human immunity is essential for accelerating vaccine development for these diseases.
One strategy is to investigate why some people respond to vaccines and infections much better than others. “If we can understand this, we can get at the pathogens we haven’t been able to tackle,” said Koff. Recent developments in single cell multi-omics allow for an in-depth analysis of an individual’s immune system. A growing body of evidence suggests that immunity biomarkers at baseline can predict an individual’s response to immunization. Researchers performed single cell RNA-sequencing on innate immune cells before immunization and successfully identified biomarkers predictive of the response to the Hepatitis B vaccine. By integrating all of the pre-immunization data, investigators could build biostatistical models that accurately predicted final antibody titers, while revealing pathways that may be involved in the response mechanism.
This data suggests that “we all have an immune set point,” said Koff, which leads to the opportunity to modulate this set point before immunization to improve outcomes. Furthermore, smaller trials that account for individual variability and assay predictive signatures may be more effective than standard large vaccine efficacy trials.
Kathrin Jansen from Pfizer discussed recent advances in maternal immunization. Infants under six months are the most vulnerable to infection, but most vaccines are not available at this early stage of life. Furthermore, “20% of stillbirths seem to be associated with an infectious disease,” said Jansen. Active antibody transfer from mother to baby during pregnancy is an essential mechanism for protecting infants from infectious diseases. The goal of maternal immunization is to enhance maternal antibody levels to further protect newborns. Jansen explained that these vaccines could either “augment pre-existing antibody responses or induce a de novo response” to infections the mother has not yet been exposed to.
Jansen presented recent findings for maternal vaccines targeting respiratory syncytial virus (RSV) and Group B streptococcus bacteria, two infections that are especially deadly for newborn infants. In a recent Phase I/II trial, the Group B streptococcus vaccine induced high levels of antibody titers for up to six months in healthy adults, giving confidence to move forward for testing in pregnancy. Recent structural biology studies of RSV identified a metastable form of the viral fusion protein. With this form in mind, a screen for vaccine candidates revealed molecules that were 30 times more powerful than the current licensed prophylactic antibody in rodents. Data from a Phase I/II study will be available later this year.
Protecting Infants from RSV via Maternal Immunization
Greg Glenn, of Novavax, presented recent progress on the development of an RSV maternal vaccine. RSV is the leading cause of hospitalization of infants in the United States. While the Pfizer version of the vaccine, described by Kathrin Jansen, resembles the metastable prefusion form of the viral fusion protein, the Novavax version targets an earlier, stable form known as the prefusogenic form. This vaccine contains a near full-length fusion protein, but with deletions in a furin cleavage site. “These deletions fix the protein structure, and that allows it to be very stable,” Glenn explained. Through stabilizing the prefusogenic form, the virus is prevented from successfully infecting cells, which allows the vaccine to be produced in culture with higher yields. Furthermore, all antibodies that target the metastable prefusion form also target the prefusogenic form. Immunization with the Novavax vaccine induces antibodies to a variety of viral epitopes, which are also transferred to the infant.
Schematic showing the different forms of the fusion (F) protein of the RSV virus.
Currently, Novavax is running a worldwide Phase III randomized placebo-controlled trial to evaluate protection of infants against RSV with their maternal vaccine. The vaccine was given “to immunized mothers in third trimester, and we monitored infants intensely for six months,” explained Glenn. The trial showed a 40% reduction in their primary endpoint, which was medically significant RSV lower respiratory tract infection at 90 days old.
Next Generation Vaccines to Eliminate Congenital Cytomegalovirus: We are halfway there
Sallie Permar, of Duke University, shared her work developing an effective vaccine for congenital cytomegalovirus (CMV), which is the most common congenital infection and cause of birth defects worldwide. Developing a vaccine has been tricky, as it’s unknown exactly what maternal immune responses are protective against congenital CMV transmission. Permar’s group is investigating these questions with a novel, non-human primate model as well as data analysis from previous vaccine trials.
Permar and colleagues infected seronegative rhesus monkeys with CMV at the beginning of pregnancy. “We used a model of severe pathology with maternal CD4+ T-cell depletion followed by an intravenous inoculation to ask whether antibodies alone could be protective against congenital CMV transmission,” explained Permar. Data from a small group of animals suggests that treatment with passive antibodies from donor plasma prior to inoculation prevents fetal transmission. This result indicates that stimulating potent antibody responses could be a promising route to an effective maternal CMV vaccine.
Previous trials of a vaccine containing glycoprotein B, the main fusion protein of the virus, have shown partial effectiveness. Permar’s group probed the trial data to investigate what immune responses correlate with protection against CMV in infected versus uninfected vaccine recipients. “The ability of vaccine-elicited antibodies to bind to glycoprotein B-transfected cells was higher in uninfected vaccinees,” said Permar, suggesting that eliciting antibodies that bind to glycoproteins is a promising vaccine target. Furthermore, the infected group of vaccine recipients was still protected against specific CMV strains, suggesting that a broader immunogen might be more effective.
Guiding Vaccine Candidates: Antibodies That Can Neutralize Influenza and Malaria
Ian Wilson, from the Scripps Research Institute, shared his recent work investigating the structural biology of antibodies to guide vaccine candidates for influenza and malaria. Wilson’s group aims to “design immunogens or even small molecules from the structural information about how antibodies bind.”
Human antibodies that neutralize a broad range of flu subtypes have been characterized in the last ten years. Interestingly, the broadest antibodies bind to the less immunogenic “stem” domain of the influenza hemagglutinin (HA) fusion protein, rather than the “head” domain. “We are using this information to try to think of novel vaccines,” said Wilson. “If we chop off the immunogenic head, then we can target the response against the stem.” Indeed, a recently developed headless HA construct elicited protection against all influenza A group 1 antibodies in mice and monkeys.
Wilson’s group has also probed the structural biology of human antibodies elicited in recent RTS,S malaria vaccine trials. Cryo-EM revealed the structure of antibodies binding to the circumsporozoite protein (CSP) of malaria: the antibodies spiral all the way around the NANP peptide repeats of the protein. Furthermore, antibodies in the spiral bind in close proximity, and often, somatic mutations strengthen these homotypic contacts for a more stable spiral. Future work will explore the relevance of this spiral structure for vaccine purposes.
Synthetic DNA Approaches for Difficult Infectious Disease Targets
David Weiner, of the Wistar Institute, presented recent findings on the development and efficacy of synthetic DNA vaccines. DNA vaccines are “very consistent, very simple to manufacture, temperature stable,” and allow for local transfection without systemic expression, explained Weiner. Recent early stage clinical trials have shown promising results for using synthetic DNA vaccines as immunotherapy to treat human papillomavirus (HPV)-related cancers. Synthetic DNA is also promising for treating emerging infectious diseases. Wiener discussed three examples, Ebola, MERS, and Zika, where prophylactic treatment with synthetic DNA induced a 95%–100% response rate, and transmission into the clinic occurred in only 7–15 months.
Weiner also discussed his group’s work developing a DNA-encoded monoclonal antibody (dMAb) platform. Muscle or skin tissue “is transfected and becomes a factory for expression of the protein. The idea is getting [the antibody] secreted into the bloodstream at detectable levels,” said Weiner. They have developed dMAbs targeting Ebola, HIV, and Zika that induce robust antibody expression and viral protection in animal models. For HIV, multiple dMAbs can be delivered at one time, which has been shown to induce broad neutralizing titers against nine HIV subtypes in non-human primates.
Weiner and collaborators are also working to engineer DNA cassettes that encode self-assembling nanoparticles directly in vivo. Nanoparticles targeting HIV showed improved immune responses versus the monomeric form: “It’s dose sparing, it’s much faster seroconversion and much higher titers, and it elicits very good CD8+ T-Cells,” Weiner said.
mRNA Vaccines: A New Era in Vaccinology
Drew Weissman, of the University of Pennsylvania, discussed recent advances in the development of mRNA vaccines for infectious diseases. Why use RNA? In theory, the cost of mRNA production would be much less than that of protein, which requires large-scale cell culture followed by purification that differs for every protein. Weissman’s group developed a platform using nucleoside-modification and purification techniques to optimize mRNA structures that induce high and long-lived translation when delivered within lipid nanoparticles to peripheral sites.
Mice vaccinated with the A/Cal/7/2009 HA mRNA vaccine challenged with the distant flu virus H5N1 showed full protection. These results suggest immunization with HA mRNA could result in a universal flu vaccine.
Weissman discussed mRNA vaccines developed with their platform targeting influenza, HSV-2, HIV, and malaria, which have all shown promising results in animal models. For influenza, a single immunization with an mRNA vaccine coding for the hemagglutinin (HA) fusion protein in mice resulted in titers 50 times higher than the current FDA approved vaccine. As a mechanism of action, they found that the lipid nanoparticles used for vaccine delivery induce T- follicular helper cells, which drive long-term immune memory and are “critical in the induction of potent antibody responses,” explained Weissman. Furthermore, their mRNA vaccines induce responses to subdominant epitopes in the presence of dominant epitopes, which isn’t seen with whole proteins. This response is useful because subdominant epitopes, such as the HA stem domain, can be broadly cross-reactive across viral subtypes. Vaccinated mice challenged with distant flu viruses were fully protected, “suggesting that using a full HA could give you a universal vaccine,” said Weissman.
Transforming New Technologies into Vaccines: Genomics, Adjuvants and Self-Amplifying RNAs
Rino Rappuoli, of GlaxoSmithKline, shared how new technologies will allow us to conquer new diseases. Recent advances have allowed for major improvements in reverse vaccinology — using human genomics and structural biology to discover new antigens and instruct vaccine design. “Today we have the tools of synthetic biology,” said Rappuoli. At GSK, “we are using self-amplifying mRNA instead of simple mRNA. We use the replicon of the alphavirus to amplify the RNA and give a better response.” Nucleic acid vaccines work well in animal models, and the challenge now is testing whether it will work well in humans.
Rappuoli also discussed encouraging new advances in antigen delivery using nanoparticles or Generalized Modules for Membrane Antigens (GMMA). While self-assembling natural nanoparticles have been around for years, fully synthetic nanoparticles have only recently been designed. “We are going from mimicking nature to completely computationally designing vaccines,” explained Rappuoli. GMMAs consist of outer membrane vesicles from bacteria, which are engineered to release these vesicles in large quantities with the desired antigens. Rappuoli also highlighted recent developments in adjuvants, substances within vaccines that enhance the immune response to antigens. A promising new adjuvant, AS01, has contributed to breakthrough vaccines for Malaria, tuberculosis, and shingles. Moving forward, Rappuoli aims to use these new technologies to target vaccines for the elderly, emerging infections, and antimicrobial resistance.
Climate change is a growing threat with global impact. Shifts in the climate present special challenges for urban areas where more than half of the world’s population lives. New York City residents, for example, are already feeling the effects through recurrent flooding in coastal communities, warmer temperatures across all five boroughs, and strains in the city’s infrastructure during heavy downpours and extreme weather events. As a result, cities like New York require the best-available climate science to develop tangible policies for resilience, mitigation, and adaptation.
On March 15, 2019, climate scientists, city planners, and community and industry stakeholders attended the Science for Decision-Making in a Warmer World summit at the New York Academy of Sciences to discuss how cities are responding to the effects of climate change. The event marked the 10th anniversary of a successful partnership between the New York City Panel on Climate Change (NPCC), the City of New York, and the New York Academy of Sciences. Established in 2008, the NPCC has opened new frontiers of urban climate science to build the foundation for resiliency actions in the New York metropolitan region.
Learn about the NPCC’s latest research findings and their implications for New York City and other cities seeking to identify and mitigate the effects of climate change in this summary.
Meeting Highlights
NPCC research provides tools to inform and shape climate change resilience in New York City and other cities around the globe.
Shifts in mean and extreme climate conditions significantly impact cities and communities worldwide.
Cities can move forward by adopting flexible adaptation pathways, an overall approach to developing effective climate change adaptation strategies for a region under conditions of increasing risk.
There is a growing recognition that resilience strategies need to be inclusive of community perspectives.
Speakers
Dan Bader Columbia University, New York City Panel on Climate Change
Jainey Bavishi New York City Mayor’s Office of Recovery and Resiliency
Sam Carter Rockefeller Foundation
Alan Cohn New York City Department of Environmental Protection
Kerry Constabile Executive Office of the UN Secretary General
Susanne DesRoches New York City Mayor’s Office of Recovery and Resiliency
Alexander Durst The Durst Organization
Sheila Foster Georgetown, New York City Panel on Climate Change
Vivien Gornitz Columbia University, New York City Panel on Climate Change
Mandy Ikert C40 Cities Climate Leadership Group
Klaus Jacob Columbia University, New York City Panel on Climate Change
Michael Marrella New York City Department of City Planning
Richard Moss American Meteorological Society
Kathy Robb Sive, Paget, and Riesel
Seth Schultz Urban Breakthroughs
Daniel Zarrilli, PE New York City Office of the Mayor
Climate Change, Science, and New York City
Speakers
Alan Cohn New York City Department of Environmental Protection
Susanne DesRoches New York City Mayor’s Office of Recovery and Resiliency
Alexander Durst The Durst Organization
Michael Marrella New York City Department of City Planning
Daniel Zarrilli (keynote) New York City Office of the Mayor
James Gennaro (panel moderator) New York State Department of Environmental Conservation
Keynote: Preparing for Climate Change — NPCC and Its Role in New York City
Daniel Zarrilli, of the New York City Office of the Mayor, gave the first keynote presentation. In addition to outlining NPCC history, he emphasized the meaning of NPCC to the city. NPCC has provided the tools to inform policy since before Hurricane Sandy in 2012. Because of NPCC, Zarrilli stated, people now know that the waters around New York City are rising “twice as quickly as the global average” and that climate change will affect communities disproportionately. The city can and will take on the responsibility to protect those who are most vulnerable. Zarrilli highlighted steps the Mayor’s Office is taking: fossil fuel divestment, bringing a lawsuit against big oil for causing climate change, and launching a new OneNYC strategic plan to confront our climate crisis, achieve equity, and strengthen our democracy. He concluded by saying that with “8.6 million New Yorkers and all major cities watching,” NPCC is providing the best possible climate science to drive New York City policy.
Panel 1: NPCC and Its Role in New York City
How are NPCC findings used in developing resiliency in New York City?
The first panel was moderated by William Solecki of Hunter College Institute for Sustainable Cities – City University of New York, and featured three city representatives, Susanne DesRoches, of the New York City Mayor’s Office of Recovery and Resiliency; Michael Marrella, of the New York City Department of City Planning; Alan Cohn, of the New York City Department of Environmental Protection; and one industry stakeholder, Alexander Durst, of the Durst Organization.
DesRoches noted that the NPCC research has made possible a proliferation of guidelines regulating building design in the city. In fact, the New York City Climate Resiliency Design Guidelines, released the same day that the panel took place, provide instruction on how to use climate projections in the design of city buildings. The Department of City Planning also uses NPCC data in its Coastal Zone Management Program to require that coastal site developers to disclose and address current and future flood risks. Marrella added that NPCC research tools allow public and private stakeholders to make informed decisions on how to shape policy. NPCC methods and approaches are also being used climate data is also being used for New York State and national projections.
Panelists also addressed how New York City’s mitigation goals enable resilience in the face of climate change challenges. DesRoches pointed to the city’s aggressive climate targets, including an “80% [emissions] reduction by 2050,” and a goal to limit temperature increase to 1.5°C, as targeted by the Paris Agreement (UN Climate Change 2015). She gave two examples of adaptations that align with the City’s mitigation goals: adapting high “passive house” and green building standards for a reduced carbon footprint; and diversifying how the city receives energy, including the development of a renewable energy grid. Cohn added that the Department of Environmental Protection aims to free up capacity in water conservation and implement the use of methane as an energy source. With resilience in mind, Durst stressed that energy models should be uniform and based on the future, not just today.
Further Readings
Zarrilli
Wallace-Wells D.
The Uninhabitable Earth: Life after Warming
New York: Tim Duggan Books; 2019
Panel 1
Rosenzweig C, Solecki W, González JE, Ortiz L, et al.
Panel 2: Latest Findings from the New York City Panel on Climate Change
What types of information are the most useful?
The second panel was moderated by Julie Pullen of Jupiter Intelligence, and featured four NPCC members who presented the latest NPCC3 report findings: Vivien Gornitz, Klaus Jacob, and Daniel Bader of Columbia University; and Sheila Foster, of Georgetown Law.
The latest NPCC3 findings confirmed climate projections from the 2015 report as the projections of record for New York City planning and decision-making. For example, by the end of the century, “ocean levels will be higher than they are now due to thermal expansion; changes in ocean heights; loss of ice from Greenland and Antarctic Ice Sheets; land-water storage; vertical land movements; and gravitational, rotational, and elastic ‘fingerprints’ of ice loss,” said Gornitz. Under the NPCC’s new Antarctic Rapid Ice melt (ARIM) scenario, there could be up to a 9.5 ft. increase in sea level rise by 2100 at the high end of the projections. The new report advises that levies or raised streets might reduce the effects that sea level rise will have on New York City’s coastline.
Vulnerability to climate change varies by neighborhood and socioeconomic status. Foster presented a new three-dimensional approach to community-based adaptation through the lens of equity: distributional, contextual, and procedural. Distributional equity emphasizes disparities across social groups, neighborhoods, and communities in vulnerability, adaptive capacity, and the outcomes of adaptation actions. Contextual equity emphasizes social, economic, and political factors and processes that contribute to uneven vulnerability and shape adaptive capacity. Procedural equity emphasizes the extent and robustness of public and community participation in adaptation planning and decision-making.
Echoing Mayor Bloomberg’s sentiment that “if you can’t measure it, you can’t manage it,” Jacob presented the proposed NPCC New York City Climate Change Resilience Indicators and Monitoring system (NYCLIM). Through the new proposed NYCLIM system, NPCC recommends climate, impact, vulnerability, and resilience indicators for the City’s decision-making processes.
Further Readings
Panel 2
Rosenzweig C, Solecki W, González JE, Ortiz L, et al.
Cities as Solutions for Climate Change and Closing Remarks
Keynote Speaker and Panelists
Jainey Bavishi New York City Mayor’s Office of Recovery and Resiliency
Sam Carter Rockefeller Foundation
Kerry Constabile Executive Office of the UN Secretary General
Seth Schultz Urban Breakthroughs
Mandy Ikert (keynote) C40 Cities Climate Leadership Group
Richard Moss (panel moderator) American Meteorological Society
Keynote: Role of Cities in Achieving Progress
Mandy Ikert, of C40 Cities Climate Leadership Group, gave the second keynote presentation. The Future We Don’t Want, a study recently released by C40, the Urban Climate Change Research Network (UCCRN), and Acclimatise found that billions of urban citizens are at risk of climate-related heat waves, droughts, floods, food shortages, and blackouts by 2050 (UCCRN 2018). Cities are situated at the forefront of these effects and urgently need to respond. Ikert stated that “we live in an urbanizing world,” where 68% of the world’s population will be living in cities by 2050, up from approximately 54% today.” Ikert stressed that “mayors and city agencies are directly accountable to their constituency” in order to protect and preserve their lives and livelihood. She also urged cities to reach out to researchers to obtain accurate modeling for extreme events. Cities have the potential to account for 40% of the emissions reductions required to align with the Paris Agreement’s goal to limit temperature rise to 1.5°C (UN Climate Change 2015). Therefore, the way a city responds to climate change, Ikert said, determines how livable and competitive it will be in the future.
Panel 3: City Stakeholders and Beyond
How can knowledge networks and city networks improve interactions to achieve climate change solutions?
The final panel was moderated by Richard Moss of the American Meteorological Society, and featured Corinne LeTourneau, of the North America Region, 100 Resilient Cities; Kerry Constabile, of the Executive Office of the UN Secretary General; Jainey Bavishi, of the New York City Mayor’s Office of Recovery and Resiliency; and Seth Schultz, of Urban Breakthroughs, spoke about the enormous value and knowledge of stakeholders.
In this session, all of the participants highlighted that many cities are playing a critical role in meeting the challenge of climate change, both through efforts to reduce their own greenhouse gas footprints, and to update infrastructure and programs to meet the needs of their citizens as climate change impacts occur.
Panelists discussed how finances are a major challenge to addressing climate change. For example, Constabile noted that a small percentage of megacities in developing countries have credit ratings. This lack of “creditworthiness” hinders cities from raising their own bonds and attracting private investment, both of which are significant sources of funding for climate-related projects. Schultz suggested that private money may jumpstart some climate resiliency and adaptation efforts, and stated that eight of ten of the world’s largest countries are funding research on climate change. LeTourneau and Schultz identified that without the climate data to assess risks, money will not be directed to the areas of greatest need. LeTourneau highlighted the importance of describing how climate change affects risks and “the bottom line” in a way that decision makers and citizens find compelling and relatable.
Panelists also highlighted that climate does not have boundaries, but government bodies do. As Bavishi pointed out, New York City is lucky that climate change adaptation has been codified into law. Chief resilience officers are retained even after city funding is spent, so continuity is in place. City governments around the country and the globe are following suit, but as the panelists pointed out, these ideas should spread more widely.
Closing Remarks
NPCC member Michael Oppenheimer remarked that the NPCC offers a “local picture at granular level with the best possible science.” Hurricane Sandy taught the City about its vulnerability and drove research on flood tides and rising coastal tides. With the 2010 NPCC report, he said, a firm research agenda was drafted that shifted the City’s view of climate change to resiliency. Oppenheimer stressed that NPCC science is useful for policy and praised New York City for utilizing NPCC data in policy decisions. In closing, Oppenheimer said that dissemination assures that communities worldwide are able to use NPCC data.
Further Readings
Ikert
Rosenzweig C, Solecki W, Romero-Lankao P, Mehrtotra S, et al.
Whereas: Global issues are often felt most deeply at the local level, and in the face of worldwide threats to our environment, infrastructure, and economy, cities have the power and responsibility to lead our planet in the right direction. After Hurricane Sandy, when the devastating effects of climate change hit home for far too many of our residents, New York City reaffirmed our commitment to building a sustainable path forward. On the 10th anniversary of its founding, it is a great pleasure to recognize the New York City Panel on Climate Change for its exceptional leadership in this work.
Whereas: Since 2008, the NPCC’s innovations in urban climate science have propelled New York to the forefront of the global fight against climate change. Its recommendations have informed ambitious policies that have helped the five boroughs recover from past damage and emerge stronger, and its successful partnership with the City of New York and the New York Academy of Sciences demonstrates the power of collaboration between the public sector, industry and local leaders, and the scientific community. With the NPCC’s guidance, we are better prepared to anticipate and conquer the climate challenges that lie ahead.
Whereas: New Yorkers have always been known for their resiliency and boldness, and our city must meet concerns of this scale with solutions that our worthy of its residents. From increasing our coastal resiliency to pioneering a global protocol for cities to attain carbon neutrality by 2050, my administration remains steadfast in our efforts to protect people of all backgrounds from the impacts of climate change. As we continue to grapple with the grave risks that global warming poses, we are grateful to the NPCC for providing our city with the rigorous science needed to thrive in our rapidly changing world. Today’s Summit offers a wonderful opportunity to applaud this organization for a decade of service to New York City, and I look forward to the progress its members will continue to inspire in the years ahead.
Now therefore, I, Bill De Blasio, Mayor of the City of New York, do hereby proclaim Friday, March 15th, 2019 in the City of New York as:
Mental illnesses present a major health, social, and economic burden and affected individuals experience disproportionately higher rates of both disability and mortality. In fact, the CDC reports that nearly 50% of U.S. adults will experience a mental illness at some point in their lifetime. And according to the WHO, depression alone accounts for 4.3% of the total disease burden worldwide and is the single greatest cause of disability. Yet despite enormous unmet need, efforts to develop new therapies for mental illness have stalled in part because of a need for more clarity surrounding the biological underpinnings of these diseases. On October 9, 2018, the New York Academy of Sciences presented Advances in the Neurobiology of Mental Illness. The one-day symposium, sponsored by Janssen Research & Development, LLC, brought together scientists, clinicians, and policymakers to discuss the genetics, molecular biology, and neurobiology of a wide range of mental illnesses. Topics included novel targets for treating depression, using genetic profiles to assess the risk of experiencing mental illness, and broader questions about battling the stigma surrounding such conditions.
Speakers
Hilary Blumberg, MD Yale School of Medicine
David Bredt, MD, PhD Janssen Neuroscience
Wayne Drevets, MD Janssen Research & Development, LLC
Steve Hyman, MD Broad Institute of MIT and Harvard
Jeff Lieberman, MD Columbia University
Eric Nestler, MD, PhD Icahn School of Medicine at Mount Sinai
Maria Oquendo, MD, PhD Perelman School of Medicine at the University of Pennsylvania
Murray B. Stein, MD, MPH University of California, San Diego
Event Sponsor
The Molecular Basis of Mental Disorders
Speakers
Hilary Blumberg, MD Yale School of Medicine
Steve Hyman, MD Broad Institute of MIT and Harvard
Eric Nestler, MD, PhD Icahn School of Medicine at Mount Sinai
Highlights
Early-life experience changes response to stress into adulthood by affecting the expression of key genes
In people with bipolar disorder, brain structure and activity change during adolescence and early adulthood.
Polygenic risk scores are a promising tool for gauging a person’s likelihood of developing a psychiatric disorder such as schizophrenia.
Transcriptional and Epigenetic Mechanisms of Depression
Techniques measuring how genes are transcribed — in animal models and human post-mortem tissue — are providing new and valuable insight into depression, and potentially, new therapies, said Eric Nestler of Icahn School of Medicine at Mount Sinai. His team uses such techniques to explore the idea that behavioral experience, such as early life stress, can produce permanent changes in the genome structure and gene expression of brain cells; these permanent changes in turn contribute to shifts in behavior for a lifetime and predispose a person towards susceptibility to stress.
In 2016, Nestler and his colleagues subjected mice to a form of chronic stress and conducted RNA sequencing in four different brain regions. The stress made about half the mice susceptible to developing behaviors associated with depression and anxiety, while the other half remained resilient to mental health effects. The resilient animals tended to have bigger changes in gene expression, suggesting that susceptibility may be caused by the brain’s inability to make the needed changes.
Stress during one of two early life periods results in susceptibility to stress in adulthood.
The researchers then conducted a similar gene expression study on post-mortem tissue of people who had depression. They found a surprising result: Gene expression changes observed in women overlapped very little with those seen in men, suggesting that the biological underpinnings of depression differ in men and women. Animal models showed the same sex difference. “That really argues for drug discovery processes that will look at both sexes independently,” Nestler said. What’s more, three different types of chronic stress dysregulated different sets of genes, with little overlap between them.
Early life stress is one of the strongest biological risk factors for depression. Most people can withstand that stress and develop normally into adulthood, but they retain an increased vulnerability to later stress. To understand the molecular mechanisms involved, Nestler’s team investigated how early life stress affects gene expression in mice. Most studies deliver early life stress continually over the first three weeks of life, but in this case, the researchers delivered early life stress over two time periods. Animals stressed during the second period, but not the first, show abnormal social behavior when stressed later in life. Gene expression studies in three different areas of the brain suggest that stress during the second early life period changes gene expression to look as though the animal has experienced chronic stress in adulthood — again, with the changing genes being different in males and females.
This pattern was strongest in one of the brain regions studied, called the ventral tegmental area (VTA), in male mice. The largest portion of those gene expression changes were regulated by a gene called Otx2. When they overexpressed that gene in the VTA of young male mice after the mice had experienced stress during the second early life period, the animals were protected from stress in adulthood. In turn, impairing Otx2 expression during that time increases stress susceptibility and dysregulates the stress-related genes irreversibly.
Otx2 is probably just one of several genes regulating susceptibility to stress, but it provides a model for how early life experience can alter stress response for a lifetime. The researchers are now studying what Nestler calls “chromatin scars” — chemical markers in the dysregulated genes.
The Brain in Bipolar Disorder
Elevated mood episodes are considered a hallmark of bipolar disorder, and these symptoms generally emerge during adolescence. But the condition is also characterized by more primitive and less widely-studied symptoms such as changes in sleep, circadian rhythms, and energy levels, said Hilary Blumberg of the Yale School of Medicine.
These features may emerge earlier than emotional disturbances, and researchers are beginning to look closely at how such symptoms might be therapeutically targeted. Early intervention could prevent the progression of bipolar disorder, said Blumberg — this is especially crucial because about 50% of people with bipolar disorder attempt suicide, and 15%–20% die by suicide.
Most research on bipolar disorder has focused on the circuitry of emotional regulation. Blumberg described two key components of this circuitry: The amygdala, an almond-shaped region deep in the brain that gets excessively activated in people with bipolar disorder; and the ventral prefrontal cortex, the frontal part of the most recently-evolved part of the brain, the cerebral cortex, where activation can be lower in people with bipolar disorder. These regions are highly interconnected.
Many factors, both environmental and genetic, can influence the development of brain differences in bipolar disorder.
Blumberg’s lab hypothesized that by adolescence, functional and structural changes might be detectable in the amygdala, which matures earlier. The frontal cortex develops later, so the researchers predicted that its structure and function would progressively diverge from normal during adolescence and young adulthood. Blumberg and her team conducted three types of brain scanning to image the structure and function of the two brain regions, as well as the connection between them, and observed these changes. They also found that differences in a specific part of the frontal cortex correlate with attempts to commit suicide, regardless of whether subjects were diagnosed with bipolar disorder or major depressive disorder.
Additionally, Blumberg and colleagues are investigating adults with bipolar disorder to better understand how the aging process interacts with psychiatric conditions. Older adults often have a higher suicide risk; little research has focused on this developmental stage, but there is evidence that lithium may be effective in reducing suicide risk. They are also using brain imaging to explore the effects of genes thought to play a role in bipolar disorder, and identifying the effects of early life stressors, such as physical or emotional abuse or neglect, on brain structure and function in adolescence.
The group developed a behavioral therapy called BE-SMART that focuses on helping people with bipolar disorder improve their emotional regulation, and regularize their sleep and daily rhythms. Preliminary imaging studies show that after undergoing the therapy, patients have less activation in their amygdala and more in their frontal cortex. “In addition to pharmacological treatments, there are many other strategies that may help improve brain circuitry trajectories,” Blumberg said.
A New Molecular Map for Mental Disorders
In the 1960s, geneticists realized that psychiatric disorders were complex, but early researchers estimated that some 20 genes might underlie these conditions. Today, researchers are realizing that many thousands of variants in many hundreds of genes are involved, said Steve Hyman of the Broad Institute of MIT and Harvard. That underestimation may in part explain why only a handful of drug treatments exist for patients with these diseases — almost all of them discovered by chance. The field desperately needs new tools to identify molecular mechanisms that can be targeted with drugs, as well as biomarkers to help researchers identify which patients might respond to a therapy and which might not. Evolving genetic technologies provide those tools, Hyman explained.
Psychiatric diseases such as schizophrenia and bipolar disorder have a heritably of up to 80%; depression has a lower, but still strong, genetic component as well. However, while some diseases are caused by mutations in a single gene, these diseases tend to be driven by variants of many genes, with no single gene playing an outsized role. Humans have been evolving for about 200,000 years and share many common gene variants. Gene chips can scan up to one million locations in the genome to identify common variants for a given phenotype — whether it be a feature such as height or a disease like schizophrenia.
In schizophrenia, for example, some 280 spots in the genome carry variants that can each nudge a person towards or away from the disease. Researchers can calculate approximately how much risk each gene confers. One recently developed metric called the polygenic risk score combines the weighted contribution of each of these risk genes for a given individual and compares them to a baseline to estimate the probability that the person will develop the disease. This score is the first objective tool for determining whether someone might be a good candidate for a clinical trial. “It will just get better as the genetics advance,” said Hyman.
Most genetic samples come from people of European ancestry.
One problem with polygenic risk scores is that they are only as good as the population genetics data they are based upon. Most data come from white Europeans, so small deviations from the norm in that population are statistically detectable. But the collection of gene variants underlying a disease such as schizophrenia is likely to differ in people from Asia, Sub-Saharan Africa, and Latin and South America, so the polygenic risk scores of patients from these backgrounds are currently much less accurate. Geneticists are beginning to amass more diverse data, but much work on this front remains.
Genetic analyses of common variants are beginning to yield cellular and molecular clues about schizophrenia. Risk genes are not all expressed in all cell types in the body, and analyzing variants in individual cells may reveal which cell types are most affected in the disease. Early work from another team at Hyman’s institute has found that more risk genes are expressed in a cell type called pyramidal neurons in the brain’s cortex. As the technology improves, researchers hope to develop a cellular map of disease risk. Researchers can then use stem cell technologies to make different types of neurons and study how the disease affects them. “There are many years of work ahead of us,” said Hyman, “but I think we finally have a toe-hold.”
Wayne Drevets, MD Janssen Research & Development, LLC
Maria Oquendo, MD, PhD Perelman School of Medicine at the University of Pennsylvania
Murray B. Stein, MD, MPH University of California, San Diego
Highlights
Immune system molecules offer a promising target for novel depression therapies likely to help a subset of patients.
Drugs already approved for other psychiatric disorders may be effective treatments for post-traumatic stress disorder.
Studies point to at least two different phenotypes of suicidal behavior.
Neuroimmune Mechanisms as Potential Therapeutic Targets for Depression
Researchers know little about the underlying biology of mood disorders, so there is little to guide the field toward new treatments and biomarkers, said Wayne Drevets of Janssen Research & Development. However, emerging research suggests that some of the most reliable blood-based biomarkers for depression include immune molecules associated with low-grade inflammation, such as interleukin 6 (IL6), and proteins that react to inflammation, such as C-Reactive Protein (CRP).
Accumulating evidence points to Interleukin 6 as a promising target for treating depression.
Studies suggest that immune mechanisms play a role in roughly 33%–50% of patients with mood disorders, and that the adaptive immune system functions deficiently in depression. In a small subset of patients, autoantibodies to certain brain receptors and channels have been implicated in mood disorders. This suggests that at least some people with such conditions would benefit from therapeutics that target immunological mechanisms.
Several pharmaceutical companies formed a collaboration to explore this possibility (although currently, only Janssen and Glaxo SmithKline remain). Microarray data pointed to IL6 as a promising therapeutic target; IL6 levels remain high in people who do not respond to depression treatment and correlate with suicidality measures. They also predicted onset and severity of depression in children of parents with bipolar disorder. In animal models, antibodies against IL6 prevented depression symptoms in animals that experience a stressor.
The pharmaceutical company consortium pooled data from all trials to date and identified 18 trials that had drug targets and diseases with a prominent inflammatory component. Two of the tested drugs were Sirukumab and Siltuximab, Janssen compounds that target IL6. They then launched a double-blind placebo-controlled trial of Sirukumab as an adjuvant therapy in patients taking an antidepressant. The effects were not significant at 12 weeks, and a heightened infection rate in subjects suggested the need for a safer antibody or small molecule. However, additional analyses were encouraging. They showed that the antibody worked as intended, decreasing IL6 levels at the target, that the therapy did work in people with high CRP levels, and that a different, more sensitive depression measure hints that the treatment may work. “We do think this might be an important learning for future trials,” Drevets said.
It has long been unclear whether immunological therapies must work in the central nervous system or in the periphery to have an effect. To find out, the pharmaceutical company consortium is currently conducting a clinical trial of a small molecule that interferes with an ion channel called P2X7. The channel is expressed on the surface of brain cells called microglia and is activated by molecules produced by stress or inflammation. P2X7 activation causes depression-like behavior in animal models through the release of another interleukin called IL1-beta. Blocking the channel might therefore prevent stress-mediated IL-1beta release. If the small molecule works, Drevets said, it would validate the pursuit of central nervous system targets.
Neurobiology and Pharmacotherapy of Post-traumatic Stress Disorder
Although environmental factors often play a role in psychiatric disorders, post-traumatic stress disorder (PTSD) is the only psychiatric disorder that by definition involves exposure to a traumatic, life-threatening event, explained Murray Stein, from the University of California, San Diego. PTSD has four core features, but researchers calculate that there are more than 600,000 combinations of symptoms that can produce the disorder, and it often co-occurs with other conditions such as major depression and chronic pain.
Risk factors for PTSD vary widely.
Around 3% of people worldwide and 7% in the U.S. have the condition, but prevalence varies enormously by population. Women have PTSD at twice the rate of men, in part because of the types of trauma they tend to experience, and the rate for Native Americans living on reservations is 2–3 times that of the U.S. at large. Meanwhile, 30% of Vietnam veterans have the condition. Despite great unmet need, very few drugs exist to treat PTSD and none have been approved since 1999. However, certain psychotherapies do seem to help.
The lack of drug treatments may be partly due to a poor understanding of what causes the condition. Brain imaging studies suggest circuits involving emotional regulation, executive function, and threat detection is out of whack. Studies of soldiers deployed to Afghanistan and patients admitted to an emergency room have shown that traumatic brain injury sharply raises the risk of PTSD. Stein and colleagues recently showed in a small study that a drug called methylphenidate helps improve focus and alleviate hyperarousal in people with PTSD.
Using genome-wide association studies, researchers are beginning to identify genes associated with the disorder. Stein’s team led one such study, called ARMY STARRS, which found that a variant in a gene called ANKRD55 was associated with PTSD in African Americans. The gene’s function is unknown, but it is linked to multiple autoimmune and inflammatory disorders. He and others are collaborating with a large biobank called the Million Veterans Program in which DNA and survey results can be analyzed along with electronic health records. They identified a link between PTSD severity and the gene coding for corticotropin-releasing hormone receptor 1, which has already been associated with the disorder in other studies.
Finally, Stein noted that a few drug studies targeting dopamine receptors have shown promise, despite the fact that different studies have shown conflicting results. That could be because the effects of the drugs are uneven across PTSD symptoms, and therefore their benefits don’t register with the assessment tools used. Overall, he said, drug trials for PTSD have been limited, but combining genetics and bioinformatics may point to both new drugs and old drugs that deserve a second look.
Subtyping Suicidal Behavior: a Blueprint for the Development of Biomarkers
Maria Oquendo from the University of Pennsylvania described her work defining two distinct subtypes of suicidality. Suicide is a major epidemic, and identifying triggers and risk factors will help prevent deaths, she said.
The suicide rate varies widely between countries around the world, but overall, more people die by suicide (44,000 per year) than by automobile accidents (33,000). In the U.S., suicide has been on the rise since 1999. Some 5%–15% of the U.S. population experiences suicidal thoughts, and that number is thought to be much higher in adolescents. About four women attempt suicide for every one man; about three men for every one woman succeed.
Although nine out of 10 people who die by suicide have a psychiatric disorder, most people with a psychiatric disorder never attempt suicide — suggesting it is not enough to spur suicidality. Based on this observation, in 1999 Oquendo’s group proposed that some individuals are predisposed or pushed toward suicidality by behavioral factors such as aggression and impulsivity; mental factors such as cognitive inflexibility; biological factors such as dysregulated serotonin levels; or substance and alcohol abuse.
Oquendo’s lab proposed two distinct phenotypes of suicidal behavior.
In 2004, they interviewed about 300 people with depression three months, 12 months, and 24 months after an initial evaluation. High levels of either aggression and impulsivity or pessimism greatly increased the risk of a suicide attempt, supporting their model. In a later study of 415 people with depression, 27% of participants had borderline personality disorder (BPD), so the researchers analyzed them separately. In people without BPD, both major depressive events and stressors such as health, work, and family events precipitated suicidality. However, in those with BPD, life stressors did not seem to contribute — perhaps because people with BPD experience life stressors in a way not captured by the study.
Nonetheless, the results suggest at least two independent pathways to suicidality. Oquendo and her colleagues hypothesized that one type of suicide attempter, who often has experienced childhood abuse, now struggles to regulate their emotions, reacts aggressively to threats or frustration, and has higher levels of cortisol and other biological stress markers. In such a person, life stressors would provoke suicidal thoughts, and they would attempt suicide impulsively. Another type of suicide attempter is someone tormented by recurring suicidal thoughts. Such a person is not impulsive or aggressive and has good cognitive control, but might attempt suicide in the context of a depressive episode.
Accumulating data supports the existence of these two suicidality subtypes. For example, people with high reactive aggression who were abused as children show sharp and frequent spikes in suicidal thoughts, often in response to seemingly minor life stressors; while people with low reactive aggression and impulsivity, have more stable levels of suicidality. Those with high aggression and impulsivity also have a spike in cortisol levels in response to a social stress test in the lab. And people with BPD who had attempted suicide seemed less able to engage brain regions involved in decision-making and perspective, suggesting a difference in their emotional regulation. There are some hints that differences in serotonin receptor levels may be at play in these two groups.
Oquendo believes there may be at least three other subtypes of suicidality, and her lab is trying to identify them in a study that follows patients with depression over a two-year period. Ultimately, the aim is to identify clear biomarkers for all suicidality subtypes.
Stigma surrounding mental illness is alive and well, but eliminating it would revolutionize mental health care.
Imagine There Was No Stigma of Mental Illness
Suppose you had to give a toast for your boss at work one day, but you couldn’t make it because you were ill. Would you rather tell your colleagues you had a kidney stone, or that you were feeling suicidal? Jeff Lieberman of Columbia University opened his talk with this hypothetical scenario to illustrate that mental illness is still highly stigmatized.
Much of this stigma is driven by a decades-old skepticism and assault on the legitimacy of psychiatry, which came to a zenith when a doctor named Thomas Szasz — who wrote a book called the Myth of Mental Illness — joined forces with L. Ron Hubbard, inventor of an applied philosophy called Dianetics. The resulting belief system, Scientology, remains deeply opposed o psychiatry. The stigma of mental illness has real consequences — it is a serious deterrent to individuals seeking mental health care and has contributed a dysfunctional mental health delivery framework.
It also drives a funding disparity for mental health research. “If you do the math, 0.06% of the federal budget is spent on biomedical research that could advance our ability to understand and treat mental disorders and addiction,” Lieberman said — much less than for cancer, infectious disease, and cardiovascular disease. Because of that funding and attention, biomedical advances for these diseases made over the past several decades have led to effective treatments. Meanwhile, the World Bank estimates that by 2030, depression will be the most costly disease globally.
Medicine became a scientifically grounded endeavor in the 19th century and psychiatry formed one of he first professional organizations, now called the American Psychiatric Association (APA). At the time, the available tools limited progress in psychiatric research, and treatment for patients was often barbaric.
Psychiatry as a whole embraced Freud, and tried to apply his ideas to the broader population, despite the fact that they were irrelevant to specific illnesses such as schizophrenia and autism. “Theories were postulated that were preposterous and venal,” said Lieberman, such as that of the “refrigerator mother,” and overbearing parents as a cause of homosexuality, or orgone theory. By the 1950s and 1960s, when the number of patients in mental hospitals across the U.S. swelled to 550,000, the conditions under which most asylum patient lived were horrendous.
The turning point in the field’s validity came in the 1970s, when Columbia University psychiatrist Robert Spitzer was appointed chair of the APA’s task force to release the third edition of the Diagnostic and Statistical Manual of Mental Disorders (better known as the DSM, currently in its fifth edition). Although next to nothing was known about the biological basis of mental illness, he took a rigorous methodological approach, eliminating homosexuality as a diagnosis and describing post-traumatic stress disorder. The decades leading up to the 1980s were a scientific revolution of sorts, with the serendipitous discovery of psychotropic drugs and adoption of diagnostic methods. Today, it is a field wholly invested in scientifically driven methodology — the era of psychiatric neuroscience, Lieberman said.
It’s certainly possible to imagine eradicating the stigma surrounding mental illness — one stigmatized illness that succeeded in creating such a change is HIV. Without stigma holding back the field, and the institution of a health care system that provides mental health care from a public health standpoint, the results could be miraculous, Lieberman said. The system could target three distinct populations — the worried well, people with mild mental disorders such as anxiety and obsessive-compulsive disorder, and the severe mentally ill population — and offer them a variety of different avenues to care.
Jeffrey A. Lieberman and Ogi Ogas. Back Bay Books, 2016.
Panel Discussion
Speakers
Hilary Blumberg, MD Yale School of Medicine
Steve Hyman, MD Broad Institute of MIT and Harvard
Jeff Lieberman, MD Columbia University
Maria Oquendo, MD, PhD Perelman School of Medicine at the University of Pennsylvania
David Bredt, MD, PhD (Moderator) Janssen Neuroscience
Highlights
Complex chemistry and complex genetics are just two of the many challenges to developing drug therapies for mental illness.
There is conflicting data about whether people with bipolar depression should be treated with antidepressants.
The relationship between circadian rhythms and psychiatric disorders is poorly understood, but normalizing people’s sleep schedules may have therapeutic value.
The panel began by discussing the challenges in developing therapeutics for mental illness. Even in cases where the drug target is clear, the chemistry can be extremely challenging, said Hyman. There is also the issue of making sure the drug can be absorbed orally and then can cross the blood brain barrier. Also, he noted, psychiatric disorders are genetically very complex, and unlike cancers where researchers can identify a driver mutation to target with a precision therapy, many genes affected in psychiatric disorders converge on the same pathways.
On the other hand, said Oquendo, psychiatric illnesses have an advantage over cancer therapeutically, in that behavioral modulations can greatly help patients and can affect the underlying disease. In this field, she said, “there are many synergistic ways to skin a cat.”
In response to a question from the audience, Oquendo and Blumberg discussed the pros and cons of antidepressants for people with bipolar disorder. For a subset of patients, antidepressants might aggravate the condition, leading to a worse prognosis, Blumberg explained. Yet, if someone presents with depression, it is not always possible to determine whether they have major depressive disorder or bipolar disorder.
However, she noted, the literature is rife with conflicting data on whether antidepressants do in fact worsen the disease. Oquendo, meanwhile, said that the fear of giving bipolar patients antidepressants might actually have caused a good deal of suffering, and even suicides. In her experience, bipolar patients often strongly objected to being taken off antidepressants, and while epidemiologic and other studies don’t prove that antidepressants help, it’s not clear that they cause harm, either.
The panelists also discussed the role of circadian rhythms and sleep in bipolar disorder and other conditions. So far, chronobiological features have not been integral to the understanding of these diseases, but they may play a real role in their pathophysiology, said Lieberman. Researchers have long known that sleep deprivation can bring on a manic state, Blumberg noted, and shifting the sleep schedules of young adults with bipolar disorder often results in improvements to their condition. Another attractive dimension of targeting sleep and circadian rhythms, said Blumberg, is that “it’s a ‘do no harm’ intervention.”
Panel Discussion
Open Questions
How exactly does early life stress lead to behavioral changes in adulthood?
Can basic functions like sleep, daily rhythms, and energy levels serve as an early biomarker for bipolar disorder?
Can polygenic risk scores accurately stratify patients in clinical trials?
How should researchers design trials to test therapies that target immune molecules to treat depression?
How can genetics and bioinformatics data be combined to help identify new and repurposed drugs for PTSD?
How can researchers use accumulating knowledge on subtypes of suicidal behavior to develop effective interventions?
What can be done to eliminate the stigma of mental illness?
For centuries, physicians and scientists have thought of inflammation as the body’s acute response to infection or injury, but in recent decades it’s become clear that chronic inflammation drives pathologies as diverse as cancer, diabetes, and Alzheimer’s disease. Controlling this aberrant inflammation, however, has proven difficult. Conventional anti-inflammatory drugs work by antagonizing the body’s pro-inflammatory hormones, but that approach also suppresses immunity, opening the patient to secondary infections. A newer strategy relies on recently discovered resolution mediators, compounds that the body makes naturally to resolve inflammatory responses without suppressing other parts of the immune system. Drugs targeting this process have shown immense potential to treat many of the world’s most serious diseases, with fewer side effects than existing therapies.
On June 25–26, 2018, the New York Academy of Sciences hosted Resolution of Inflammation, Infection and Tissue Regeneration, a symposium featuring many of the top researchers in the rapidly developing field of resolution pharmacology. In two days of oral presentations, a poster session, and an extensive panel discussion, speakers and attendees reviewed the biggest advances and challenges in resolution biology. The meeting covered the basic biology of inflammation and its resolution, studies on animal models of chronic and acute diseases, and clinical trials of promising new inflammation-resolving drugs.
Speakers
Nan Chiang, PhD Brigham and Women’s Hospital, Harvard Medical School
Michael Conte, MD University of California, San Francisco
Jesmond Dalli, PhD William Harvey Research Institute, QMUL
Gabrielle Fredman, PhD Albany Medical Center
Catherine Godson, PhD University College Dublin
Dipak Panigrahy, MD Beth Israel Deaconess Medical Center, Harvard Medical Center
Paul Ridker, MD, MPH Brigham and Women’s Hospital, Harvard Medical School
Charles Serhan, PhD, DSc Brigham and Women’s Hospital, Harvard Medical School
Patricia Sime, MD University of Rochester School of Medicine
Matthew Spite, PhD Brigham and Women’s Hospital, Harvard Medical School
Ira Tabas, MD, PhD Columbia University
Mark Tepper, PhD Corbus Pharmaceuticals
Kevin Tracey, MD The Feinstein Institute for Medical Research
Thomas Van Dyke, DDS, PhD Forsyth Center for Clinical and Translational Research
Resolution Mediators and Mechanisms in Inflammation: Leads for 21st Century
Speakers
Charles Serhan Brigham and Women’s Hospital, Harvard Medical School
Charles Serhan, from the Brigham and Women’s Hospital and Harvard Medical School, opened the meeting with a keynote presentation that spanned the history of resolution physiology, a field he pioneered. Physicians and scientists have known about inflammation since antiquity, primarily as an acute condition associated with injury and infection. In recent years, however, biologists have come to understand that chronic inflammation underlies many non-communicable diseases, including cancer, diabetes, Alzheimer’s disease, and Parkinson’s disease.
Serhan has focused on how acute inflammation normally resolves, and how this process sometimes malfunctions, leading to chronic inflammation. When he entered the field, “in the textbooks, the resolution of acute inflammation was thought to be a passive event,” Serhan said. Pro-inflammatory molecules became diluted over time, bringing the inflammation to an end. Through an extensive series of cell culture, animal, and human studies, Serhan and his colleagues have overturned that model, showing that multiple families of pro-resolving molecules actively antagonize the inflammatory process and promote healing. These small fatty acid-derived molecules, now known as lipoxins, resolvins, protectins, and maresins, act through specific cellular receptors to orchestrate a complex switch from inflammation to resolution.
Several classes of chemical mediators actively drive inflammation resolution.
Serhan, like many others at the meeting, is now exploiting those findings to design new drugs that could treat a wide range of chronic conditions far more effectively than current anti-inflammatory compounds, with fewer side effects. “This is really a paradigm shift in thinking about how to treat inflammation, using agonists to stimulate resolution rather than inhibitors that eventually become immunosuppressive,” said Serhan.
Dipak Panigrahy, MD Beth Israel Deaconess Medical Center, Harvard Medical Center
Ira Tabas, MD, PhD Columbia University
Cancer Progression: Failure to Resolve?
Dipak Panigrahy, of Beth Israel Deaconess Medical Center and Harvard Medical School, started the meeting’s first session by discussing his work on inflammation resolution in cancer. Researchers first discovered the link between inflammation and tumor growth in the late 19th century, but only recently has it become clear that inflammation is an essential initiator of at least some types of cancer. A mouse model of pancreatic cancer, for example, does not get the disease unless it first develops pancreatitis.
Unfortunately, most current anti-inflammatory drugs suppress the immune system, allowing established tumors to become even more aggressive. To find better solutions, Panigrahy began dissecting the mechanisms linking cancer and inflammation. He discovered that cancer-killing interventions such as chemotherapy leave behind debris from the killed tumor cells. In a mouse model of ovarian cancer, that debris worsens the disease. “So the debris will stimulate the tumor growth. It’s kind of a double edged sword of cancer therapy,” said Panigrahy. Adding specialized pro-resolving mediator molecules (SPMs) stimulates phagocytic cells to engulf the cellular debris, inhibiting further tumor growth. Treatments that boost SPMs could work synergistically with chemotherapy to attack numerous types of cancer.
The Interplay between Efferocytosis and Inflammation Resolution
Ira Tabas from Columbia University continued the theme of clearing cellular debris, with a presentation about his group’s work on the process. Macrophage cells function as the body’s garbage collectors, engulfing the remains of dead cells through efferocytosis. The process is critical for healing damaged tissue and resolving inflammation, but it requires intensive metabolic management by the macrophage. “When a macrophage is eating multiple dead cells … it might be like you sitting down eating 20 filet mignons, and then half an hour later eating 20 more,” said Tabas, adding that “it’s a tremendous metabolic load.”
Efferocytosis of dead cells requires macrophages to handle a high metabolic load.
Tabas’s team studies efferocytosis in mouse models of heart disease. They found that eliminating a single gene in the animals blocks efferocytosis and leads to much worse disease, highlighting the importance of efferocytosis in resolving inflammation. Next, the researchers used an elegant in vitro assay to demonstrate that the degradation products from engulfing one dead cell regulate the macrophage’s ability to engulf a second one. The macrophages use another tightly regulated process to recycle the membranes of the dead cells. Together, the mechanisms explain how macrophages can keep their efferocytosis rates as high as possible without becoming metabolically overloaded.
Michael Conte, MD University of California, San Francisco
Gabrielle Fredman, PhD Albany Medical Center
Paul Ridker, MD, MPH Brigham and Women’s Hospital, Harvard Medical School
Providing Proof of Principle for Atherosclerosis, Lung Cancer, Kidney Disease, and Osteoarthritis: Lessons from CANTOS
Paul Ridker from Brigham and Women’s Hospital began the second session with a keynote address on the CANTOS clinical trial. This trial sought to address several questions about inflammation resolution in cardiovascular disease.
Atherosclerosis is a leading cause of vascular disease worldwide. Researchers have identified numerous factors that predict the onset of atherosclerosis, including high blood pressure, cholesterol, and markers of chronic inflammation, but it remains unclear which of these factors are causative and which merely correlate with pathogenesis.
Current treatments for atherosclerosis focus on lowering blood pressure and cholesterol levels, but Ridker and his colleagues wanted to target inflammation instead. To do that, they used a human monoclonal antibody drug called canakinumab, which binds the pro-inflammatory protein interleukin-1beta. IL-1beta triggers a series of signals that promote inflammation and also increase blood levels of C-reactive protein (CRP), a biomarker of atherosclerosis. A pilot study on 1,400 patients sought to determine how much canakinumab it would take to reduce patients’ CRP levels to baseline, but the drug was so powerful that it worked at all doses tested.
The CANTOS trial enrolled over 10,000 patients to test canakinumab in patients with cardiovascular disease.
Based on those data, Ridker’s team designed a much larger trial, enrolling over 10,000 patients. The participants all had high CRP levels even after aggressive cholesterol-lowering therapy, indicating that they were still suffering from chronic inflammation. Those treated with canakinumab showed dramatic reductions in CRP, and concomitantly lower rates of cardiovascular events over the trial’s seven-year run, compared to controls who received a placebo. Crucially, treated patients showed no signs of immunosuppression, and most of the drug’s side effects were mild or even beneficial. For example, patients in the treatment groups had significantly lower rates of overall cancer mortality and chronic kidney disease than controls.
The results show that atherosclerosis treatment plans should focus on both cholesterol and inflammation. “If we’re going to beat this disease, we have to [target] both of these processes,” said Ridker.
Resolution of Vascular Injury: Mechanisms and Therapeutic Implications
Michael Conte, of the University of California, San Francisco, addressed what happens in the next step of modern vascular disease management: surgery. “It really doesn’t matter what we do when we touch blood vessels, whether we inflate a balloon, scrape out plaque, do a bypass graft or insert a catheter, we are faced with a scarring response … that has a classic inflammatory and resolution phase,” Conte explained.
In animal models of vascular injury, damaged blood vessels become inflamed, then produce specialized pro-resolving mediators (SPMs) to resolve the inflammation. Conte’s group also found that delivering extra SPMs locally to the site of injury significantly improves inflammation resolution and healing.
To put that finding into practice, the investigators have developed thin film polymers that can release SPMs directly into a vessel over time. They wrap the film around the blood vessel during surgery and leave it in place to deliver the molecules for days afterward. The system reduces graft thickness in a rabbit bypass graft model, and improves outcomes in mouse models of aneurysm surgery and thrombosis. Conte is also conducting a clinical trial testing the safety of naturally isolated SPM-stimulating compounds in humans.
Dysregulation of Resolution Pathways in Atherosclerosis
Gabrielle Fredman from Albany Medical Center continued the vascular theme, discussing her work on how dead cells get removed from atherosclerotic plaques. As a plaque develops on the wall of an artery, the cells at the center begin to die. This weakens the structure of the plaque and makes it more likely to rupture. Fredman studies this process in genetically modified mice that develop atherosclerosis when fed a high-fat diet. Treating these mice with SPMs decreases necrosis in their plaques, but how?
When cells die through apoptosis, or programmed suicide, macrophages rapidly engulf the resulting debris. Fredman and her colleagues found that cells undergoing necroptosis, such as those in the core of a plaque, are apparently much less appetizing. Macrophages fed necroptotic cells take them up much more slowly and in smaller pieces. “This resembles something like a nibbling process rather than a whole engulfment process,” said Fredman. The researchers subsequently found that a molecule called CD47 on the necroptotic cells may act as a “don’t eat me” signal, slowing their engulfment by macrophages. Adding SPMs, however, boosts macrophages’ efferocytosis responses enough to overcome that signal.
Speaker Presentations
Further Readings
Ridker
Aday, A.W., Lawler, P.R., Cook, N.R., et al. (2018).
Nan Chiang, PhD Brigham and Women’s Hospital, Harvard Medical School
Jesmond Dalli, PhD William Harvey Research Institute, QMUL
Kevin Tracey, MD The Feinstein Institute for Medical Research
The Role of n-3 Docosapentaneoic Acid-derived Pro-resolving Mediators in Systemic Protection
Jesmond Dalli, of the William Harvey Research Institute at the Queen Mary University of London, began the second part of the session with a presentation linking circadian rhythms and vascular inflammation. Disruption in circadian rhythms has been linked to metabolic disorders and cardiovascular disease progression, so Dalli wondered whether specialized pro-resolving mediators (SPMs) also showed circadian patterns.
Dalli’s team took blood samples from seven healthy volunteers throughout a 24-hour period, and found that the level of n-3 DPA, a precursor to SPMs, rose and fell in a consistent cycle. In contrast, patients with cardiovascular disease lose this circadian regulation, and have consistently low levels of SPMs. Additional experiments in mice confirmed the link. “This suggests that [loss] in circadian regulation of this pathway leads to a breakdown [in] early morning activation of platelets and monocytes,” said Dalli, “and that this then promotes cardiovascular disease.” He and his colleagues found that the cholesterol-lowering drugs atorvastatin and pravastatin increase the production of two SPMs, reinforcing other groups’ findings that these drugs combat cardiovascular disease through multiple mechanisms.
Pro-resolving Receptors: Mechanisms and Signaling
Nan Chiang from Harvard Medical School talked about the cellular receptors that respond to SPMs. One well-characterized SPM, resolvin D2, is a potent promoter of inflammation resolution; even extremely low doses of resolvin D2 can limit peritonitis and enhance survival in animal models of sepsis.
Resolvin molecules signal through specific cellular receptors to generate their observed effects.
Chiang suspected that resolvin D2 might act through a G-protein coupled receptor, so she tested a panel of 77 of these receptors whose functions had not yet been identified. That screen revealed that the receptor GPR18 responds strongly to resolvin D2. Human macrophages overexpressing GPR18 respond more strongly to resolvin D2 than controls; and mice lacking GPR18 don’t benefit from resolvin D2 treatment during experimental E. coli infection or sepsis, confirming that GPR18 is a biologically relevant receptor for resolvin D2.
In addition to resolvins, Chiang also studies another family of SPMs, known as maresin conjugates in tissue regeneration (MCTRs). She discovered that MCTRs act through a receptor called CysLT1 to reduce vascular leakage after injury. Knowing the receptors for these SPMs should facilitate the design of drugs with similar effects.
Molecular Approaches to Bioelectronic Medicine
Kevin Tracey, from the Feinstein Institute for Medical Research, started the meeting’s second day with a keynote presentation on bioelectronic medicine. Instead of manipulating body chemistry with chemicals, bioelectronic treatments connect electronic devices to the nervous system to stimulate desired responses. “The idea of bioelectronic medicine is a mechanistic approach to using electrons to replace drugs,” Tracey explained.
The vagus nerve connects the brain to multiple organs, and also the immune system.
About thirty years ago, when Tracey was a practicing neurosurgeon, a young patient died in his arms from shock. That spurred him to search for new drugs that could block shock-causing cytokines. In one experiment, his lab injected a promising anti-inflammatory drug directly into the brains of mice with experimentally induced strokes. It blocked inflammatory cytokines in the brain, but also in other organs throughout the animals’ bodies. That made no sense, as the molecule shouldn’t have been able to escape the brain.
The researchers subsequently discovered that the vagus nerve can trigger an anti-inflammatory reflex throughout the body, connecting the nervous system directly to the immune system. Subsequent work by others revealed that the vagus nerve stimulates the production of pro-resolving mediators in multiple organs and tissues. Tracey’s team is now conducting clinical trials to treat Crohn’s disease with an implanted electronic device that stimulates the vagus nerve and triggers this response.
Speaker Presentations
Further Readings
Dalli
Arnardottir, H., Orr, S.K., Dalli, J., and Serhan, C.N.
Proc. Natl. Acad. Sci. U.S.A. 2018; 115(21):E4843-E4852.
Session 3: Better Living through Chemistry
Speakers
Patricia Sime, MD University of Rochester School of Medicine
Matthew Spite, PhD Brigham and Women’s Hospital, Harvard Medical School
Temporal Biosynthesis of Pro-Resolving Lipid Mediators by Distinct Immune Cell Subsets during Skeletal Muscle Injury and Regeneration
Matthew Spite, of Brigham and Women’s Hospital and Harvard Medical School, returned the focus to chemistry, with a discussion of the specialized pro-resolving mediators (SPMs) that orchestrate healing from injuries. Using mass spectrometry, Spite identified all of the lipids produced in an injured mouse muscle as it recovers. The lipid profile changes over time and increases in the well-known resolvin subset of SPMs correlate with healing. That correlation persists whether the muscle damage comes from a toxin or exercise. “A lot of these pathways were consistent in two distinct models of injury,” said Spite. His team next characterized the macrophages present in the healing tissue, and found a distinct shift from pro-inflammatory to pro-resolving macrophage types, in sync with the shift in the lipid profile.
COPD: Inflammation, Infection and Resolution
Patricia Sime, from the University of Rochester School of Medicine, discussed the role of SPMs in chronic obstructive pulmonary disease (COPD). COPD, a chronic inflammatory condition, is now the fourth leading cause of death worldwide. It is caused primarily by smoking. “There’s actually no drug treatment for COPD,” said Sime, “so it’s a huge unmet need.”
Exposing mice to precisely controlled doses of cigarette smoke provides a model of human lung inflammation.
To better understand COPD, Sime used mass spectrometry to profile the lipids in exhaled breath condensates from patients with the disease as well as healthy controls. That pointed toward the SPMs resolvin D1 and D2 as critical mediators of inflammation resolution in the lung. Treating a mouse model of chronic smoking with resolvins decreases inflammation in the animals’ lungs. Sime hopes to exploit these findings to develop new therapies for COPD, as well as prophylaxis against lung damage from all types of smoke inhalation.
Thomas Van Dyke, DDS, PhD Forsyth Center for Clinical and Translational Research
Lipoxins and Lipoxin Mimetics Attenuate Diabetic Complications
Catherine Godson of University College Dublin opened the meeting’s final session with a presentation on lipoxins in diabetes. As a result of the obesity pandemic, diabetes has become an immense global health problem. One of the most serious complications of diabetes is kidney disease. “Those with the most profound diabetic kidney disease… have almost 50% increased mortality,” said Godson, adding that “there are no effective therapeutics” for the condition.
In an effort to change that, Godson and her colleagues have examined the lipoxin A4 molecule, a specialized pro-resolving molecule (SPM) that attenuates inflammation in animal models. The researchers found that lipoxin A4 attenuates molecular signals that promote fibrosis, helps maintain epithelial tissue integrity, and reduces activation of the inflammatory cytokine TGF-beta. “All of these are important potential targets of lipoxin actions in the context of chronic kidney disease and diabetic kidney disease,” said Godson.
Lipoxins mediate multiple protective and inflammation-resolving effects.
Next, Godson investigated lipoxin A4’s effects in animal models. Mice fed a high-fat diet become obese and develop kidney and liver disease similar to that seen in obese humans. Treating the animals with lipoxin A4 protects their livers and kidneys. Godson and her colleagues have also found that lipoxin A4 can reverse atherosclerosis in the overfed mice.
To translate those findings into practical medications, Godson is now working with synthetic chemists to develop drugs that can mimic the effects of lipoxin A4 in humans.The team has developed several promising leads, and is now testing them in various preclinical models.
Targeting the Endocannabinoid-Specialized Pro-resolution Mediator Pathway with Lenabasum to Treat Chronic Inflammatory/Fibrotic Diseases
Mark Tepper from Corbus Pharmaceuticals discussed lenabasum, the company’s synthetic, oral, small-molecule, selective cannabinoid receptor type 2 (CB2) drug. The endocannabinoid system activates the resolution of inflammation through the CB2 receptor. This GPCR is commonly found on activated immune cells during inflammation.
Based on promising preclinical results, Corbus tested lenabasum in the human clinical study (“blister model”) that has been designed to follow the progression of an inflammatory stimulus and subsequent resolution of inflammation. This study showed that lenabasum indeed stimulates inflammation resolution, reduces pro-inflammatory mediators, and promotes the clearance of bacterial endotoxins.
Corbus is now conducting more advanced clinical trials in patients with various chronic inflammatory conditions, including scleroderma, dermatomyositis, cystic fibrosis, and lupus. So far, the safety profile has been favorable with no serious adverse events attributed to lenabasum and no evidence of immunosuppression.
The Role of Resolution Phase Mediators in Oral Medicine
Thomas Van Dyke, from the Forsyth Center for Clinical and Translational Research, gave the final presentation: a look inside the mouth. Over 90% of American adults over age 30 suffer from gingivitis, and about 14% of them – or 22 million people – have severe periodontal disease. Conventional anti-inflammatory drugs can slow the progression of this disease, but can’t stop it.
A resolvin-containing mouthwash treats periodontal disease in an animal model.
In a rabbit model of periodontitis, Van Dyke has found that rinsing the animals’ mouths with a SPM analog called benzo-lipoxin A4 reverses periodontitis and restores lost bone in the jaw. That’s far better than any previously studied treatment. “There is no [prior] example of pharmacologically induced bone regeneration in periodontal disease anywhere, this just doesn’t happen,” said Van Dyke. Additional studies in pigs yielded similar results, and Van Dyke and his colleagues are now conducting a clinical trial on benzo-lipoxin A4-containing mouthwash in patients with periodontitis.
Panel Discussion: Barriers to Translation in Inflammatory Disease
The meeting concluded with a wide-ranging panel discussion with extensive audience interaction, featuring speakers Godson, Sime, Conte, Tepper, and Van Dyke, and led by keynote presenter Serhan. Panelists covered issues that ranged from the need for better biomarkers to follow inflammation resolution in laboratory and clinical studies; to the difficulty of overcoming old paradigms of anti-inflammatory interventions in medicine; and the complex interplay between drug-based and “alternative medicine” strategies for promoting inflammation resolution.
Approximately 36.7 million people currently live with HIV worldwide. Successful treatment with antiretroviral therapy has controlled the virus and prevented transmission in more than 20 million people. However, barriers to treatment and prevention such as stigma and discrimination, especially against women, are still prevalent in the communities most affected by HIV. According to the United Nations, an integrative strategy is required, not only in response to HIV, but also for the advancement of women’s sexual and reproductive health and rights. To accomplish this, they have focused on three main areas of intersection between HIV and women’s health: hormonal contraception, cervical cancer, and female genital schistosomiasis (FGS). Recent scientific advances raise the possibility of enhancing women’s health through closer collaboration and engagement between women, their health care providers and health programmers, and policy makers.
On March 15, 2018, the Joint United Nations Programme on HIV/AIDS (UNAIDS), the World Health Organization (WHO), and the Microbiology & Infectious Diseases Discussion Group at the New York Academy of Sciences presented Improving Women’s Health: HIV, Contraception, Cervical Cancer and Schistosomiasis. Coinciding with the 62nd session of the UN, the daylong symposium focused on improving women’s health in line with the UN Sustainable Development Goals designed to broaden community response to HIV and identify methods of intervention and treatment for reproductive diseases that afflict women.
Speakers
Sharon Achilles, MD, PhD University of Pittsburgh
Shona Dalal, PhD World Health Organization
Jennifer Downs, MD, PHD Weill Cornell Medical College
Danielle Engel, MA United Nations Population Fund (UNFPA)
Mary Rose Giattas, MD Jhpiego
Ebony Johnson, MHS Global Coalition on Women and AIDS, Athena Network
Eyrun Kjetland, MD, PhD University of KwaZulu-Natal, South Africa
Erna Milunka Kojic, MD Mount Sinai St. Luke’s, Mount Sinai West
Terry McGovern, JD Columbia University Mailman School of Public Health
Pragna Patel, MD US Centers for Disease Control and Prevention
Chelsea Polis, PhD Guttmacher Institute
Nelly Rwamba Mugo, MD Kenya Medical Research Institute
Vikrant Sahasrabuddhe, MBBS, MPH, DrPH National Cancer Institute, NIH
Annah Sango Zimbabwe Young Positives
Sponsors
Additional support provided by a medical education grant from Gilead
Session 1: Setting the Scene
Speakers
Terry McGovern, JD Columbia University Mailman School of Public Health
Women’s Sexual and Reproductive Health and the Sustainable Development Goals (SDGs)
Terry McGovern, of the Mailman School of Public Health at Columbia University, introduced the Sustainable Development Goals (SDGs) set by the UN and aimed at ending poverty by tackling a range of social and economic issues, including gender inequality. As a poverty lawyer in the late 1980s, McGovern witnessed first-hand human rights violations against women with HIV, including refusal to provide health benefits. “Science is affected by structural barriers,” said McGovern. At the time, “science had overlooked converging epidemics.” Today, the intersection between HIV and women’s healthcare, including hormonal contraception, cervical cancer, and female genital schistosomiasis continues to pose a problem in countries around the world. The purpose of this meeting was to raise awareness and promote efforts to end gender inequalities, empower women and girls, and to highlight the co-infections of HIV and female reproductive illnesses.
Speaker Presentation
Session 2: HIV and Cervical Cancer
Speakers
Danielle Engel, MA United Nations Population Fund (UNFPA)
Mary Rose Giattas, MD Jhpiego
Ebony Johnson, MHS Global Coalition on Women and AIDS, Athena Network
Erna Milunka Kojic, MD Mount Sinai St. Luke’s, Mount Sinai West
Vikrant Sahasrabuddhe, MBBS, MPH, DrPH National Cancer Institute, NIH
Annah Sango Zimbabwe Young Positives
The Intersection of Cervical Cancer and HIV
Vikrant Sahasrabuddhe, of the National Cancer Institute at the NIH, explained the intersection of cervical cancer and HIV. Cervical cancer, caused by oncogenic genotypes of the human papillomavirus (HPV), is a leading cause of cancer-related morbidity and mortality among women globally. HIV-infected women have three to five times higher risk for HPV-induced cervical lesions to progress to invasive cervical cancer. Millions of women with HIV now access affordable antiretroviral therapy globally and are living long enough for cervical cancer to manifest and progress. There are several approaches to prevent cervical cancer, including HPV vaccination and early detection and treatment of cervical precancerous lesions. Sahasrabuddhe talked about efforts underway to innovatively expand cervical cancer prevention services globally piggybacking on infrastructures developed through HIV care and treatment programs. ‘Screen-and-treat’ strategies use a low-cost simple clinical innovation called visual inspection with acetic acid (VIA) to detect precancerous lesions, followed by either freezing of the lesions by cryotherapy or referral of women with larger lesions for further evaluation and excisional treatment. Rapid, point-of-care HPV tests with self-collection of samples are being introduced for improving the sensitivity of VIA-based screening, although testing costs are still a barrier. Sahasrabuddhe concluded by emphasizing the need for improving current interventions and provided an overview of efforts for evaluating reduced dosing of HPV vaccines, improvements in screening accuracy via technological advancements, and novel non-surgical alternatives for treating precancer.
The three pillars of cervical cancer prevention provided by the WHO.
HPV Vaccine and HIV in Women
Erna Mulinka Kojic, of Mount Sinai St. Luke’s, continued the conversation on HIV and HPV co-infections. She pointed out that cervical cancer is not the only known cancer caused by HPV. For example, HPV also causes oropharynx, anal, oral cavity, larynx, vulva, and penile cancers but they have been neglected in the field, resulting in a lack of national recommendations for screening methods. Kojic then shifted the focus to HPV vaccines, which consist of virus-like particles housed in empty shells that are specific to HPV types. This specificity makes it difficult to create one vaccine for treating all nine types of HPV. Efficacy trials of the current quadrivalent HPV vaccine –which targets HPV types 6, 11, 16, and 18—indicate that it is 98% effective in preventing cervical cancer. However, in individuals previously infected with HPV types 16 or 18, the efficacy drops to 44% and even further to 17% in those with a history of any other type of HPV. Hence, the goal is to vaccinate boys and girls between the ages of 9-26 to catch cases before infection occurs. In a study on the immunogenicity of the quadrivalent HPV vaccine in HIV+ women, Kojic and colleagues found the vaccine to be highly safe and effective among this population. Vaccinated women showed a large increase of antibody titers compared to pre-inoculation levels, indicating the success of the vaccine. These exciting results present the possibility that the vaccine can do more than prevent HPV in uninfected individuals but also protect HIV+ women.
Bending the Curve for Cervical Cancer Prevention in Tanzania-Reflections on Effective Programming for Population Coverage
Mary Rose Giattas, of Jhpiego (a Johns Hopkins University affiliate), reflected on the challenges Tanzania faced while developing a national program for cervical cancer prevention (CECAP). The combination of Tanzania’s high incidence rate of cervical cancer, a large pool of adult women with HIV infection, and the lack of CECAP services provided in rural areas where more than 71% of the population lives, led the Tanzanian ministry to improve cancer services throughout the nation. In 2008, the Reproductive Health Cancer Unit was established with the goal to ensure women are free of cervical cancer. Through the support of the WHO and Merck, in collaboration with cervical cancer program implementing partners Tanzania developed a strategic plan focusing on the WHO’s three pillars of prevention. Jhpiego with USG funded MAISHA program provided technical inputs in the development process. While this plan has allowed doctors to successfully treat patients with small lesions using cryotherapy, the limited supply of LEEP devices creates a challenge in treating patients with larger lesions. Hence, collaboration between the Tanzanian ministry and Jhpiego, an international non-profit health organization with USG funding, has helped to further strengthen the key health system components in the program with the focus on the same day screening and treatment . Jhpiego has also been providing technical assistance to other implementing partners to improve access and quality of cervical cancer prevention services including timely and appropriate referral. Strong partnership between the MOH and implementing partners has contributed to scale up high quality VIA and Cryotherapy services for women with cervical cancer. In the 9 years since it was first implemented, this program has increased the number of CECAP sites from 3 to 557, improved cervical cancer and HIV testing, and reached more than 600,000 women in Tanzania. Bending the curve for cervical cancer prevention in Tanzania requires improving coverage by providing greater access to services through health system strengthening led by an empowered MOH, which has taken on the task of eliminating cervical cancer in Tanzania.
Cervical and uterine cancer affect approximately 38% of women in Tanzania.
How Does Science and Delivery Affect People in Communities?
Following the incredible milestones of Tanzania’s health services, Annah Sango, of the Zimbabwe Young Positives, spoke about the harsh realities women in Zimbabwe face when seeking medical treatment for HIV. Some common issues include long lines at doctors’ offices due to limited supplies, low accessibility of healthcare providers in rural areas, and the stigma prevalent throughout the community. She advocated for more information on medical treatments, more access to care in both urban and rural areas, the need to involve and educate young boys and men, and friendlier doctors who provide unbiased treatment. Government collaborations with health organizations, similar to the programs Tanzania successfully implemented, would greatly benefit the Zimbabwean community.
The United Nations Joint Global Programme on Cervical Cancer
Danielle Engel, of the United Nations Population Fund, presented the development of a new, five-year Joint Programme at the UN, which seeks to eliminate cervical cancer globally. Given that we know how to treat cervical cancer and the prevention is cost effective, the greatest obstacle is making treatment widely available, especially in middle- and low-income nations with the highest incidence rates. The Programme is based on three pillars: prevention, treatment, and care. At the national level, the goals are to increase HPV immunization access to all girls, ensure screening and treatment for cervical pre-cancer by providing technical assistance to local governments, and guarantee universal access for the diagnosis and treatment of invasive cervical cancer. At the global level, new innovative technologies are needed for cervical cancer screening, as well as policies to improve and increase access to HPV vaccination.
The burden of cervical cancer is highest in the global south, with sub-Saharan Africa particularly affected.
Women, HIV, HPV and Cervical Cancer: An Intersectional Approach Moving beyond the Biomedical Lens
Although technological advances have enabled a needed reduction of new HIV infections, these advances are hampered by policy, funding, and access barriers in many parts of the world. Ebony Johnson, from the Global Coalition on Women and AIDS, Athena Network, gave a compelling call to action, emphasizing the need to go beyond the biomedical to include a human rights lens in the creation of enabling environments for healthy women and girls. As part of the Athena Network’s global #WhatWomenWant campaign, Johnson and colleagues asked women and girls around the world what they need to be safe, healthy, educated, and empowered in their communities. Participants said they want respect, representation, equal opportunities, power and autonomy over their own bodies, and much more. Johnson advocated for women and girls to be a part of research at the onset and for doctors to communicate better with their patients, creating bi-directional interactions and suspending judgment. “[Women] know our bodies, we know our communities, we know our environments, we know our barriers,” said Johnson, “and we know how to help you help us.” Ultimately, expanding funding, igniting political will, promoting intersectional sexual and reproductive healthcare, and developing innovative HIV, HPV and cervical cancer programming are key components of achieving gender equality.
Session 3: The Right to Comprehensive Sexual and Reproductive Health and Rights
Speakers
Peter Godfrey-Faussett UNAIDS
Sharon Achilles, MD, PhD University of Pittsburgh
Shona Dalal, PhD World Health Organization
Ebony Johnson, MHS Global Coalition on Women and AIDS, Athena Network
Nelly Rwamba Mugo, MD Kenya Medical Research Institute
Chelsea Polis, PhD Guttmacher Institute
Vikrant Sahasrabuddhe, MBBS, MPH, DrPH National Cancer Institute, NIH
Annah Sango Zimbabwe Young Positives
Hormonal Contraceptive Methods and Women’s Risk of HIV Acquisition: Understanding the Evidence
Observational studies have suggested an association between use of specific hormonal contraceptives (HCs), particularly the injectable depot medroxyprogesterone acetate (DMPA), and increased risk of HIV acquisition in women. This issue is critically important for women’s health, particularly in sub-Saharan Africa, where high rates of HIV coincide with high use of injectable contraception. Chelsea Polis, from the Guttmacher Institute, presented the results of a comprehensive review she conducted with her colleagues on the relationship between HC methods and HIV risk. The preponderance of data for oral contraceptive pills, injectable norethisterone enanthate, and levonorgestrel implants do not suggest an association with HIV acquisition, though data for some of these methods were limited. On the other hand, new information increases concerns about a potential causal association between DMPA and HIV acquisition risk in women, although the possibility of confounding in these observational data cannot be excluded. Since DMPA is the most commonly used type of birth control in sub-Saharan Africa, these results could have important implications for these epidemiological populations. A meta-analysis estimated that DMPA may increase a woman’s risk of HIV acquisition by about 40%. In other words, if the association between DMPA and HIV is causal, a woman with a 2.4% chance of HIV per year would increase her risk to 3.3% if she uses DMPA. Similarly, a woman who starts at a higher baseline risk, for example, 14% per year, would increase her risk to about 19% per year if she uses DMPA. While these studies suggest a potential causal association between DMPA and women’s risk of HIV, all currently available data are observational, and thus potentially vulnerable to confounding. A randomized study is underway to attempt to parse out the relationship between various HC methods and women’s risk of HIV acquisition.
Even though Sub-Saharan Africa has the lowest contraceptive use compared to other regions, injectables comprise the largest portion of contraceptive methods. The prevalence of injectables is due to their discrete and easy-to-use nature, but it is concerning that their use overlaps with nations where HIV prevalence is highest.
Hormonal Contraception and HIV Acquisition Risk: Biological Plausibility, Clinical Evidence, and Research Gaps
Sharon Achilles, of the University of Pittsburgh, addressed the biological evidence for the possible mechanisms of action of HCs in HIV-infected individuals. She focused on four main mechanisms, including: changes in architectural epithelial cells, target cells, immune changes, and microbiota. Architectural changes of epithelial cell thinning were seen in animals given DMPA. However, similar studies in women failed to show significant thinning between the follicular and luteal cycles, which has led researchers to nearly abandon this mechanism of action. Evidence for target cell changes in healthy HIV- women on DMPA showed increased cervical CD8CCR5+ target cells during high progestin concentrations, which was not evident in women using Net-En, an alternative injectable contraceptive. Studies on adaptive and innate immune changes have provided variable results making it difficult to converge on a specific mechanism. Finally, none of the hormonal methods shifted the vaginal microbiota studied including Lactobacilli, Gardnerella, and Atropobiumvaginalis. Achilles cautioned that the study of biological changes associated with HC is complicated by the diversity of available hormones and delivery routes. There is a need for more precise categorization of progestin types, progestin concentration, and mode of administration to converge results from multiple studies and understand the biological mechanisms linking HCs to HIV.
Update on the Evidence for Contraceptive Options and HIV Outcomes (ECHO) Trial
Given the lack of a causal link between DMPA and HIV risk, the Evidence for Contraceptive Options and HIV Outcomes (ECHO) trial was created to fill this critical knowledge gap. Nelly Rwamba Mugo, of the Kenya Medical Research Institute, provided an update and overview of the trial. As an open-label randomized clinical trial for HCs, ECHO has recruited more than 7,800 women, ages 16-35, in four countries since it began in 2015. Participants were randomly assigned to one of three types of birth control: DMPA, levonorgestrel (LNG) implant, or copper intrauterine device (IUD), and regularly tested over 18 months for HIV and pregnancy. Furthermore, participants were given contraceptive and HIV-risk reduction counseling. The results of the study, expected within the next year, will indicate HIV incidence, pregnancy rates, serious adverse events (SAEs), and method continuation associated with each of the three HCs. This information will help policymakers formulate counseling options for clinicians and educate women and communities on the benefits and risks of using the three contraceptive methods.
The ECHO trial will allow researchers to compare HIV incidence across three different types of contraceptives using twelve study sites across four African nations.
Translating Evidence to Policy: Guidance on Hormonal Contraceptive Use for Women at High Risk of HIV
Shona Dalal, of the World Health Organization (WHO), reviewed the Medical Eligibility Criteria (MEC) used by the WHO to provide recommendations on 25 methods of contraception. Based on the review of various hormonal contraceptive methods and HIV conducted by Chelsea Polis and colleagues, the WHO changed the classification for progestogen-only contraceptives for women at high risk for HIV from no restriction, to an indication that the advantages of this method generally outweigh the theoretical risks. In reassessing the risk level, they considered the following: quality of the evidence (GRADE profile), values and preferences of contraceptive users and providers; balance of benefits and harms; priority of the problem; equity and human rights; acceptability; and feasibility. Although there continues to be evidence of a possible increased risk of contracting HIV among progestogen-only injectable users, there is an absence of evidence from randomized trials and unclear causality (methodological issues versus a real biological effect). Dalal stressed that messaging surrounding possible risk is critical so that women at low risk of HIV infection don’t change their preferred method of contraception. “The WHO is committed to keeping emerging evidence under close review,” said Dalal, before explaining that data from the ECHO trial is highly anticipated so that the WHO can incorporate it into future guidance accordingly.
Panel Discussion: Integrating Rights, Services and HIV
The first panel discussion addressed the impending results of the ECHO trial and its impact on the communities that use DMPA. Peter Godfrey-Faussett from UNAIDS moderated the conversation, which included four of the speakers: Annah Sango, Ebony Johnson, Nelly Rwamba Mugo, and Vikrant Sahasrabuddhe. The panelists warned that African communities rely heavily on DMPA for contraception and it is vital that they are informed early about the possible outcomes of the study and how to proceed. Education about alternative methods of contraception should come from a collaborative partnership between patients and healthcare providers rather than media outlets. This can prevent fear and overgeneralizations of HIV risk to other types of birth control which may not apply.
Panelists also discussed the intersection of HPV, contraceptives, and cervical cancer. Sahasrabuddhe noted that the literature on HCs and HPV acquisition is mixed but oral contraceptives tend to increase risk of HPV. Yet the studies conducted on these co-factors are mostly observational and should be revisited. On the other hand, the known progression of HPV to cervical cancer provides opportunities for developing better screening techniques and possibly a single dose, multivalent vaccine that would protect against 98% of HPV types. The session closed with take-home points emphasizing the need for better doctor-patient interactions, good policies translating to good practice, and keeping the public scientifically educated.
Am J Obstet Gynecol. 2018 Mar 2. pii: S0002-9378(18)30176-5.
Session 4: Female Genital Schistosomiasis (FGS)
Speakers
Jennifer Downs, MD, PHD Weill Cornell Medical College
Eyrun Kjetland, MD, PhD University of KwaZulu-Natal, South Africa
Pragna Patel, MD US Centers for Disease Control and Prevention
Female Genital Schistosomiasis: A Burning Sensation, Malodorous Discharge and Bleeding from a Waterborne Parasite
The final session of the symposium shifted towards the intersection of HIV and Female Genital Schistosomiasis (FGS). Eyrun Kjetland, from the University of KwaZulu-Natal, South Africa, explained that urogenital schistosomiasis, a largely African, waterborne, parasitic disease that can cause Female Genital Schistosomiasis (FGS), affects the cervix, fallopian tubes, and the urinary tract. The cycle of FGS begins with eggs released with urine or feces in fresh water rivers or lakes. These eggs hatch, releasing larvae that infect snails and multiply into many cercariae parasites. The parasites then penetrate human skin and lay eggs inside the body, which typically penetrate the cervix and appear as grainy, sandy patches on the vaginal wall. In a cross-sectional study in a Zimbabwean community, 41% of women with FGS were also HIV+. Importantly, FGS, which may mimic the symptoms of cancer and sexually transmitted infections is not limited to adult women. Young girls aged 10-12 typically contract it and can develop symptoms including: intravaginal lesions, malodorous discharge, bloody discharge, a burning sensation in the genitals, and ulcers. Affected young girls grow into adulthood with damaged genitals and may experience infertility and ectopic pregnancy. Starting treatment at a young age can help reduce contact bleeding and decrease CCR5-HIV receptor expression in CD4+ cells, a receptor used by HIV to enter and infect host cells.
HIV and Schistosomiasis: Summary of the Evidence
Jennifer Downs, of Weill Cornell Medical College, summarized evidence from epidemiological studies in sub-Saharan Africa on the relationship between FGS and HIV. To date, three studies have found an increased odds of being HIV-infected of at least 2.9 in women with FGS by measuring either parasite eggs or circulating anodic antigen, a carbohydrate produced in the gut of adult schistosome worms. A similar study in men failed to find a significantly increased odds of HIV infection, highlighting that the intersection between schistosomiasis and HIV specifically affects women. Work done in macaque monkeys with pre-existing Schistosoma mansoni infections showed that when they were rectally inoculated with increasing doses of simian HIV (sHIV), they became sHIV-infected at a dose 17 times lower than macaques without schistosomiasis. Furthermore, the monkeys infected with Schistosoma mansoni showed increased HIV viral replication. Downs reported results from a nested case-control study situated within a longitudinal study in adults of reproductive age since 1994 in Kisesa, Tanzania. In the longitudinal study, participants are tested for HIV every three years and have blood spots stored for additional analyses, allowing researchers to compare individuals who recently contracted HIV to matched controls that didn’t contract HIV during this period. Downs and colleagues documented that the prevalence of the schistosome infection at the time of HIV-seroconversion was higher among HIV-1 female seroconverters but not males. Seroconverters with schistosome infection also have higher HIV-1 RNA levels at the time of HIV diagnosis. Hence, this study has been vital in extending findings on schistosomiasis from animal models to humans.
The results of a longitudinal study on schistosomiasis and HIV underscore the importance of understanding the intersection between these diseases.
Schistosomiasis and HIV Transmission: A Call for Research
The dearth of research on schistosomiasis and HIV transmission is a problem for this largely African epidemic. Schistosomiasis affects more than 230 million people worldwide, 90% of whom are in Africa. Pragna Patel, of the CDC, highlighted that there is not enough epidemiological evidence in terms of incidence and prevalence of FGS and HIV. Furthermore, due to decreasing child mortality, the youth population in sub-Saharan Africa will double by 2020 from the start of the HIV epidemic in 1990. This increase in the size of vulnerable populations and the fact that young girls typically contract FGS through freshwater contact with recurrent exposures throughout their lifespan, requires improved treatment of FGS to reduce HIV infections in the future. Patel made a call for research on the effect of FGS and its treatment on HIV acquisition, particularly among adolescent girls and young women.
Adolescent girls are a vulnerable population for HIV infection.
Next Steps: Research, Policy, Activism
The final session ended with an open discussion in which audience members dove deeper into the current understanding of schistosomiasis by asking questions on its transmission and overlap with HIV. The speakers noted that while men are less likely to have schistosomiasis, those who do, tend to have bloody semen, making it more likely that they transmit HIV. This intersection with HIV can be leveraged to provide more widespread treatment of schistosomiasis. Kjetland mentioned a current randomized trial she is conducting in African communities which uses a thorough questionnaire to identify potential confounds in kids with schistosomiasis. Such trials can catch cases at an early stage and provide consistent treatment. Downs called attention to the WHO guidelines for treating schistosomiasis, which indicate that in communities with prevalence above 50%, treatment should be provided twice a year to all community children. Yet, less is done to diagnose and treat adults with schistosomiasis. Pragna mentioned that the DREAMS initiative for adolescent girls and young women, which is currently implemented in a number of African communities, could be anchored to create an integrative package to educate women on HPV, cervical cancer, HIV, and schistosomiasis. These types of initiatives along with good policies can greatly reduce prevalence and stigma of female-reproductive diseases around the world.
Scientists, ethicists, and other experts gather to discuss the promises and potential consequences of advances in biotechnology and artificial intelligence aimed at improving human performance.
New York, NY | May 10, 2018 — From eyeglasses that restore sight to robotic prosthetics to replace limbs, people throughout history have sought to overcome the limitations of the human body. New advancements in such technologies and their implications will be explored at “The Enhanced Human: Risks and Opportunities,” presented by the Aspen Brain Institute, The Hastings Center, and The New York Academy of Sciences at the Academy’s headquarters on Monday, May 21 at 6:00pm.
This evening event will include short presentations and a panel discussion examining the scientific and ethical implications of existing and rapidly emerging technologies with applications for human enhancement. Special emphasis will be placed on CRISPR/Cas9 gene editing technology and artificial intelligence. Experts from multidisciplinary fields will provide historical perspective and scientific background before discussing the vast opportunities of these cutting edge technologies and delving into the complex ethical and social questions still to be addressed.
The program will begin with introductory sessions on “The History and Science of Human Enhancement” and “Present and Future Bioethical Considerations,” featuring brief talks from renowned geneticist George Church (Wyss Institute at Harvard University), biomedical ethics and policy expert Josephine Johnston (The Hastings Center), technology futurist Jamie Metzl (Atlantic Council), and artificial intelligence specialist Meredith Whittaker (AI Now Institute at NYU).
These introductory sessions will be followed by a lengthy panel discussion moderated by Mildred Z. Solomon, distinguished health care and science policy expert and president of The Hastings Center. The panel is comprised of the aforementioned speakers and Glenda Greenwald, president and founder of the Aspen Brain Institute. A speaker networking reception will close the event. For those unable to attend the event in person, the event will be available via Livestream.
This event was made possible, in part, through the support of a grant from the John Templeton Foundation. The opinions expressed are those of the presenters and do not necessarily reflect the views of the John Templeton Foundation.
About the Aspen Brain Institute
The Aspen Brain Institute convened its first meeting co-presented with The New York Academy of Sciences in 2010 focused on Neurotechnology: Building Better Brains. Since 2010, the Aspen Brain Institute has partnered with the Academy on six symposia and a social impact challenge. As a 501(c)(3) non-profit organization, the Aspen Brain Forum Foundation supports and produces scientific meetings covering topics ranging from neuroprosthetics to the developing human brain. The Foundation’s mission is to:
Organize, produce, and host an annual high-level meeting of international brain researchers, in partnership with The New York Academy of Sciences, leading to global collaborations and breakthroughs in world brain science.
Present and disseminate the most cutting-edge innovations in brain science.
Ally with large new initiatives, such as the American Brain Coalition, the American Brain Foundation, and One Mind for Research, to prevent and cure brain disorders such as Alzheimer’s, Parkinson’s, autism, and depression, within a decade.
About The Hastings Center
The Hastings Center addresses fundamental ethical and social issues in health care, life sciences research, and biomedical technologies. The Center’s goal is to promote compassionate and just health care and the wise use of emerging technologies. Through its scholars’ writing and speaking, and through the work of the many people from around the world who participate in its projects or submit articles to its two journals, The Hastings Center shapes ideas that influence key opinion leaders, including health policymakers, regulators, lawyers, legislators, and judges, as well as health care executives, physicians and nurses. Founded in 1969 by philosopher Daniel Callahan and psychoanalyst Willard Gaylin, The Hastings Center is the oldest independent, nonpartisan, interdisciplinary research institute of its kind in the world. In addition to producing original research, it accomplishes its mission through public engagement and service to the field of bioethics. To learn more, please visit www.thehastingscenter.org.
Many promising strategies for promoting neuroregeneration have emerged in the past few years, but a further research push is needed for these ideas to be translated into therapies for neurodegenerative diseases.
On June 13–14, a symposium presented by Eli Lilly and Company and The New York Academy of Sciences brought together academic and industry researchers working on multiple neurodegenerative diseases as well as clinicians and government stakeholders to discuss cutting edge basic and clinical research on neuroregeneration and neurorestoration. Topics included neuronal plasticity, inflammation, glial cell function, autophagy, and mitochondrial function, as well as analysis of recent drug development failures and how to move forward from them.
Speakers
Benedikt Berninger, PhD, University Medical Center Johannes Gutenberg University Mainz, Germany
Graham Collingridge, PhD, University of Toronto
Ana Maria Cuervo, MD, PhD, Albert Einstein College of Medicine
Valina Dawson, PhD, Johns Hopkins School of Medicine
Roman Giger, PhD, University of Michigan
Steven Goldman, MD, PhD, University of Rochester Medical Center
Eric Karran, PhD, AbbVie
Arthur Konnerth, PhD, Technical University of Munich, Germany
Guo-li Ming, MD, PhD, Johns Hopskins School of Medicine
David Rowitch, MD, PhD, ScD, University of Cambridge and University of California, San Fransisco
Amar Sahay, PhD, Massachusetts General Hospital
Reisa A. Sperling, MD, MMSc, Brighman and Women’s Hospital
James Surmeier, PhD, Northwestern University
Richard Tsien, DPhil, New York University, Longone Medical Center
Jeffrey Macklis, Harvard University
Mark Mattson, National Institute of Aging
Clive Svendsen, Cedars-Sinai Medical Center
Michael Sofroniew, David Geffen School of Medicine, UCLA
Michael J. O’Neill, Eli Lilly and Company
Presented By
Meeting Reports
Meeting Reports
Astrocytes in CNS Repair; Disease-Modifying Therapies in the Pipeline
Speakers
Eric Karran AbbVie
Michael V. Sofroniew David Geffen School of Medicine, University of California, Los Angeles
Highlights
Astrocyte scar formation is not detrimental to neuronal regeneration and repair after injury but is in fact critical to the healing process.
The clinical pipeline in Alzheimer’s disease is dominated by amyloid beta-targeting compounds, despite the fact that the approach has not been successful to date.
Astrocytes in CNS Repair
In his keynote talk, Michael V. Sofroniew of the University of California, Los Angeles, described 25 years of work on the overlooked and misunderstood role of astrocytes in the central nervous system (CNS).
These glial cells were discovered in the 19th century, and researchers widely believed that their activation after injury—which often results in scar formation around the lesion—detrimentally affects recovery. “But one has to ask, why would nature conserve this response to injury across all mammalian species if it were purely detrimental?” Sofroniew said.
Astrocytes can play fundamentally different roles in the CNS. In healthy tissue, they help synapses take up and release neurotransmitters and other factors, and help maintain neuronal energy balance and blood flow in surrounding tissue. Their activation in response to damage differs depending on whether recovery requires neurons to grow through lesioned tissue or through intact neural tissue.
Two different phenotypes of reactive astrocytes occur after injury.
Astrocytes responding to injury exist in different phenotypes: a hypertrophic reactive form interacts with neural cells, and a scar-forming reactive form interacts with non-neuronal inflammatory and fibrotic cells. Researchers are just beginning to define the function of hypertrophic astrocytes, but Sofroniew and his colleagues hypothesize that they represent a beneficial gain of function—helping injured neurons make new synapses and reorganize damaged circuits. Much remains to be learned about this process, he said.
Ongoing research from Sofroniew’s lab suggests that scar-forming astrocytes have a different, also beneficial function: recruiting inflammatory cells into the tissue, regulating their activity, and restricting their spread outside the lesion. Inflammation is crucial for getting rid of damaged cells, but too much of it damages surrounding intact tissue.
When neural tissue is injured, astrocytes recruit cells to scavenge damaged tissue. Somehow, astrocytes sense where the border between damaged and healthy tissue should be and wall off the injury with scar tissue. Sofroniew and others have shown that disrupting scar formation causes neurons in surrounding tissue to die.
Entrenched dogma in the field, however, says that astrocyte scar formation prevents axon regeneration. Twenty years ago, Sofroniew’s lab first tested whether disrupting scar formation in mice would spur injured axons to spontaneously regenerate. Their results showed that it didn’t, but the findings went against current dogma so the team never published them. When a researcher interested in the question joined the lab recently, they began exploring the question again, using two mouse models with mutations that prevent scar format.
After a spinal cord injury, sensory axons stimulated with growth factors can regrow despite astrocyte scar formation.
They showed that axons in three different types of CNS tracts failed to regrow in the mutant mice. Both astrocytes in lesions, along with other, non-astrocyte cells, all produced a variety of molecules both promoting and inhibiting axonal growth, underscoring the multi-component nature of regeneration. And axons that received appropriate stimulatory molecules “grow happily across astrocyte scars,” he said. The group is now confirming the result in additional types of CNS tracts. Sofroniew concluded that astrocyte reactivity and scar formation are not forms of astrocyte dysfunction, but adaptive functions critical for CNS repair and regeneration after injury.
Disease-Modifying Drugs for Alzheimer’s Disease: An Industry Perspective
The 1990s were a rich decade of discovery in Alzheimer’s disease, said Eric Karran of the pharmaceutical company AbbVie. Researchers identified disease-causing autosomal dominant mutations in the amyloid precursor protein presenilin and in tau. The field began to uncover key mechanisms and targets, and many believed that the next decade would yield effective therapeutics. However, that has not transpired, and many uncertainties about Alzheimer’s disease drug development remain.
Researchers still puzzle over the relationship between tau pathology and amyloid beta deposition. And while evidence suggests that Apolipoprotein E (ApoE) is closely involved in amyloid beta pathology, the mechanistic details remain mysterious. Nonetheless, research on the autosomal dominant mutations has geared drug discovery toward the idea that amyloid deposition initiates the disease process. Yet it is not clear that amyloid beta is an effective target for people who already have symptoms of Alzheimer’s disease.
Three questions are critical for therapeutics targeting amyloid: at what stage of the disease is such a drug most likely to be effective, by how much should amyloid beta be lowered, or its clearance be facilitated, and what kind of clinical experiment will test the validity of the amyloid cascade hypothesis.
Karran made a distinction between onset and duration of the disease. Possibly, amyloid beta deposition initiates the disease, he said, but is not the factor that drives its progression. The amyloid cascade hypothesis has many permutations, making proving or disproving it particularly difficult. One clear sign of this is the multiple failed trials that targeted amyloid beta. Lilly’s solanezumab seemed to show a mild effect on cognitive decline, but the signal was too small for a phase 3 trial. One currently promising candidate is Biogen’s aducanumab, which showed time- and dose-dependent reduction of amyloid plaques in early-stage trials.
Tau binpathology correlates with disease progression, but amyloid does not.
A drug that intervenes with the onset and spread of tau pathology could potentially have therapeutic value relatively late in disease. Tau pathology is the most proximate marker for neuronal loss and cognitive impairment. Tau proteins are released by a currently unknown mechanism; how they are seeded and travel to distant neurons is also poorly understood. The process points to several points of interventions, such as anti-tau antibodies targeting seeds or fibrils. However, early efforts at tau therapeutics have failed.
Speaker Presentation
Further Readings
Michael Sofroniew
Anderson MA, Burda JE, Ren Y, Ao Y, O’Shea TM, Kawaguchi R, Coppola G, Khakh BS, Deming TJ, Sofroniew MV.
Dendritic Spines, Axons, and Synapses in Neuroplasticity
Speakers
Richard Tsien New York University Langone Medical Center
Roman J. Giger University of Michigan School of Medicine
Jeffrey Macklis Harvard University
James Surmeier Feinberg School of Medicine, Northwestern University
Highlights
Neuronal cell bodies regulate events at the synapse via the CamKII signaling pathway.
Imperfect adaptation to the gradual loss of dopaminergic neurons in the striatum drives Parkinson’s disease symptoms
Dectin1, a receptor expressed on the surface of macrophages, mediates a neuroregenerative immune response after injury.
Growth cones may contain autonomous machinery for building the neuronal circuitry of the brain.
Regulation of Synapses and Synaptic Strength
Understanding the neural circuitry underlying learning and memory requires understanding how neurophysiological events at the synapse are integrated with molecular events in the nucleus such as gene transcription and protein translation, said Richard Tsien of New York University. At the synapse, this process depends on the combined activation of glutamate receptors and so-called L-type calcium channels. Tsien’s lab discovered that such dual activation is coordinated by the mobilization of a molecule called CamKII—known to be a key player in learning and memory—around tiny protrusions from dendrites called dendritic spines.
Tsien and his colleagues then elucidated how the signal from this synaptic activity is conveyed to the nucleus. Two of the four known forms of CamKII do their jobs at the synapse, but a third form, called gamma CamKII, shuttles calcium and its binding partner calmodulin to the nucleus, where it initiates a signaling cascade that drives the transcription of genes involved in long-term potentiation, a key molecular mechanism underlying learning and memory. Mice mutated to lack gamma-CamKII showed reduced learning and memory and did not upregulate key genes after training in memory tasks.
Mice mutated to lack gamma-CamKII showed reduced learning and memory and did not upregulate key genes after training in memory tasks.
A mutation in gamma CamKII has been linked to intellectual disability in humans; studies on this human mutation revealed that it prevented the protein’s ability to shuttle calcium / calmodulin. Mutations in multiple proteins on this CamKII signaling pathway have been causally implicated in neuropsychiatric disorders such as autism, pointing to its importance in linking neuronal activity with nuclear processes.
Striatal Plasticity in Parkinson’s Disease
The core motor symptoms of Parkinson’s disease (PD) are caused by the loss of dopaminergic neurons in a brain region called the striatum. James Surmeier of Northwestern University described his lab’s research on how the two main pathways of the striatum—the direct (dSPN) and the indirect (iSPN) pathway—maintain homeostasis as the disease progresses.
Dopaminergic signaling in the striatum helps regulate goal-directed behaviors. The dSPN promotes desired actions, while the iSPN suppresses undesired actions, and the two must remain balanced for appropriate action selection to occur. Dopamine helps provide that balance. When its levels are high, it promotes long-term potentiation (LTP) of the dSPN (increasing choice of good actions) and long-term depression (LTD) of the iSPN (limiting opposition to them). When levels fall, the opposite occurs, quashing the selection of “bad” actions. Surmeier’s lab studies what drives LTP and LTD at these synapses by visualizing them. Only a subset of synapses is responsive to dopamine, they found.
Dopamine differentially affects the dSPN and iSPN via D1 and D2 receptors.
According to the standard model of Parkinson’s, loss of striatal neurons changes the excitability of the dSPN and iSPN, leading to suppression of motor activity. However, this model fails to account for how the system might compensate for its gradual deterioration. Such compensation may explain why the striatum must lose more than 60% of its dopaminergic cells before a person shows symptoms of the disease, Surmeier said. His work instead suggests that the dSPN and iSPN undergo a more graded but imperfect adaptation to the loss of dopaminergic innervation which distorts the information that these pathways receive, and which may cause deficits in goal-directed behavior before gross motor symptoms appear.
Immune-mediated Nervous System Regeneration
There is no spontaneous regeneration after nerve injury in the central nervous system. That is probably because extrinsic factors exist that block regeneration intrinsic factors that promote it are not activated, said Roman J. Giger of the University of Michigan School of Medicine. However, some types of inflammation can activate such regeneration factors.
His team found that an injection of zymosan (a mixture of proteins and carbohydrates prepared from the yeast cell wall) induced significant long-distance regeneration after optic nerve injury in mice, while the bacterial extract lipopolysaccharide did not. He and his colleagues found that this regenerative antifungal response is mediated primarily by a dectin-1, a receptor for a substance called beta glucan, which is expressed on the surface of macrophages and other immune cells, as well as by the immune recognition protein Toll-like receptor 2 (TLR2).
They also found this mechanism in spinal cord regeneration, as tested after a so-called conditioning injury to the sciatic nerve (which activates immune response genes) followed by a spinal cord lesion at the dorsal root ganglion. Wild type mice showed significant spinal cord axon regrowth after zymosan injection, while mice engineered to lack dectin-1 or TLR2 showed none.
Wild type mice showed significant spinal cord axon regrowth after zymosan injection, while mice engineered to lack dectin-1 or TLR2 showed none.
The researchers then tried to pinpoint which immune cell types produced dectin-1, and where it had to be localized to spur regeneration. They found that immune cells from the sciatic nerve—that is, the conditioning lesion—carried the signal. Although mice lacking dectin showed no regeneration, immune cells from the lesioned sciatic nerve of a wild type mouse transplanted into the dectin-1 knockout mouse could rescue this deficit.
Growth Cone Control over Circuit Development
Building the brain’s neuronal circuitry is enormously complex endeavor: neurons exist in a multitude of diverse subtypes, they project to precise sompatotopic targets, and some send projections to more than one specific location. Projections can be up to a meter in length – some 10,000 cell body diameters away. The system’s precision is astounding, said Jeffrey Macklis of Harvard University, and being able to rebuild circuits when they go awry is key to regeneration in the face of injury or disease.
Macklis described work showing that the transcriptional machinery that generates this complexity is present not just in the neuronal cell body, but also in growth cones located at the tips of projections as they extend. His lab has found that growth cones contain locally translated proteins, suggesting that these neuronal outposts might exert autonomous control over circuit development. “As a developmentalist, I view growth cones as little baby synapses,” Macklis said.
Immature axons transplanted in the developing mouse still project to their original, appropriate targets, suggesting a logic and subtype specificity to the process. Macklis’s lab came up with an approach to label and isolate growth cones from different neuronal subtypes. They found specific protein and RNA enriched at growth cones that was not present in the neuronal cell body, suggesting a localized projection machinery. Targeting this machinery could be an important strategy for promoting regeneration.
Inflammation, Oxidative Stress, Mitochondrial Function, and Autophagy
Speakers
Ana Maria Cuervo Albert Einstein College of Medicine
Valina L. Dawson Johns Hopkins University
Mark Mattson National Institute of Aging
Highlights
Fasting and exercise exert protective effects on the brain and improve the bioenergetics properties of neurons.
Activators of a selective autophagy process may help clear aggregating proteins implicated in neurodegenerative disease.
A key cluster of Parkinson’s disease proteins regulate mitochondrial biogenesis and function.
Bioenergetic Challenges Bolster Brain Resilience
Mark P. Mattson of the National Institute of Aging described how two bioenergetics challenges—food deprivation and exercise—affect brain health. The ability to function under conditions of food deprivation is the main driving force in brain evolution, he said: Fasting was frequent, and it drove humans to search for food. Aging is a major risk factor for dementia and stroke, but sedentary lifestyles contribute as well, by compromising cells’ ability to adapt to the molecular stresses of aging.
Increased exercise is known to boost brain levels of the neuroprotective factor BDNF, and early work in Mattson’s lab found that fasting has the same effect in mice. Also, in mice genetically engineered to be obese and diabetic, alternate day fasting and increased exercise on a running wheel increased the density of synaptic spines in their brain. Further work showed that fasting and exercise also increased the number of mitochondria—the cell’s energy-generating organelles—in cultured hippocampal neurons.
The brains of mice lacking Sirt3 experience more cell death (blue) upon excitotoxic treatment with glutamate, kainic acid, and NMDA.
More recently, Mattson’s lab found that exercise and intermittent fasting upregulate a mitochondrial protein called sirtuin 3 (sirt3), which goes on to block enzymes that protect the mitochondria against stress and protect cells against apoptosis. The group has also explored the effects of fasting in humans. Currently, the group is studying whether people at risk for cognitive impairment due to age or metabolic status benefit from fasting two days per week.
Malfunctioning Autophagy Pathways in Neurodegeneration
Autophagy is the process of degradation or recycling of materials inside the cell, and many facets of it are coming under scrutiny as causal factors in neurodegeneration. Ana Maria Cuervo of the Albert Einstein College of Medicine studies chaperone-mediated autophagy (CMA), in which individual proteins targeted with a degradation motif are recognized by a chaperone protein, carried to a receptor called LAMP-2A on the lysosome surface, and pulled inside for degradation. In order to study the role of CAM in neurodegeneration, Cuervo’s lab designed a fluorescent reporter system that can track the process in vivo, in the brain and other organs.
A fluorescent reporter technique developed by Cuervo lab allows researchers to observe chaperone-mediated autophagy in different tissues of a live mouse.
The CAM pathway is highly sensitive to aging; levels of the LAMP-2A receptor drop as animals age. Additionally, many proteins involved in neurodegenerative diseases have CMA degradation motifs. The mutant form of LRRK2, the protein most often mutated in familial cases of Parkinson’s, interferes with LAMP-2 receptor’s ability to form complexes as required for translocation into the lysosome; other neurodegeneration-related proteins, such as tau, showed a similar effect, which led to an aggregation of these proteins due to their inability to be broken down inside the lysosome. Human postmortem Alzheimer’s disease brains also appear to have a CMA deficit.
The lab has now developed a selective activator of the CAM pathway and is administering it to a mouse model of Alzheimer’s disease. The intervention ameliorates behavioral symptoms such as anxiety, depression, and visual memory in the animals, as well as cellular markers of the disease.
Mitochnodrial Mechanisms and Therapeutic Opportunities
Mitochondrial dysfunction was first observed in Parkinson’s disease some 40 years ago, but how it plays a role in the disease is unknown. Some genetic causes of PD have been identified, including mutations in Parkin and PINK1. Valina L. Dawson’s lab at Johns Hopkins University is investigating how three closely interacting proteins, Parkin, PINK1, and PARIS, regulate mitochondrial function and, in turn, the integrity of dopaminergic neurons, which malfunction in PD.
In 2011, Dawson’s lab identified PARIS, a protein that tamps down mitochondrial production by repressing another protein called PGC1-alpha. PARIS is ubiquitinated by Parkin to remove the brake on mitochondrial production. Mice genetically engineered to lack Parkin show age-dependent loss of dopaminergic neurons and serve as a model of PD. But if these mice also experience a knock-down in PARIS, the deficit is rescued. Loss and gain of function studies of these proteins in mice revealed a homeostasis between them that regulates mitochondrial biogenesis and function. Pink1 is also central; it must phosphorylate Parkin for this homeostasis to occur.
In human neuron lacking Parkin, knocking down PARIS restores mitochondrial deficits.
The relationships between these proteins also hold in human embryonic stem cells when these proteins are knocked down, and in induced pluripotent cells derived from Parkinson’s patients with mutations in these proteins. Based on these findings, Dawson’s team and collaborators are exploring whether PARIS inhibitors, Parkin activators, or other molecules affecting this protein network have therapeutic value in PD mice.
Speaker Presentations
Further Readings
Mark Mattson
Cheng A, Yang Y, Zhou Y, Maharana C, Lu D, Peng W, Liu Y, Wan R, Marosi K, Misiak M, Bohr VA, Mattson MP.
Cell Rep. 2017 Jan 24;18(4):918-932. doi: 10.1016/j.celrep.2016.12.090.
Glial Function
Speakers
Steven A. Goldman University of Rochester Medical Center
David H. Rowitch University of Cambridge
Clive Svendsen Cedars-Sinai Medical Center
Highlights
Glial cell dysfunction may causally contribute to schizophrenia and other neurological diseases.
Astrocytes engineered to produce GDNF are in clinical trials for treating amyotrophic lateral sclerosis.
Astrocytes are functionally and regionally heterogeneous, and their dysfunction may contribute to neurodegenerative disease.
Targeting Glial Cell Dysfunction in Neurological Disease
Glial cells make up a significant proportion of cells in the brain, yet their contribution to disease is poorly understood. Steven A. Goldman of the University of Rochester Medical Center studies glia’s role in brain diseases such as schizophrenia. His lab injects human glial progenitor cells into the brains of mutant mice that lack their own glia; the brains of the resultant chimeras become fully repopulated with human astrocytes and oligodendrocytes. This human glial chimera maintains the phenotypes of human glial cells, and mice with human glia show stronger long-term potentiation in the hippocampus and learn fear-conditioning and other behavioral and cognitive tasks more quickly than wildtype mice.
Astrocytes in mice populated by glial cells derived people with schizophrenia had different morphology than those derived from control subjects, with fewer and longer processes.
Goldman’s team created chimeric mice populated by glia derived from eight different people with juvenile onset schizophrenia, and compared them to mice with glial cells derived from control subjects. These glial precursor cells migrated abnormally and formed less myelin than precursors from control human subjects. Myelin-producing and glial differentiation genes, as well as genes associated with synaptic development and transmission, were downregulated. Astrocytes in the patient-derived chimeras also had irregular morphology. The animals exhibited impaired response to stimuli as well as anxiety and antisocial behavior. Genes related to glial cells might be potent therapeutic targets for schizophrenia and other diseases, like Huntington’s disease and frontotemporal dementia.
“We never thought of these as glial diseases, but fundamentally they might be,” Goldman said.
Stem-cell-derived Astrocytes for Treating Neurodegenerative Disease
Ninety percent of neurodegenerative diseases have no known genetic cause, and may be amenable to treatment with cell therapy, said Clive Svendsen of Cedars-Sinai Medical Center. While delivering neurons into diseased CNS is still evolving, astrocytes have great potential for immediate use, Svendsen said.
His lab developed a protocol for deriving astrocytes from human fetal tissue; these cells migrate to areas of damage when delivered to a rat brain. To give these cells more regenerative capacity, Svendsen and collaborators engineered the cells to release the growth factor GDNF. They initially tested this cell delivery therapy in a Parkinson’s disease model, but it has also been applied in stroke, and both Huntington’s and Alzheimer’s disease.
More recently they have begun to explore its use in amyotrophic lateral sclerosis (ALS), where life expectancy after diagnosis is a mere three years and no treatments exist. They first tested it in an ALS rat transgenic model in which astrocytes lacked the protein SOD1. When they transplanted the therapeutic astrocytes to the lumbar spine, the cells survived well and improved neuronal survival, but did not prevent paralysis. As they moved up the spinal cord, results improved; cell delivery into the brain’s motor cortex yielded improved motor function and survival in the animals.
GDNF-releasing astrocytes injected into the motor cortex spur motor neuron growth in a rat model of ALS.
Last October, Svendsen and his team launched an 18-person clinical trial of this approach. For safety reasons, the U.S. Food and Drug Administration required the researchers to start by delivering cells into the lumbar spine; patients will receive the therapy in one leg, with the other acting as a control. If the first few patients experience no adverse effects, delivery into the cervical spine and the cortex will also be attempted.
Functionally Heterogeneous Astrocytes in the Mammalian CNS
How neuron patterning generates a diversity of neuronal types throughout the central nervous system is well understood. But very little is known about heterogeneity in astrocytes, although they are the most abundant cells in the CNS, comprising about half of all brain cells, said David H. Rowitch of the University of Cambridge.
Early work in Rowitch’s lab identified an astrocyte-specific transcription factor that showed that astrocytes are allocated to specific regions of the brain during development. They then searched for postnatal astrocytes in the spinal cord that were regionally and functionally distinct by comparing gene expression in the dorsal and ventral part of the spinal cord. The gene Sema3a was most highly expressed in ventral astrocytes in mice, and when it was deleted, half the animal’s alpha motor neurons, which innervate fast-twitching muscle, died.
Mice lacking Kir4.1 have abnormal signaling in motor neurons, smaller muscle fibers, and decreased strength.
To investigate how neurons and astrocytes interact, the researchers examined a potassium channel called Kir4.1, which is preferentially expressed in the ventral brain and spinal cord. Loss of function mutations to the channel cause epilepsy, and the channel is strongly downregulated in astrocytes of people with ALS. Mice engineered to lack the channel in astrocytes have smaller alpha motor neurons and weaker muscle function. Transfecting the astrocytes of these mice with the channel reverses these deficits. The fact that astrocytes so strongly affect neuron function suggests that dysfunction in specific subsets of astrocyte may play a role in neurodegenerative diseases.
Speaker Presentations
Further Readings
Steven Goldman
Han X, Chen M, Wang F, Windrem M, Wang S, Shanz S, Xu Q, Oberheim NA, Bekar L, Betstadt S, Silva AJ, Takano T, Goldman SA, Nedergaard M.
Science. 2012 Jul 20;337(6092):358-62. doi: 10.1126/science.1222381. Epub 2012 Jun 28.
Innovative Approaches to Promote Neuroregeneration
Speakers
Graham Collingridge University of Toronto
Guo-li Ming University of Pennsylvania
Benedikit Berninger Johannes Gutenberg University Mainz
Amar Sahay BROAD Institute of Havard and MIT
Highlights
Novel therapies targeting the synaptic plasticity pathways could address the dysregulation of long term depression underlying Alzheimer’s disease.
Brain organoids grown from human induced pluripotent stem cells recapitulate development and can model brain disease.
Reprogramming pericyte cells into neuronal cells occurs via a distinct developmental program.
Promoting neurogenesis and re-engineering molecular connectivity in the hippocampus restored age-related memory decline in mice.
Is Alzheimer’s Disease Caused by Long Term Depression Gone Awry?
One key purpose of brains is to enable learning and memory—a process that relies on a balance between long term potentiation (LTP) and long term depression (LTD) to drive synaptic plasticity, said Graham Collingridge of the University of Toronto. Dysregulation of that balance causes Alzheimer’s disease, he said.
In 1983, Collingridge’s lab identified the role of the NMDA receptor in synaptic plasticity, finding that its activation could cause both LTP and LTD. In later work, they sought kinase inhibitors that could block LTP and LTD. One of the few ways to inhibit LTD was to block glycogen synthase kinase 3beta (GSK-3beta). This molecule is also known as tau kinase because it hyperphosphorylates the protein tau—a process implicated in Alzheimer’s disease pathogenesis. “I thought, well, that’s just not coincidence, is it,” Collingridge said.
Dysregulation of the pathway regulating LTD can cause the pathogenic features of Alzheimer’s disease.
Tau regulates microtubules in axons, but Collingridge’s lab found that it also exists in synapses, and is phosphorylated by GSK-3beta. In mice engineered to lack tau, LTD is absent but LTP is undisturbed. Work from other researchers had shown that amyloid beta, the protein that aggregates in Alzheimer’s disease, inhibits LTP and facilitates LTP. His group showed that GSK-3beta reverses this effect, and identified other parts of the signaling pathway linking amyloid beta, tau, GSK-3beta, and both LTP and LTD. Dysregulation in these components can generate amyloid beta plaques, tau tangles, and the neuroinflammation, synapse loss and memory loss that characterizes Alzheimer’s. Modulators of NMDA receptor activity may have therapeutic potential.
Modeling Human Brain Development and Disease with Human Induced Pluripotent Stem Cells
Guo-Li Ming of the University of Pennsylvania is developing 3-dimensional cell culture models of the developing brain—so-called organoids—using induced pluripotent stem cells. High school students working in her lab designed 3D-printed lids with shafts that insert into standard cell culture plates, to divide each individual well of the plate into a separate miniaturized spinning bioreactor. Because most brain organoid protocols produced highly heterogeneous tissue, she used these tiny bioreactors to create organoids containing almost exclusively forebrain tissue.
Using markers specific to different layers of the cerebral cortex, Ming’s lab could show that organoids roughly recapitulated the cortical architecture.
Cell labeling and gene expression studies showed that when grown for 100 days, these organoids recapitulated fetal forebrain development through the end of the second trimester. Progenitor cells generated neurons and glia whose migration pattern mirrored development, and the neurons received both excitatory and inhibitory input. The researchers used the organoids to study how Zika virus affects the developing brain. They found that the virus specifically targets neural progenitor cells, dose-dependently causing cell death and causing a collapse of tissue that resembles the microcephaly in infants affected by Zika. A screen of 6000 compounds yielded a neuroprotective compound called Emricasan that is positioned to enter clinical trials.
The group has now developed other brain-region specific organoids, modeling the midbrain and the hypothalamus. They plan to use these tools to study other neurodevelopmental disorders. Recent publications suggest the approach can also recapitulate features of neurodegenerative diseases, Ming said.
Engineering Neurogenesis via Lineage Reprogramming
For the past decade, Benedikit Berninger of Johannes Gutenberg University Mainz has been working on identifying cellular signals that can drive the reprogramming of astroglial cells from early postnatal mouse brain into neurons. More recently, to see if such reprogramming could be conducted in human cells, his lab began working with cells derived from adult human brains during epilepsy surgery. These cells turned out to be pericytes, and Berninger’s team identified a two transcription factors—Sox2 and Ascl1—that could reprogram them into functional neurons, which formed synapses and fired action potentials in culture.
To understand how the two transcription factors interact, the researchers investigated gene expression in the early stages—day 2 and day 7—in this two-week reprogramming process. A few genes were regulated by just one of the factors, but most were turned on only when both factors were present, suggesting that the two factors act synergistically. Ascl1 alone appears to target a different set of genes—ones associated with mesodermal cell fate (which generate pericytes), rather than neurogenesis-related genes activated when Ascl1 is co-expressed with Sox2. A similar difference was seen on a single cell level.
The researchers also observed two subpopulations in the starting population of pericytes—one of which was susceptible to reprogramming into neurons while the other was not. That may account for distinct competence in reprogramming in individual cells, Berninger said. For example, cells expressing the leptin receptor had a low level of reprogramming efficiency, indicating subtype differences in reprograming competence.
Three sets of genes are induced during reprogramming of pericytes to neurons—a set associated with pericytes, one associated with a progenitor-like stage, and one associated with neurons.
In the subset of cells that do reprogram successfully, a set of genes was induced transiently, then downregulated. These genes reflect a progenitor-like stage in the reprogramming process. These studies suggest that cells are not transforming directly from pericyte to neuron, but undergo a series of events reminiscent of an unfolding developmental program, Berninger said.
Rejuvenating and Re-engineering Aging Memory Circuits
The hippocampus plays a critical role in formation of episodic memories-that is, memories of what, when, and where. Essential to this capacity is the need to keep similar memories separate and retrieve past memories in a context appropriate manner. With age, the ability to keep similar memories separate and context-appropriate retrieval is potentially impaired, said Amar Sahay of Massachusetts General Hospital and Harvard Medical School. Within the hippocampus, the dentate gyrus-CA3 circuit performs operations such as pattern separation and pattern completion that support resolution of memory interference and retrieval. With age, neurogenesis in the hippocampus declines and CA3 neurons become hyper excitable in rodents, non-human primates and humans. Sahay’s lab investigates circuit mechanisms that may be harnessed to optimize hippocampal memory functions in adulthood and aging.
The DG-CA3 circuit in the hippocampus regulates episodic memory.
The hippocampus generates new neurons throughout life, and previous work has suggested that adult-born neurons integrate into the hippocampal circuitry by competing with existing mature neurons for inputs. Sahay and his colleagues identified a transcription factor called Klf9 that, when unregulated just in the mature neurons, biases competition dynamics in favor of integration of the adult-born neurons. This enhances neurogenesis in adult (3-month-old), middle-aged (12 months) and in aged (17-month-old) mice. Older rejuvenated animals (with enhanced adult hippocampal neurogenesis) had a memory advantage: they were better at discriminating between two similar contexts, one safe and one associated with a mild footshock.
In a complementary series of experiments, Sahay and his colleagues found age-related changes in connectivity between dentate granule neurons and inhibitory interneurons. They performed a screen and identified a factor with which they re-engineered connectivity between dentate granule neurons and inhibitory interneurons and augmented feed-forward inhibition onto CA3. By targeting this factor in the dentate gyrus of aged mice, the authors were able to reverse age-related alterations in dentate granule neuron-inhibitory interneuron connectivity and enhance memory precision.
Nat Neurosci. 2011 May;14(5):545-7. doi: 10.1038/nn.2785. Epub 2011 Mar 27.
Kimura T, Whitcomb DJ, Jo J, Regan P, Piers T, Heo S, Brown C, Hashikawa T, Murayama M, Seok H, Sotiropoulos I, Kim E, Collingridge GL, Takashima A, Cho K.
Philos Trans R Soc Lond B Biol Sci.2013 Dec 2;369(1633):20130144. doi: 10.1098/rstb.2013.0144. Print 2014 Jan 5.
Peineau S, Taghibiglou C, Bradley C, Wong TP, Liu L, Lu J, Lo E, Wu D, Saule E, Bouschet T, Matthews P, Isaac JT, Bortolotto ZA, Wang YT, Collingridge GL.
McAvoy KM, Scobie KN, Berger S, Russo C, Guo N, Decharatanachart P, Vega-Ramirez H, Miake-Lye S, Whalen M, Nelson M, Bergami M, Bartsch D, Hen R, Berninger B, Sahay A.
Biomarkers, Hot Topics, and the Future of Therapeutics
Speakers
Reisa Sperling Brigham and Women’s Hospital
Johanna Jackson Eli Lilly and Company
Eliška Zlámalová University of Cambridge
Arthur Konnerth Technical University of Munich
Milo Robert Smith Icahn School of Medicine at Mount Sinai
Highlights
Multimodal imaging is becoming advanced enough to identify people with early-stage disease, which will help determine the critical window for therapies in clinical trials.
Slow wave oscillations are disrupted in Alzheimer’s disease model mice due to a misregulation of excitatory and inhibitory synaptic activity.
Imaging pre- and post-synaptic structures over time can reveal how disease progression affects synapses.
Integrative bioinformatics can identify common pathways across neurodegenerative diseases and as well as drugs that can may act on those pathways.
An RNAi-based screen in Drosophila can reveal genes that shape the morphology of axonal ER.
Neuroimaging in Early Alzheimer’s Disease
Alzheimer’s disease evolves over a couple decades, but most research to date has examined the disease at a late stage—perhaps too late to intervene effectively, said Reisa Sperling of Brigham and Women’s Hospital. Multimodal imaging is becoming advanced enough to identify people with early-stage disease, which will help determine the critical window for therapies in clinical trials.
PET amyloid imaging detects amyloid pathology in humans in vivo. Some 30% of clinically normal individuals have high amyloid levels, accumulating data suggests that this increases the risk of cognitive decline over the next 15 years—particularly when combined with markers of neurodegeneration such as decreased hippocampal volume. Still, Sperling said, “I see that as a glass half full—we’ve got 15 years to intervene.”
Committing something to memory requires activation of a brain region called the medial temporal lobe, where tau accumulates in AD. It also requires disabling the so-called default mode network (DMN), a brain circuit active when the brain is not engaged in a particular task. Amyloid accumulation disrupts the DMN, and disruptions also emerge in other networks and the specificity with which they signal.
Tau levels are associated with cognitive decline.
It’s the combination of amyloid and tau that is important for cognitive decline. Because tau—though not amyloid—correlates clearly with cognitive decline, tau PET imaging, which emerged just a couple years ago, has the most promise as a neurodegenerative marker for clinical trials, Sperling said. Ultimately, trials should move toward primary prevention—identifying drugs that block disease onset before clinical symptoms emerge. The field also needs biomarkers that show a person’s response to therapy.
Circuitry Dysfunction in Alzheimer’s Disease Mouse Models
A lot is known about clinical symptoms, pathology, and molecular mechanisms involved in Alzheimer’s disease, but there is a big gap in understanding how neuronal circuits are affected, said Arthur Konnerthof the Technical University of Munich.
About ten years ago, Konnerth’s lab developed a method for measuring neuronal function at the single cell level in living mice using fluorescent calcium indicators. They used it to investigate neurons surrounding amyloid beta plaques in mice lacking functional amyloid precursor protein (APP), an Alzheimer’s disease model. They hypothesized that these neurons would show decreased activity, but to their surprise, they were hyperactive, while further-away cells were silent. The error signal sent by these hyperactive cells probably disturbs the circuit significantly, Konnerth said.
His team also explored the function of long-range circuits in Alzheimer’s disease model mice. They studied slow wave oscillations, a form of activity that is essential for slow wave sleep and for memory consolidation. These waves travels through the cortex and into the hippocampus in a coherent fashion. In Alzheimer’s disease mice, the coherence of this circuitry is highly disrupted. Enhancing inhibitory (GABAergic) neuron activity reversed the deficit.
Alzheimer’s disease model mice showed improved learning after restoration of slow wave activity.
Tweaking GABAergic activity in normal mice also affected this circuitry, pointing to a synaptic effect. Returning the circuitry to normal also improved a learning task, the Morris water maze, and individual animals’ behavioral performance could be predicted by the coherence of this slow wave oscillation. An fMRI study in humans conducted by another lab showed also showed a disruption in slow wave oscillation. Targeting the shift in excitation-inhibition that underlies slow wave disruption may ameliorate cognitive deficits in the disease, Konnerth said.
Hot Topics in Neuroregeneration
In three short talks, early career researchers described imaging, bioinformatics and candidate gene analyses for probing neurodegenerative diseases.
Johanna Jackson from Eli Lilly used two-photon imaging in two mouse models of Alzheimer’s disease to study how disease progression affects synapses. She and her colleagues tracked axonal boutons and dendritic spines—the presynaptic and postsynaptic points of contact—over time in the same brain region. In the J20 mouse, which develops amyloid plaques, dendritic spine number remained constant, but axonal boutons were lost and the turnover rate of both spines and boutons increased as amyloidopathy progressed. The Tg4510s mouse, which develops tauopathy, showed a different pattern: both spines and boutons were lost, and neurites sickened then disappeared over time. Switching off the transgene in these mice could partially prevent or delay these deficits.
Milo Robert Smith of the Icahn School of Medicine at Mt. Sinai used bioinformatics to probe plasticity mechanisms in neurodegenerative diseases and to identify common disease pathways and potential therapeutic drugs. First, his team conducted microarray experiments to capture gene expression signatures of plasticity in mice. They then matched these signatures to transcriptomics signatures of 436 diseases taken from publicly available databases. The 100-plus illnesses showing a significant association were enriched for neurodegenerative diseases, and inflammatory genes appeared highly implicated. Finally, the researchers matched disease transcriptional signatures to transcriptional signatures of drugs measured in cell lines, also from publicly available databases. Using this approach, they identified drug candidates for resting plasticity in Huntington’s disease.
A strategy for using integrative bioinformatics to identify drugs that target common mechanisms in neurodegenerative disease.
Human motor neuron axons can extend a meter in length, but dysfunction in trafficking such a distance underlies a neurodegenerative disease called hereditary spastic paraplegia (HSP), in which corticospinal motor neurons progressively degenerate. Eliška Zlámalová of the University of Cambridge is identifying candidate genes involved in long axon transport and HSP pathology. Three genes associated with HSP—reticulon, REEP1, and REEP2—produce proteins that localize to smooth endoplasmic reticulum (ER) in axons. When Zlámalová disabled all three in Dropsophila, ER fragmented in the middle of the axon and degenerated distally. To look for additional candidate genes, Zlámalová developed fluorescent markers for two other proteins, knocked own their genes in triple-mutant flies using RNA interference, and imaged ER morphology. She found a trend toward further ER fragmentation; a higher number of experiments may yield more conclusive results.
Further Readings
Reisa Sperling
Jack CR Jr, Bennett DA, Blennow K, Carrillo MC, Feldman HH, Frisoni GB, Hampel H, Jagust WJ, Johnson KA, Knopman DS, Petersen RC, Scheltens P, Sperling RA, Dubois B.
Science. 2014 Jan 31;343(6170):506-511. doi: 10.1126/science.1247363.
Panel Discussion: The Future of Research and Therapies in Neuroregeneration and Restoration
Speakers
Michael J. O’Neill, Moderator Eli Lilly and Company
Ana Maria Cuervo, Panelist Albert Einstein College of Medicine
Mark P. Mattson, Panelist National Institute of Aging
Clive Svendsen, Panelist Cedars-Sinai Medical Center
Jeffrey Macklis, Panelist Harvard University
Panel Discussion The Future of Research & Therapies in Neuroregeneration & Restoration
The panelists began by summarizing what they consider the most exciting dimension in the field of regeneration. Jeffery Macklis said that since graduate school, he had puzzled over the fact that only certain cell types were vulnerable and selectively damaged in different neurodegenerative diseases. “I find that the most exciting question,” he said. “Until we get to neuron subtype specificity and the circuits involved, we could be looking at a lot of unrelated stuff.”
Ana Maria Cuervo notes that neurodegenerative diseases primarily occur in the elder population, yet researchers still don’t know enough about the physiology of aging to determine which dimensions of the disease are due to aging and which are not.
Mark P. Mattson agreed, noting that in Alzheimer’s disease, events upstream of amyloid including generic age-related events such as increased oxidative stress, can affect the disease. “We need to understand those if we want to intervene earlier,” he said. He also wondered whether mechanisms being targeted by drug development could also be activated by exercise or energy restriction. A related approach might be to induce mild intermittent bioenergetic stress on cell pharmacology.
“The thing that keeps me up at night in this field is biomarkers,” said Clive Svendsen. Molecules that change as the disease progresses are not necessarily causative; indeed, some of the stress responses observed in Alzheimer’s disease might be neuroprotective, and that holds for Huntigton’s disease, too, he explained.
An audience member raised the question of sex differences in neurodegenerative disease, noting that even when boys and girls reach the same cognitive milestones, they often arrive there through different routes. In response, Mattson described a study conducted by his group that compared responses to different diets in male versus female mice. At 40% calorie restriction, females shut down their estrus cycle, increased their physical activity, and lost most of their body fat. Males under the same circumstances remained fertile, and their activity levels did not change. That could be because from an evolutionary perspective, females would ostensibly want to avoid having babies when there is no food around, because they lack the energy to care for them, while males might want to inseminate as widely as possible before they starve to death.
Reisa Sperling noted that women respond more adversely to a smaller amount of amyloid beta. “Something about being female means that you are more vulnerable,” she noted. An audience member noted that although men have a higher risk of Parkinson’s disease, females deteriorate faster once diagnosed. Svendsen noted that these observations speak to broader issues in personalizing treatments for neurodegenerative diseases. Sporadic Alzheimer’s disease likely consists of more than one disease, for example. “We’re trying to subdivide ALS into 10 types,” he said.
Panel Discussion
Open Questions
How do hypertrophic astrocytes help require damaged neuronal circuits?
What is the best way of clinically testing the amyloid beta hypothesis?
Can the signaling mechanism linking neuronal activity at the synapse and gene transcription in the nucleus be therapeutically targeted?
How should Parkinson’s disease therapeutic efforts account for homeostatic plasticity in stratal neurons?
Why do different inflammatory responses have different effects on CNS regeneration? [Giger]
How can growth cone machinery be targeted to promote regeneration?
Can fasting and exercise mitigate against dementia and neurodegenerative damage in diseases like Alzheimer’s and Parkinson’s?
How do pathogenic proteins cause the breakdown of chaperone-mediated autophagy, and how does such authophagy contribute to the clearance of pathogenic proteins?
Will improvements in mitochondrial function obtained by targeting Parkin, PARIS or related proteins provide therapeutic benefits in Parkinson’s disease?
How does glial cell dysfunction cause neurological disease and can it be therapeutically targeted? [Goldman]
Can a cell therapy consisting of GDNF-releasing astrocytes stave off paralysis in ALS?
Are there neurodegenerative diseases besides ALS in which genes are maladaptively downregulated in astrocytes?
Will drugs that modulate NMDA activity prove beneficial for Alzheimer’s disease?
How well can organoids reflect the pathology of neurodegenerative diseases?
Can promoting reprogramming strategies that turn non-neuronal cells into neurons be used therapeutically?
Can memory be improved with the help of molecular strategies to rejuvenate hippocampal circuitry that degenerates with age?
Will candidates identified through integrative bioinformatics yield drugs that target common mechanisms in neurodegenerative disease?
How to determine the optimal window for efficacy of different prospective Alzheimer’s disease therapies?
Will reversing the disintegration of slow wave oscillations ameliorate cognitive impairment in Alzheimer’s disease?
The enterprise of drug development is a crucial lifeline for patients and their families. Those who need new and better treatment options depend on researchers to deliver safe and effective therapies as quickly as possible, meaning experimental drugs must first be tested on human volunteers before they can be approved for widespread use.
Since the mid-twentieth century, the randomized controlled trial (RCT) has been considered the gold-standard in research design because of its ability to overcome bias and yield high-quality evidence. But it comes at a steep cost: The average new drug requires six to eight years of human testing and $100 million to fund the clinical trial phase alone. Moreover, conducting an RCT is not always feasible or moral, such as during a pandemic or in the case of a very rare disease.
In such cases, alternative trial designs may produce faster and cheaper results, but in doing so, they must not compromise appropriate levels of standards of safety and efficacy, say regulators, patients, and insurers. While more rapid development is critical to save lives, difficult questions remain about how to tread this delicate balance.
On June 21 – 22, 2017, the Academy convened a colloquium at which academic and pharmaceutical researchers, federal regulators, bioethicists, executives, patient advocates, and lawyers met to discuss the relevance of the randomized controlled trial as the default model for human subject research. Talks focused on the history of the RCT, the ethics and use of alternative trial designs, the risks of foregoing traditional tools, the role of patient advocacy, lessons learned from a recent case study, and the importance of innovation in reforming a flawed system.
With the success of emerging interventions like genomic therapy and immunotherapy, a cultural conversation has opened up around issues such as determining how clinical trials should be designed in this new era, who may participate in research, and when promising therapies should reach the market. Formulating answers to these urgent questions could benefit millions of patients and reshape the future of medicine.
Speakers
Alison Bateman-House, PhD, MPH, MA NYU School of Medicine
Luciana Lopes Borio, MD U.S. Food & Drug Administration
Timothy Caulfield, LLM, FRSC, FCAHS University of Alberta
Anne Cropp, PharmD Early Access Care, LLC
George D. Demetri, MD Dana-Farber Cancer Institute
Rebecca Susan Dresser, JD Washington University in St. Louis
Susan S. Ellenberg, PhD University of Pennsylvania
Howard Fingert, MD, FACP Takeda Pharmaceuticals
Pat Furlong Parent Project Muscular Dystrophy
Barry J. Gertz, MD, PhD Clarus Ventures
Edward M. Kaye, MD Sarepta Therapeutics
Nancy M.P. King, JD Wake Forest School of Medicine
Clifton Leaf Fortune
Holly Fernandez Lynch, JD, BE The Petrie-Flom Center for Health Law Policy, Biotechnology and Bioethics at Harvard Law School
Susan E. Lederer, PhD University of Wisconsin School of Medicine and Public Health
Andrew McFayden The Isaac Foundation
Jane Perlmutter, PhD Gemini Group
Vinay Prasad, MD, MPH Oregon Health and Science University
Amrit Ray, MD Johnson & Johnson
Jane Reese-Coulbourne, MS, ChE MK&A
Christopher Robertson, PhD, JD University of Arizona
Matthew D. Rotelli, PhD Eli Lilly and Company
Eric H. Rubin, MD Merck & Co., Inc.
David Scheer Scheer & Company, Inc.
J. Russell Teagarden NYU School of Medicine Working Group on Compassionate Use & Pre-Approval Access
John (L.P.) Thompson, PhD Columbia University
Meg Tirrell CNBC
Andrea B. Troxel, ScD NYU School of Medicine
Ellis Frank Unger, MD U.S. Food & Drug Administration
Steve Usdin BioCentury
Joanne Waldstreicher, MD Johnson & Johnson
Jeffrey S. Weber, MD, PhD NYU Langone Medical Center
Charles Weijer, MD, PhD Western University
Robert Walker, MD U.S. Department of Health and Human Services
Sponsors
This symposium was made possible with support from
Presented by
Meeting Reports
History and Contribution of Randomized Controlled Trials to Public Health
Speakers
Susan S. Ellenberg, Panelist University of Pennsylvania
Howard Fingert, Panelist Takeda Pharmaceuticals
Susan E. Lederer, Panelist University of Wisconsin School of Medicine and Public Health
Jane Perlmutter, Panelist Gemini Group
Arthur Caplan NYU School of Medicine
Panel Discussion History and Contribution of Randomized Controlled Trials to Public Health
Highlights
American laws regarding drug testing transformed in the 1960s in response to crisis.
New epidemics and targeted genomic therapy are prompting re-evaluation of the RCT.
Industry sponsors have a responsibility to uphold data quality.
A tension may exist between statistical endpoints and patient experiences.
History lessons
The opening panel set the stage for the role RCTs have played in the history of medical research. Susan Lederer, a professor of medical history and bioethics at the University of Wisconsin, described how clinical trials first came to be. In the 1760s, James Lind was a ship surgeon in the British navy faced with a rash of scurvy cases.
In a bid to stop the outbreak, he divided twelve sailors into groups of two, rotating each through different sets of treatments. The groups tried sea water, sulfuric acid, vinegar, cider, a tamarind paste, and oranges and lemons. When that last treatment proved effective, Lind realized he had hit upon a cure.
But officially randomizing treatment into a control arm and a trial arm didn’t gain traction until the mid-twentieth century, when World War II prompted a massive influx of federal dollars for research, and the pharmaceutical industry began to transform American medicine. In the early 1960s, after many pregnant women took the drug thalidomide, which caused fetal deaths and birth defects, Congress established laws calling for “adequate and well-controlled” studies that demonstrated efficacy as well as safety before drugs could be approved.
By the 1970s and 80s, the RCT had become the gold standard, said Arthur Caplan, a bioethicist at the NYU School of Medicine. But just two decades later, criticism emerged during the HIV epidemic, when many patients pushed back on ethical grounds against being randomized, contending that scientific advancement should not come at the cost of their own lives. While some patient groups praised the RCT model, some observers, like prominent physician Marcia Angell, called into question researchers’ “slavish adherence” to the RCT at the expense of compassion for individual sufferers.
In the current era of epidemics like Ebola and Zika, and the increasing prevalence of targeted genomic therapies, the relevance of the standard RCT has been called into question with renewed urgency. Some situations, Caplan said, don’t permit the time or expense of a standard RCT. That’s a point which has raised substantial debate, but some argue that patients may be too sick to participate, the need for treatment may be immediate, the number of sufferers too small, or the ability to maintain oversight too unrealistic.
Jane Perlmutter, a patient advocate, offered additional concerns about RCTs, including limitations on generalizability if trial subjects don’t comply with the protocol, and if eligibility requirements narrow the scope of the testing population.
“This gold standard is not so terrific,” she declared. “We need to innovate.”
Patients also don’t like to be guinea pigs, she noted, suggesting one “baby step,” towards innovation could be allowing patients to choose to join the experiment or control group, rather than be blinded and randomized. Still, randomizing some patients in is important to preventing bias and leading to generalizable findings. In such a design, researchers must carefully assess the data to ensure that the randomized subjects and the self-chosen subjects show no misleading discrepancies. As long as their results align, this type of study can be both efficient and effective.
At the same time, Howard Fingert, senior medical director at Takeda Pharmaceuticals, said that the management of big data is a major responsibility and opportunity for industry sponsors no matter the trial design. Mechanisms for data sharing can improve understanding in trials that are single-armed, propensity-matched (meaning those driven by a statistical score that estimates a treatment’s effectiveness), or underpowered (meaning those statistically unlikely to distinguish a treatment effect from pure luck due to a low sample size).
And upholding data that is reflective of reality is crucial, he said. For example, if a primary endpoint in a study fails, investigators may look for a positive secondary endpoint that wasn’t originally in the protocol—a practice he called “ubiquitous but not legitimate.”
Caplan asked whether fear of adverse outcomes is hindering innovation, citing the 1999 death of an 18-year-old in a clinical trial for gene therapy, which proved a major setback for the entire burgeoning field. Susan Ellenberg, a professor of biostatistics at the University of Pennsylvania, noted that risk aversion is even more common now, as social media reinforces people’s negative beliefs about the prevalence of dire medical events, like vaccine toxicity. But 37 states have passed right-to-try laws, Perlmutter pointed out, which permit terminally ill patients to volunteer for experimental therapies.
Finally, the panelists discussed how the very notion of efficacy has evolved. Decades ago, patients were asked if they were feeling better after an intervention, but now the focus is on objective endpoints—sometimes to a fault, according to Perlmutter. She questioned whether an outcome such as a shrinking cancer tumor, for example, is truly meaningful if the patient’s quality of life remains unaffected. Caplan reminded the group that in dialysis programs for end-stage renal disease in the 1970s, one measure of success was whether patients could return to work. But Ellenberg added that patient improvement and high-quality data are not mutually exclusive.
“Looking for objectivity doesn’t exclude those endpoints,” she said.
Luciana Lopes Borio, Panelist U.S. Food and Drug Administration
Barry J. Gertz, Panelist Clarus Ventures
Andrea Troxel, Panelist NYU School of Medicine
Charles Weijer, Moderator Western University
Panel Discussion Beyond RCTs — Assessing the Need for Alternatives
Highlights
Choosing between a standard RCT and a non-RCT alternative can be a false dichotomy.
FDA states that all patients deserve the same evidentiary and regulatory standard.
Tension exists between targeting therapies to the right patient population and understanding drug safety and efficacy.
Innovation without compromise
Moderator Charles Weijer, a bioethicist at Western University, kicked off the discussion by asking panelists to offer up important lessons about clinical trials from the past. Barry Gertz, a partner at Clarus, pointed to randomization as the key to reducing bias, and a reason why the RCT ought to remain the default design for testing new agents. Despite its heavy costs, he argued, the overall societal burden would be even higher without it, citing the example of a new device tested for severe hypertension. It produced what seemed at first to be miraculous results—until a subsequent RCT proved it no better than a sham procedure.
“If you don’t test with adequate rigor,” he warned, “society will pay a very substantial price if it’s not as effective as it’s billed to be.”
Luciana Borio, acting chief scientist at the FDA, agreed that classic RCTs still deserve a primary place in the medical ecosystem.
“Nobody has said, ‘I regret doing an RCT,’” she said. “History has played out the other way around; ‘we didn’t know and had to live with the consequences.’”
Even in cases of public health emergencies like Ebola, when some scientists deem RCTs impractical, she maintained that such situations especially demand informative studies.
“We have to be better prepared for the next epidemic,” she added. “We can’t say it’s too hard to do it.”
Weijer commented on the importance of avoiding a false dichotomy between RCTs and alternatives that are still capable of incorporating randomization into their designs. For example, Borio mentioned the ring study carried out during the Ebola crisis, in which groups of people known to be in contact with a patient—those forming a so-called “ring” around the infected person—were randomized to receive a new vaccine either immediately or after a three-week delay.
Andrea Troxel, a professor of population health and biostatistics at NYU, agreed that randomization in some capacity is necessary for the generation of high-quality knowledge, even if a standard RCT “is not always the answer.”
Weijer then raised the complex issue of whether rare diseases necessitate a lower standard of evidence for drug approval, given the lack of patients available for clinical trials. While Troxel said that “sufficient evidence” would not be possible to attain in a standard RCT, others disagreed. Gertz pointed to the approval of a drug for spinal muscle atrophy, the most common genetic cause of early demise in infants. An RCT was carried out on just 81 patients using a sham placebo administered to the spinal fluid, with results showing that the drug yielded profound increases in motor activity.
“It benefited a very small number, but even in that rare disease, the RCT provided some real evidence of benefit and is now available,” he said.
Regarding common diseases, the panelists disagreed on whether a social imperative to accelerate development justifies a lower evidentiary standard. Borio cautioned against the temptation to take short cuts, and said that all patients deserve the same high regulatory standard, while Troxel similarly warned of the “unintended consequences” of rushing new therapies out to desperate patients.
But at that moment, patient advocate Jane Perlmutter spoke up from the audience, declaring that patients with terminal illnesses want to take risks. “I don’t think we need to lower the bar, but we need to have innovative approaches to deal with deadly diseases,” she said. Gertz suggested that one potential solution would be for the FDA to grant a drug provisional approval using an intermediate or surrogate endpoint, with later testing to confirm the findings.
But if those findings failed to hold up, withdrawing such a drug from the market would be difficult, due to a backlash from patients still demanding access to the drug. He said this scenario has happened once in oncology and “it wasn’t pretty.”
In the unique case of biologically targeted therapy, Weijer posed the intriguing question as to whether the science has evolved to such point that an RCT is not needed to evaluate a drug’s effectiveness. Gertz acknowledged that studies with driving mutations in oncology are typically single arm, but that a control group is implicit in the standard of care response rates. He also maintained that a randomized trial would be needed eventually to determine safety as well as efficacy.
All the panelists agreed that helping the diverse range of patients who exist in the real world is crucial, and requires testing beyond narrow subsets who don’t reflect the larger population. More recently, pragmatic trials—which more realistically mimic day-to-day practice settings—are gaining traction, said Troxel.
Such trials aim to clarify how effective a recommended therapy might be, as opposed to explanatory trials, which aim to elucidate mechanisms of action in a new agent. Yet, “those two goals are not necessarily in conflict,” she said. A trial might be explanatory at first, with small numbers and a strict inclusion criteria, then broadened to test the therapy on a wider group.
Borio lamented that researchers don’t learn from most patient encounters because of a lack of access to studies. Today, the practice of medicine often takes place separately from the world of research, so when sick patients visit the doctor, their cases are not analyzed to improve the effectiveness of treatments for others. And those who do participate in studies often fail to represent important demographic subgroups.
Currently, the typical participant is a young, white male who lives near a metropolitan area. Borio would like studies to systematically include patients who are not usually included, like those in rural areas, minorities, babies, and pregnant women. Her dream is for every person in the medical system to be able to enroll in a clinical trial.
“There’s no national trial infrastructure in this country, like highways,” she said. “But we need it so we can make the most use of all the knowledge.”
Doing so, however, she acknowledged would require a major shift in how doctors are educated about clinical trials and how patients view the riskiness of participating in research. Many patients decline to participate because they view research as inherently riskier than regular medicine, which is not necessarily true.
Expert Opinion Pharmacotherapy 16(9):1275-9, Jun 2015.
Finding the Right Balance in Learning about Therapies
Speakers
Robert Califf Duke University
Audience Q&A with Robert Califf
Highlights
There are clear benefits to combining research with clinical practice.
RCTs and alternative trials could be combined and run continuously.
The current clinical trial system is deeply flawed and too expensive.
Data sharing among health care systems will speed evaluation and development.
Asking the right questions
The future of human experimentation is at a crossroads. Sick and dying patients need treatment options as quickly as possible, but rushing out new therapies will not necessarily benefit them.
The real issue, said keynote speaker Robert Califf, is how to accelerate drug development but also “get it right.” The current clinical trial enterprise has “gone awry,” he said, calling it unnecessarily expensive.
Califf, a cardiologist and former commissioner of the FDA from 2016 to 2017, charged the system fails patients by not asking all the important questions. “It’s not that clinical trials are too hard, it’s that there are questions not even being asked because it’s so costly,” he said.
A schism has developed in medicine, between those who think human experimentation should be conducted within the context of daily practice and those who feel it should remain separate from it. In Califf’s view, human experiments benefit when combined with insights of clinicians, but the layers of oversight and the risk of punitive action dissuades doctors from participating in research. He criticized what he called common myths about RCTs: that they must exclude patients who represent the likeliest use of therapies, and that clinical trials are risky compared with routine care.
“There’s no reason you can’t enroll real-world clinical patients in a trial,” he said.
He also dismissed the notion that doctors regularly review evidence and make the best decisions for their patients—simply because statistically valid evidence often doesn’t exist in medicine. In fact, he said, many practice recommendations are not based on high-quality evidence, such as the CDC’s recent guidelines for prescribing opioids. Unlike the rigorous approach codified in research studies, much of medical practice is rooted in observational and historical data, leaving doctors with a limited set of tools.
His solution is to run RCTs in combination with alternatives, such as pragmatic trials, to reduce the cost and enable better generalizability from the start. In the early phases of therapeutic development, he suggested randomizing from the first patient — “the quickest way to get treatment to patients even with rare diseases.”
Then, in later phases, every interaction with patients would be logged in a digital database. He urged a national paradigm shift toward the sharing of such data across health care networks. Such an effort would be in keeping with the drive to create incentives for health systems to work together that was written into the 21st Century Cures Act, which was signed into law in December 2016, and the user fee reauthorization bill currently working its way through Congress.
He envisions moving away from inefficient one-off studies, done in a parallel track to clinical practice with passive surveillance, to active surveillance, for instance by collecting information on millions of patients in a central database embedded in the health care system, with broad data-sharing among providers. He discussed his involvement in PCORnet, the National Patient-Centered Clinical Research Network, which collects data across hospitals, doctor’s offices, and community clinics in an attempt to help guide healthcare decisions.
He also urged patients to push academic health systems to stop hoarding data, positing that if the medical world shared the business world’s mentality of persistent data collection, progress would accelerate.
“When you do a Google search, you’re participating in up to ten randomized trials,” he noted.
The bottom line, he concluded, is not to abandon RCTs, but to maintain continuous and constant observation as health care is delivered. Just as Google analyzes its data nonstop to improve user experience and anticipate search queries, medicine ought to catalogue and interpret its abundance of real-world data to bring to light the best treatment options for patients.
Weighing the Risks of Randomized Controlled Trials and Alternatives
Speakers
Holly Fernandez Lynch, Panelist Petrie-Flom Center for Health Law Policy, Biotechnology and Bioethics at Harvard Law School
Amrit Ray, Panelist Johnson & Johnson
Matthew D. Rotelli, Panelist Eli Lilly and Company
Robert Walker, Panelist U.S. Dept. of Health and Human Services
Steve Usdin, Moderator BioCentury
Panel Discussion Weighing the Risks of RCTs and Alternatives
Highlights
Controversy surrounds the use of RCTs during public health emergencies.
Platform trials can reduce costs and increase efficiency.
Vulnerable populations need adequate access to clinical trials.
Increasing research participation is key to obtaining comprehensive data.
Maintaining equipoise
Genuine uncertainty about the comparative effectiveness of different interventions is the ethical foundation for randomized clinical testing, a concept known as equipoise. Moderator Steve Usdin, Washington editor of BioCentury, opened the discussion by asking panelists to weigh in on the challenges of striking equipoise during therapeutic development. If a given intervention is known to work, the researcher cannot in good conscience withhold it from test subjects, said Harvard bioethicist Holly Fernandez Lynch.
Robert Walker, acting chief medical officer of the Biomedical Advanced Research and Development Authority (BARDA) within the U.S. Department of Health and Human Services, discussed the challenges of maintaining equipoise during the Ebola crisis.
“There was a sense that you can’t conduct a clinical trial in the midst of an emergency response, but we saw that it was in fact feasible,” he said, citing three randomized vaccines trials carried out in Liberia, New Guinea, and Sierra Leone.
As to the private groups that granted some patients emergency access to treatment during the public health emergency—without a trial to gauge efficacy—Walker said, “It’s not even information…We really didn’t learn.”
Usdin asked the panelists to describe when to use RCTs versus alternatives. Amrit Ray, chief medical officer at Johnson & Johnson, posed a solution that would retain the benefits of randomization but reduce the costs and facilitate data sharing: integrated platform trials. In the current system, five companies might test five different drugs for the same disease in isolation. Instead, Ray proposed, what if those companies collaborated on one joint trial with a common control arm? This would lessen the burden of duplicate trials and patient recruitment, and allow for faster data collection to evaluate drugs, as with the innovative I SPY-2 trials in breast cancer.
Then Matthew Rotelli, a director at Eli Lilly, raised the challenge of how to broaden clinical trials to include vulnerable populations like children, “because if you don’t study them,” he said, “you have no way to guide their treatment.” Walker responded that BARDA has a legislative mandate to study all populations, and that special additional oversight for kids would only make the process more onerous. He stated that existing measures, including institutional review board review, are already responsible for ensuring proper informed consent.
Regarding novel trial designs, Usdin worried that even if the data persuades regulators to approve a drug, insurers still might not pay without the legitimacy conferred by a standard RCT. Ray responded that the comparison design of platform trials could potentially mitigate that risk.
Another new paradigm could emerge to meet serious unmet needs—allowing patients to risk taking a promising experimental drug faster in exchange for the sponsor collecting comprehensive data post-market. While Fernandez called this an “ideal world,” she was somberly realistic about its prospects. New laws would have to be passed, and sponsors would need to be held accountable.
Rotelli envisioned a future in which clinical trials never end. As new drugs come out, they are added to ongoing randomized platform trials for further study against known drugs. Less effective ones eventually get dropped, while electronic medical records facilitate the data collection. But obtaining and sharing that data would require a “dramatic shakeup of systems,” Fernandez said.
Right now, research participation requires robust informed consent, with autonomy prized as the highest value. It operates in a separate layer from clinical care, protected by institutional review boards that regularly review protocols to protect participants from exploitation.
An opposite model, in which data collection is routine, would require most patients to participate by default, rather than choosing to opt in.
“I don’t know that I would go to that end of the spectrum,” she said. “It’s so different from how we’ve done research, given concerns about historical abuses.”
Expecting compulsory participation makes many observers in the medical community uneasy. The twentieth century, after all, is filled with brazen examples of vulnerable subjects who were harmed or killed for the sake of science, including concentration camp victims and the cohort of African-American men infected with syphilis who, unbeknownst to them, were denied penicillin by Tuskegee researchers. Such infamous cases led to establishment of a set of morals and rules for human research participation via the 1947 Nuremberg Code and the 1979 Belmont Report, establishing the ethical pillars of autonomy and informed consent.
Unless such historical abuses fade in the collective consciousness, any future reforms that dial back the protection of individuals are unlikely to be popular.
Ethics and Patient Advocacy in Clinical Trial Design
Speakers
Rebecca Susan Dresser, Panelist Washington University in St. Louis
Andrew McFadyen, Panelist The Isaac Foundation
Jane Reese-Coulbourne, Panelist MK&A
J. Russell Teagarden, Panelist NYU School of Medicine Working Group on Compassionate Use & Pre-Approval Access
Alison Bateman-House, Moderator NYU School of Medicine
Panel Discussion Ethics and Patient Advocacy in Clinical Trial Design
Highlights
A cultural clash exists between patients and researchers.
Many specialists agree that clinical design could be improved by involving patient experts early on.
Early access programs allow patients to try experimental therapies outside of clinical trials.
Expanding inclusion criteria would allow more people to participate in research.
Balancing acts
When it comes to the policies and guidelines that govern drug development, patients and researchers often find themselves at odds, clashing over aspects such as trial design, compliance protocols, and early access. Differing motivations lie at the heart of the conflict, suggested moderator Alison Bateman-House, a bioethicist at NYU. Researchers want to help push science forward, while patients want access to therapies that will help them and their loved ones.
“When you’re a patient or a parent, [those with] the option of being in a trial think, ‘What would benefit me most?’” said Rebecca Susan Dresser, a cancer survivor and bioethicist at Washington University in St. Louis. “Altruism is low on the list.”
Many of those who can’t participate in trials struggle to persuade sponsors to let them try experimental therapies under the FDA’s program of expanded access, also known as compassionate use. Companies may be reluctant to participate in compassionate use in part because giving patients a drug outside of a trial means a lost opportunity to gain valuable data on safety and efficacy.
Advocacy groups, such as Andrew McFadyen’s Isaac Foundation, fight for access despite these concerns, because offering patients with rare diseases otherwise unavailable treatments can mean the difference between life and death.
“While RCTs are good at getting approval of drugs, it’s a hindrance in getting them to our children,” he said.
Patients and researchers should work together from the start of designing a trial so their goals can coincide, the panelists all suggested. Too often, Bateman-House said, patients are silent partners, which can translate into a protocol that’s too lengthy, intensive, or inconvenient. For example, Dresser rejected an offer to join a cancer trial for her advanced illness because its timeline would have meant a delay in starting treatment.
Jane Reese-Coulbourne, a former cancer trial participant and now consultant, stressed the importance of companies bringing in expert patients for feedback. As a patient advisor, she helped Genentech, a major biotech company responsible for several dozen pioneering drugs, understand why its recruitment for one particular trial was so low: the protocol required enduring four painful bone marrow aspirations, a procedure which extracts fluid from the marrow.
But when collaborating, patient advocacy groups can sometimes find themselves toeing a tricky ethical line between accepting funding from pharmaceutical companies and maintaining their organizational independence.
“Often pharma does bring us in for advice,” McFadyen said, “but sometimes the expectation there is that we’re going to be the people out there making sure [the drug] gets reimbursed.”
Some advocacy groups, he said, will accept payment in exchange for not asking tough questions about access. J. Russell Teagarden, a pharmacist, executive and educator, acknowledged that there are advocacy groups vulnerable to coercion.
“But on the other hand, there are some groups so sophisticated that maybe the companies are vulnerable,” he said, to laughs.
Another source of conflict between companies and patients is rhetoric. Too often, companies employ hyperbolic language like “breakthrough” to attract investors, while desperate patients line up for trials that haven’t in actuality even begun.
Bateman-House said that the lack of scientific literacy in the general population, who are prone to believing the science holds all the answers, is a major source of confusion. In fact the vast majority of drugs fail in the lab long before the point of human trials. Indeed, only one in a thousand compounds graduates to clinical testing, and of those, only about 10 percent eventually cross the finish line.
Issues about trial demographics came to the fore during a vibrant Q&A. One audience member expressed concern over how to expand clinical trials to underrepresented groups, like pediatric cancer patients. McFadyen suggested that is possible if parents push for it. Another spoke of disappointment over the fact that only 10 percent of patients qualify for trials. Several panelists responded that legislation is underway in the Senate to expand inclusion criteria so more people can participate in research.
Expert Opinion Pharmacotherapy 16(9):1275-9, Jun 2015.
Modern Trends in Clinical Drug Development
Speakers
Janet Woodcock U.S. Food and Drug Administration
Audience Q&A with Janet Woodcock
Highlights
Clinical trials are a prohibitively expensive element of drug development.
Trial designs, no matter how novel, will only be as good as the knowledge underlying them.
Randomization remains an important tool but is not always necessary in novel designs.
The system requires reform to incentivize continuous, collaborative platform trials.
Designing alternatives
The clinical trial system in the United States is broken because it isn’t “fit for purpose,” argued Janet Woodcock, director of the Center for Drug Evaluation and Research at the FDA. Because trials are so expensive and time-consuming, many questions remain unanswered after a drug is approved, leading to health care practices that too often lack high-quality evidence.
She discussed the wasteful efforts when a sponsor sets up a trial, tests an intervention, and then walks away because either the trial fails or the drug reaches the market. Instead, the future ought to bring more continuous, ongoing platform trials that can answer multiple questions at once, with data shared among health care networks.
“The goal,” she said, “is not to test a specific therapy, but to bring about continuous improvement in disease outcomes.”
In the current era, rapidly evolving science is driving novel research designs. Molecularly targeted therapies are on the rise, along with drugs that are “disease agnostic,” such as those that might target a specific biomarker appearing across tumor types, for example. With rare, life-threatening diseases that lack treatment options, she suggested it may in fact be adequate to test a targeted therapy, which is expected to show a large treatment effect, in a single-arm trial with an extended phase one cohort.
“I’m going to say something heretical, but oncology has been doing this, and it’s perfectly reasonable in my mind under these circumstances,” she said.
While a very useful tool, randomization in her mind is not an imperative. However, “it’s foolish not to use it if at all possible,” she added, such as if the disease outcomes are very variable or researchers don’t expect to get a homerun treatment effect.
But as more development programs are working on very rare and orphan diseases, the FDA is approving drugs based on limited trials that may lack randomization, as with an antidote for methotrexate toxicity devised from the data of 22 patients. Such cases involve a serious unmet medical need, a well-understood disease, highly plausible biomarkers that can be easily measured in a standardized way, and a drug that yields a large treatment effect.
She cautioned, however, that the design of a trial is only as good as the quality of the knowledge underlying it. Biomarkers may mistakenly drive a development program, for example, if they are not reproducibly measured, accurate, or predictive. Before starting trials in humans, researchers should be confident that a biomarker is “reasonably likely to predict clinical benefit,” she said, suggesting that randomization usually remains the best design in this situation.
Calling for greater efficiency overall, she urged a shift toward collaborative platform trials that integrate research and practice. But implementing changes to the status quo poses a serious challenge.
“In this translational world of continuous improvement in medicine, nobody is charged to do it and that’s the real problem,” she acknowledged. Since there isn’t a key stakeholder, she urged patients to rise up and demand reform.
Lessons from the Eteplirsen Drug Trial for Duchenne Muscular Dystrophy
Speakers
Pat Furlong, Panelist Parent Project Muscular Distrophy
Edward M. Kaye, Panelist Sarepta Therapeutics
Ellis Frank Unger, Panelist U.S. Food and Drug Administration
David Scheer, Panelist Scheer & Company, Inc.
Meg Tirrell, Moderator CNBC
Panel Discussion Lessons from the Eteplirsen Drug Trial for Duchenne Muscular Dystrophy
Highlights
Patients-researcher collaboration could enhance planning of clinical trials.
Surrogate endpoints should comport with clinical gains.
Understanding a disease’s natural history and its biomarkers is crucial to guiding high-quality research.
Limited trials can lead to accelerated approvals, but questions may remain about real-world effectiveness and who will pay for the drug.
Case study
The accelerated FDA approval late last year of the drug Eteplirsen for Duchenne Muscular Dystrophy (a disorder that predominantly manifests in young boys and progresses rapidly) based on controversial data from a 12-patient randomized trial, set off a lively discussion. Sufferers with this rare disease progressively lose muscle function and previously had no treatment options before Eteplirsen came on the market in late 2016, gaining approval even though its effectiveness is still being debated. Moderator Meg Tirrell of CNBC opened by asking the panelists whether the case established any precedents.
Ellis Unger, director of Drug Evaluation-I in the Office of New Drugs at the FDA, offered his concern about the trial’s surrogate endpoint: the drug was approved based on a small increase in the amount of dystrophin, a key protein, found in skeletal muscle. However, whether the increase yields meaningful clinical benefits remains an open question and a flash point for controversy. Unger said he worried that the case will prompt other companies to present similarly limited data and expect to gain FDA approval.
But Pat Furlong, a patient activist and the mother of two boys who died of the disease, argued that the drug did show improvement in the gaits of those who took it, and that desperate patients should not be prevented from taking risks. “It has rocked my world,” she said, speaking of the hope it’s brought to patients who now have the option to try a drug where before none existed.
Edward Kaye, CEO of Sarepta Therapeutics, the drug’s sponsor, contended that small amounts of a biologically active component can work, and said that “the bigger precedent is patient involvement.” Throughout the study, his company worked with patients’ families to understand what quality-of-life outcomes would be most meaningful from a drug, such as the ability to go to the bathroom independently. He also collaborated with other companies to accelerate the search for biomarkers. Their collective pact to publish joint findings represents a notable shift in how research is done.
“It’s not one company against another,” he said, “it’s a number of companies and patient groups against the disease.”
In response to a question about the importance of biomarkers in raising capital for research, David Scheer, an entrepreneur in the life sciences, said that they provide crucial preclinical data.
“Without having some sort of biomarker technology that can facilitate translational medicine, we might be shooting in the blind,” he explained.
The discussion turned heated when Unger described the unusual public comment period during an FDA advisory meeting prior to the drug’s approval. While some of the boys from the trial declared their improvement, Unger said the data showed they were in fact deteriorating. He also described the comment period as “a circus,” because in his view patients and families went over the line, taking too long, and in some instances heckling the committee.
Shortly thereafter, patient advocate Andrew McFadyen approached the microphone and admonished Unger. McFadyen told him to show more respect for families with dying children and to listen to their stories for a year if necessary. “If you can’t do that, you should give your chair up to someone else,” he declared.
While Unger apologized for using the word “circus,” he defended his remarks, recounting the conduct of the session.
“When the deputy director of the Neurology Division told a very personal story of tragedy, he was heckled.” He continued, “we have to draw a line somewhere, and we thought that the time we allotted was reasonable… the catcalls, and the heckling, it was very disheartening.”
Former FDA commissioner Robert Califf stepped up to offer additional insight into the process. “Advisory committees are so named because they do not make the decisions,” Califf said. “Full time government employees are the ones who make the decisions and most people are still confused by that.”
“There was no one in the FDA who thought that the studies were well done,” he added. “I don’t think these decisions would have been so hard otherwise.”
Another audience question addressed the cost of the drug: At a price of $300,000 annually per patient, insurers are balking; they want to see real-life evidence of effectiveness before paying for it. Kaye’s company has started a registry to gather such data, but he said that new therapies in small populations entail expensive drugs because limited numbers of patients receive them.
“So, the cost of developing the drug is transferred to them,” he said. “That is the cost of innovation.”
George D. Demetri, Panelist Dana-Farber Cancer Institute
Anne Cropp, Panelist Early Access Care, LLC
Christopher Robertson, Panelist University of Arizona
John (L.P.) Thompson, Panelist Columbia University
Donald Berry, Moderator MD Anderson Cancer Center
Panel Discussion A Way Forward
Highlights
Platform trials are a key way to merge research and practice.
RCTs are still considered the definitive trial design for reducing bias.
Sharing well-established trial templates for common diseases will eliminate redundant efforts.
Sponsors should make compliance less burdensome for patients.
Refinements or reinvention?
The lively panelists in the afternoon session had no qualms about offering blunt criticism of the status quo. Echoing a theme of the conference, moderator Donald Berry, a statistician at MD Anderson Cancer Center, underscored the need to merge research with practice.
“It’s inevitable,” he said. “We have to figure out how to do it, and platform trials may be the way.”
George Demetri, a medical oncologist at the Dana-Farber Cancer Institute, summed up the situation more derisively: “The clinical trial system is broken,” he said, “and we’re not being honest with the public about what we do and don’t know.” He argued that the benefits of precision medicine and testing for mutations are oversold to patients, particularly by academic institutions.
Christopher Robertson, a law professor at the University of Arizona, raised concerns about bias skewing results, especially in cancer drugs with small effect sizes. Blinding not only patients, but also investigators and statisticians, is crucial to finding legitimate outcomes. Another way to reduce bias is to specify endpoints before the start of a trial to avoid coming up with erroneous probability values, he said.
Anne Cropp, chief scientific officer of Early Access Care, suggested that one way to improve efficiency in the development of new protocols is to make data from the NIH more widely available so that companies working on common diseases like Alzheimer’s and diabetes can use established trial templates, with well-defined endpoints, rather than starting from scratch. She also urged physicians to become more literate in drug testing, citing a Tufts study that revealed a surprising lack of knowledge among doctors regarding the ins and outs of clinical trials.
John Thompson, a professor of biostatistics and neurology at Columbia, cautioned against a premature rejection of double-blind, placebo-controlled RCTs. He worked on just such a trial involving a treatment for ALS, despite being told it was impossible because patients would decline to participate.
“Must RCTs give way?” he asked. “A flexible no, although many people will hear it as a yes, because I envisage considerable fast-moving changes.…It’s a matter of adding to and expanding rather than abandoning the existing techniques.”
A key to the ALS trial’s success, he said, was explaining to patients the importance of its design to gain their trust and cooperation. To help with recruitment, he suggested that disease advocacy groups post the details of ongoing trials on their websites, after networking with investigators, so that patients can find the information and take it to their doctors.
During the audience comment period, Ellis Unger of the FDA offered additional suggestions. He mentioned a “very powerful” trial design that he believes is not used enough: randomized withdrawal, in which responders stop taking a drug and investigators observe what happens. He also urged sponsors to make compliance easier for patients by letting them participate from home, via Skype, when possible, and to limit the number of scans and tests they must undergo.
“The FDA does not need forty thousand blood tests or four X-rays per person to approve a drug,” he said dryly.
Panel Discussion
Further Readings
Journal Articles
Poor Physician and Nurse Engagement Contributes to Low Patient Recruitment Rates
Tufts Center for the Study of Drug Development, Jan 2017.
Nature Reviews Clinical Oncology 9(4):199-207, Nov 2011.
Ethics Panel Wrap-up
What is the Future of Accelerated Development and the Randomized Controlled Trial Standards?
Speakers
Nancy King, Panelist Wake Forest School of Medicine
Vinay Prasad, Panelist Oregon Health and Science University
Eric H. Rubin, Panelist Merck & Co., Inc.
Jeffrey S. Weber, Panelist NYU Langone Medical Center
Timothy Caulfield, Moderator University of Alberta
Panel Discussion Ethics Panel Wrap-up
Highlights
RCTs remain a key method for overcoming bias and threats to validity.
But not every drug requires a large, expensive RCT for initial approval.
Platform trials retain randomization while operating more efficiently.
The system requires reform to incentivize collaboration and transparency.
One tool along the continuum
The final presenters agreed that RCTs are not going away anytime soon, but there are changes in how and when they are being used.
Vinay Prasad, a hematologist-oncologist at Oregon Health and Sciences University, defended the RCT against common criticisms. If such trials don’t reflect real-world populations, he said that is due to strict inclusion criteria, not the design. And if endpoints don’t represent clinical outcomes, the RCT itself is not to blame. That would be “like blaming the Wright brothers for United Airlines,” he quipped.
Eric Rubin, vice president of oncology clinical research at Merck, argued that the title of the conference should not be, “Must RCTs give way?” but rather, “Should RCTs not get in the way?” For example, a single-arm study in a drug with a large effect size can lead to initial approval faster than a standard RCT. Finding such a drug requires high-quality basic research and reproducible preclinical studies, he added.
Jeffrey Weber, deputy director of the Perlmutter Cancer Center at NYU, acknowledged that everyone “worships the god of the randomized, phase three trial,” but he expressed concern over its exploding costs and suggested that modifications in some cases could be appropriate. He proposed using more novel endpoints, such as landmark survival at one and two years, combined with a quality-of-life questionnaire.
“In the immunotherapy era,” he said, “I think we can afford to be more flexible than to do an RCT with a thousand participants and the only endpoint is survival.”
But Prasad was quick with a rebuttal, arguing that progression-free survival is based on an arbitrary line in the sand and is not necessarily correlated to eventual survival.
Rubin agreed with Weber that RCTs are the definitive way to demonstrate benefit, but that at least in oncology, an RCT with overall survival as the endpoint is not required to approve a drug. Rubin suggested that it is possible to deliver promising therapies quickly, without sacrificing randomization, by conducting early phase explanatory trials for initial registration and then a post-market RCT to verify early results.
For example, at Merck he led the development of a melanoma drug that was approved after a single-arm study in patients with advanced illness who were out of options. Afterward, Merck followed up with a randomized trial in less sick patients to compare the new drug against existing alternatives, in which case researchers still retained equipoise. This scenario shows it’s possible to do both—accelerate approval, in this case by three years, and still conduct a confirmatory RCT.
Rubin reiterated an idea that got a lot of play across the conference—the notion that a collaborative platform trials could streamline the process of matching drugs to patients across a spectrum of disease, as was the case in I-SPY2. Such trials benefit patients by letting them get assigned to one arm no matter their cancer.
But Nancy King, a professor of social sciences and health policy at Wake Forest, pointed out that academic institutions and businesses aren’t structured to reward transparency and collaboration over competition.
“You have to be able to turn the battleship,” she remarked.
In a discussion on the exorbitant expense of running trials, Weber said that the regulatory scrutiny has proliferated over the last decade, adding to the cost burden.
“We have monitors that monitor the monitors,” he joked.
Ultimately, even as some areas of drug development move away from the RCT, it remains a fundamental tool along a continuum of designs. One reason it may never vanish is that it can act as a bulwark against the fallibility of human nature.
“Our capacity for hope makes us incredibly susceptible to inferior levels of evidence,” Prasad reflected.
In his opinion, the beauty of randomization is that with a modest effect size, there is no better way to tease apart what works.
Journal of Clinical Epidemiology 66(4):361-366, April 2013.
Open Questions
How can researchers and industry sponsors be incentivized to collaborate on platform trials and sharing data?
How can researchers accelerate drug development without sacrificing the collection of data on efficacy and safety?
How can society increase scientific literacy among the public to encourage participation in research, rather than view it as inherently risky?
How can the medical profession systematically integrate research and clinical practice?
If a drug is granted accelerated approval after a single-arm trial, how can the sponsor be held accountable for collecting post-market data on safety and efficacy?
Will insurers pay for drugs that are approved based on limited or non-randomized trials?
During the next humanitarian emergency, is it feasible and ethical to test interventions with a RCT?
How can costs be better managed to complete a RCT without the prohibitive expenses?
Can decreasing the amount of oversight streamline trials without sacrificing protection for research participants?
Can sponsors and patients work together to design trials at the earliest stages, ensuring that compliance in a protocol is not overly burdensome?
Should a standard RCT remain the default design?
Is choosing between a RCT and an alternative design a false dichotomy?
How can trials better accommodate broad patient populations to yield real-world data and integrate more patients into research?
Who should decide how much risk is appropriate in trying an unproven therapy?
Will big data solve quandaries of speed and the historical limits on the RCT?
Should rare diseases with limited numbers of patients available for trials have a lower evidentiary standard for drug approval?
What can be done to reign in exorbitant drug prices?
Will automation and electronic medical records help motivate doctors to participate in large-scale practical trials?
How can society implement the changes required to modernize the clinical trial enterprise?
Biotechnology and nanotechnology have given rise to a growing number of innovator-driven complex drug products and their copy versions. Biologics exemplify one category of complex drugs, but there also exist non-biological complex drug products (NBCDs), including many nanomedicines such as iron-carbohydrate complexes, several drug carrying liposomes or emulsions, and glatiramoids. These products are difficult to characterize—often the key features for efficacy and safety are not well understood. These factors pose unique challenges for pharmaceutical companies and regulatory agencies when comparing generic complex drugs to their branded counterparts.
On November 9, 2016, representatives from academia, industry, and regulatory agencies convened at the New York Academy of Sciences for the symposium Equivalence of Complex Drug Products: Scientific and Regulatory Challenges, an opportunity to discuss how to approach complex generics. Regulatory officials described how agencies approach evaluating complex generics for marketing approval, while industry speakers presented several examples that demonstrate the difficulties in characterizing complex drugs.
The symposium was presented by the Non Biological Complex Drugs Working Group, the Nanotechnology Characterization Laboratory, and the New York Academy of Sciences.
Lawrence Mayer, senior vice president of discovery at Jazz Pharmaceuticals, has played a lead role in the discovery and development of a number of oncology drugs, several of which eventually achieved market approval. He has also held senior management positions at The Canadian Liposome Company and QLT, Inc. before joining the British Columbia (BC) Cancer Agency, where he established and directed the Health Canada-accredited Investigational Drug Program. Celator Pharmaceuticals, now a subsidiary of Jazz Pharmaceuticals, was formed in 2000 as a spin-out of Mayer’s laboratory at the BC Cancer Agency. Mayer has authored more than 250 scientific publications and has more than 35 patent families awarded or pending. Mayer received his BS in both chemistry and biology, summa cum laude, from Wartburg College and his PhD in biochemistry from the University of Minnesota.
Daan Crommelin is professor emeritus at the Department of Pharmaceutics at Utrecht University. Until December 2011 he was scientific director of the Dutch Top Institute Pharma in Leiden. He is adjunct professor at the Department of Pharmaceutics and Pharmaceutical Chemistry at the University of Utah. Crommelin is co-founder of OctoPlus, a Leiden based company specialized in the development of pharmaceutical (mainly protein based) product formulations and advanced drug delivery systems. He published extensively and is on the editorial board of 10 peer reviewed journals in the pharmaceutical sciences. He is Editor-in-Chief of the AAPS book series Advances in the Pharmaceutical Sciences. He advises venture capital groups and acts as consultant. He chairs the UCAB Foundation: the Utrecht Center of Excellence for Affordable Biotherapeutics, a WHO supported initiative. He chaired the Board of Pharmaceutical Sciences of the International Pharmaceutical Federation (F.I.P.), was chair of the organizing committee of the Pharmaceutical Sciences World Conference 2007 in Amsterdam. He is past president of the European Federation of Pharmaceutical Sciences (EUFEPS) and past vice-chair of the scientific advisory board of the European Innovative Medicines Initiative (IMI).
A pharmacist by training, Beat Flühmann holds a PhD in molecular biology. In his current position Flühmann serves as global lead on non-biological complex drugs at Vifor Pharma Ltd Switzerland, with a main interest in regulatory aspects of nanomedicines. Previously, Flühmann led a global multidisciplinary research and development team at Roche/DSM nutritional products developing novel compounds for the prevention and treatment of diabetes. He also is a steering committee member of the Non-Biological Complex Drugs Working Group hosted at the nonprofit Lygature, a group set up to discuss science-based approval and post-approval standards to ensure patient safety and benefit with non-biological complex drugs. The working group engages in activities to publish and discus scientific evidence with authorities, experts, health care providers, and is involved in scientific education and training to relevant stakeholders. Flühmann also sits on the advisory board of the GoNanoBioMat project, a multinational research project in the field of nanomedicine.
Joseph L. Glajch is director of analytical development at Momenta Pharmaceuticals. He received his AB in chemistry at Cornell University and PhD in analytical chemistry at the University of Georgia under L.B. (Buck) Rogers. He has held technical and R&D management positions at DuPont, Bristol-Myers Squibb, Certus, and Momenta, with an emphasis on HPLC column and method development and pharmaceutical development and analysis. He has served as president and program chairman of the Analytical Division of the American Chemical Society and the Chromatography Forum of the Delaware Valley, as well as program chair of the Gordon Conference on Analytical Chemistry. He has served on the editorial advisory boards of Analytical Chemistry, the Journal of Chromatography, and LC/GC. He is a member of the USP Expert Committee on General Chemical Analysis and has over 40 publications, is co-author of three books, and holds six patents on HPLC column materials and medical imaging agents.
Elwyn Griffiths, PhD, DSc
World Health Organization and Health Canada publications
Elwyn Griffiths is currently a consultant in vaccines and biotherapeutics to WHO and a member of the WHO Expert Committee on Biological Standardization. He is also a member of the Clinical Trials, Biologicals and Vaccines Expert Advisory Group of the UK Commission on Human Medicines and of the Expert Advisory Group on Biological and Biotechnology products of the British Pharmacopoeia Commission.
In 2011, Griffiths retired as director general, biologics and genetic therapies directorate of Health Canada, an organization he joined in 2003 upon retirement from the World Health Organization. Griffthis holds a PhD and a DSc degree from the University of Wales. In 1980, he became a senior member of staff at the UK National Institute for Biological Standards and Control, and in 1994 was appointed chief of biologicals at WHO. From 1994 until the end of 2002, Griffiths was responsible for WHO’s program for providing international written and physical standards for vaccines, blood products and biotherapeutics.
Iris Grossman, VP, global head of the Personalized & Predictive Medicine (PPM) and Big Data Analytics unit for Teva Global R&D, is currently charged with defining and implementing Teva’s global PMP strategy, covering both discovery and development R&D programs. Israel’s leading financial magazine, Globes Magazine, selected Grossman as one of the country’s top 40 professionals under 40 years of age in 2013.
Prior to joining Teva, Grossman was CEO and president of the pharmacogenetics management consultancy IsraGene Ltd.. This followed several years of spearheading pipeline pharmacogenetic programs for industry and academia as director of pharmacogenetics at Cabernet Pharmaceuticals Inc. Grossman moved into consultancy having been responsible for running large-scale pharmacogenetic programs at GlaxoSmithKline, with an emphasis on infectious and neurological diseases.
Grossman received her PhD from the Technion–Israel Institute of Technology, where her research project, conducted in collaboration with the Weizmann Institute for Science, investigated pharmacogenetic markers of multiple sclerosis treatment response.
Wenlei Jiang, PhD
Office of Research and Standards, Office of Generic Drugs, US Food and Drug Administration website | publications
Wenlei Jiang is currently a senior science advisor in the Office of Research and Standards (ORS)/Office of Generic Drugs (OGD)/Center for Drug Evaluation and Research (CDER). She is mainly responsible for coordinating post-market generic drug safety investigation, representing ORS on OGD’s new international harmonization activities, and developing opportunities for scientific outreach. Previously, she served as the acting deputy director of ORS, where she provided oversight on Generic Drug User Fee Act (GDUFA) regulatory science research programs. She used to work in the Division of Chemistry, OGD to review the chemistry and manufacturing control (CMC) sections of ANDAs. Prior to joining FDA, she was at Novartis Pharmaceutical Corporation where her responsibilities included formulation development of conventional liquid and solid dosage forms, as well as advanced parenteral drug delivery systems. She received her PhD in pharmaceutics and pharmaceutical chemistry from Ohio State University in 2001.
Scott McNeil serves as director of the Nanotechnology Characterization Laboratory (NCL) for Leidos Biomedical Research and Frederick National Laboratory for Cancer Research, where he coordinates preclinical characterization of nanotech cancer therapeutics and diagnostics. At the NCL, McNeil leads a team of scientists responsible for testing candidate nanotech drugs and diagnostics, evaluating safety and efficacy, and assisting with product development. McNeil is a member of several working groups on nanomedicine, environmental health and safety, and other nanotechnology issues. He is an invited speaker to numerous nanotechnology-related conferences and has several patents pending related to nanotechnology and biotechnology. He is also a vice president at Leidos Biomedical Research.
McNeil’s professional career includes tenure as an Army officer, with tours as chief of biochemistry at Tripler Army Medical Center, and as a combat arms officer during the Gulf War. He received his bachelor’s degree in chemistry from Portland State University and his doctorate in cell biology from Oregon Health Sciences University.
Kouros Motamed, PhD has been the Director of Drug Development at NantBioScience, Inc. since April 2016. Prior to that, he has served as VP of Strategic Alliances and Clinical Communications and VP of Clinical Development and Nanomedicine at Sorrento Therapeutics from 2013 to 2016. He has also served as a co-founder and CSO/CTO of Igdrasol, Inc. and Biomiga Diagnostics start-up companies from 2011–2013. Dr. Motamed has also served as the MOA and Molecular Biology Group Head at Celgene Corp. and Abraxis BioScience Inc. from 2007–2011. Dr. Motamed held an Assistant Professorship position in the Department of Pathology and Vascular Biology Center at Georgia Health Sciences University from 2002–2007. He has over 30 original publications in peer-reviewed journals, over 50 conference presentations and has 5 issued patents. He has served on the Editorial Board of Journal of Nanomaterials & Molecular Nanotechnology since 2013. Dr. Motamed received a BS degree in Biology from University of San Francisco and a PhD degree from the University of California, Davis in Microbiology.
Stefan Mühlebach, regulatory science lead for non-biological complex drugs at Vifor Pharma–Fresenius Medical Care Renal Pharma Ltd. (Switzerland), chairs the Non-Biological Complex Drugs (NBCDs) Working Group at Lygature, a nonprofit, private-public partnership in the Netherlands. He is a university professor, medical faculty member, and member of the clinical pharmacy & epidemiology unit at the Department of Pharmaceutical Sciences at the Natural Sciences Faculty (Switzerland). Research activities, graduate and postgraduate teaching cover topics in pharmacology, clinical nutrition, hospital pharmacy, and regulatory sciences. He has authored over 100 peer-reviewed papers and several book chapters. From 1980 to 2005, he served as a chief hospital pharmacist in Switzerland. He is an honorary member of the Swiss Association of Public Health Administration and Hospital Pharmacists and a board member of the Swiss Academy of Pharmaceutical Sciences. In 2008, he joined Vifor Pharma Ltd as chief scientific officer.
Chetan Pujara is vice president, small molecule product development at Allergan, Plc. His organization is responsible for designing and developing pharmaceutical dosage forms intended for clinical trials and commercialization. SMPD develops topical sterile ophthalmic solutions, suspensions and emulsions, sustained-release ocular biodegradable implants, oral tablets/capsules, topical dermal gels & creams and other locally acting dosage forms. Prior to joining Allergan, Chetan was employed by Abbott Laboratories/Abbvie, where he held various positions in global pharmaceutical R&D, gaining experience in development of solid oral dosage forms and pediatric oral suspensions.
Pujara is also a member of the USP Dosage Forms Expert Committee and serves on the USP <771> Ophthalmic Preparation Expert Panel. He serves as a scientific advisor to the editors of Journal of Pharmaceutical Sciences and an adjunct professor in the Department of Industrial and Physical Pharmacy, Purdue University. Pujara has also contributed to the Physical Properties Working Group of Product Quality Research Institute.
Andre Raw, PhD
Center for Drug Evaluation and Research, US Food and Drug Administration website | publications
Andre Raw received his BS from the Massachusetts Institute of Technology and his PhD in chemistry from the University of California at Berkeley. He 2001, he joined the FDA as a reviewer within the Office of Generic Drugs, where he is currently acting senior scientific and policy advisor in the Office of Lifecycle Drug Products in the Office of Pharmaceutical Quality. Raw was involved in the development of several FDA initiatives, including the Guidance on Pharmaceutical Solid Polymorphism in Abbreviated New Drug Applications (ANDAs), Regulations on Listing of Polymorph Patents in the “Orange Book,” and Question Based Review – Quality by Design (QbD) Initiative, QbD Example for Generic Modified Release Products, and Guidance for Industry: Pharmaceutical Solid Co-Crystals. He has also been active in addressing scientific and regulatory issues raised in citizen petitions. He was instrumental in FDA’s recent approval of generic versions of complex active ingredients including Lovenox (enoxaparin sodium), and Ferrlecit (sodium ferric gluconate complex in sucrose).
Stephan Stern is acting deputy director and senior principal scientist at the National Cancer Institute’s Nanotechnology Characterization Laboratory (NCL), located at the Frederick National Laboratory for Cancer Research in Frederick, Maryland. NCL assists in all phases of the nanomedicine drug development process, from early preclinical to late stage clinical trials, working with academic laboratories and the pharmaceutical industry. At NCL, Stern oversees nanomedicine pharmacology and toxicology. Stern’s research interests include novel drug formulation, bioanalytical method development, and pharmacokinetic modeling. Prior experience includes a postdoctoral fellowship at the University of North Carolina–Chapel Hill in the Division of Drug Delivery and Disposition, and curriculum in toxicology, and work within regulated areas of the pharmaceutical industry. He received his BS in biochemistry from the University of Rochester and his PhD in toxicology from the University of Connecticut at Storrs. Stern is a diplomate of the American Board of Toxicology.
Wyatt Vreeland, PhD
The National Institute of Standards and Technology publications
Wyatt Vreeland earned his PhD in chemical engineering from Northwestern University, where he developed techniques for the electrophoretic separation of natural and synthetic polymers in microfluidic devices. Later, Vreeland joined National Institute of Standards and Technology as an National Research Council postdoctoral, where Vreeland focused on using liposomes to package chemicals and release those reagents at controlled times and locations in microfluidic systems. Additionally, during his postdoctoral fellowship he undertook the technical development of a field-portable electrophoresis system for forensic DNA analysis for the Department of Justice. Most recently, Vreeland’s research has focused on controlled synthesis and characterization of colloidal protein systems as can be encountered (usually undesirably) in many of today’s complex drug therapeutics. In 2015, Vreeland served as an U.S. State Department Embassy Science Fellow for the U.S. Embassy in Prague, Czech Republic, where he toured the country’s burgeoning biotechnology industry.
Gary West is currently a member of the board of directors of Azaya Therapeutics. A retired radiation oncologist, he graduated from the University of Colorado Medical School and did his radiation oncology residency at the University of New Mexico, where he was affiliated with New Mexico’s Los Alamos Meson Facility (LAMF), before completing his residency at the Joint Center for Radiation Oncology (JCRO), Harvard University. He completed a research fellowship at JCRO, where he investigated chemotherapy drug delivery in human tumor cells. While in the Air Force, he was chief of the radiation oncology department at Wilford Hall USAF Medical Center. He has also served as chief of staff at the University of Texas Health Science Center, Cancer Therapy, and Research Center (CTRC), in San Antonio and as a member of the CTRC board of governors. He is a retired member of the American Society of Clinical Oncologists and the American Society of Therapeutic Radiologists.
Elena Wolff-Holz is medical assessor at the Paul-Ehrlich-Institut and a member of the Biosimilar Working Party (BMWP) of the Committee for Medicinal Products for Human Use (CHMP) and a national expert to the Oncology Working Party (OWP) of the CHMP, where she contributes to scientific advice procedures and the development of guidelines and reflection papers. Wolff-Holz spent 14 years in the biotech industry, where she held various positions in clinical development and medical marketing functions at Centocor Inc (now J&J) and Amgen in the U.S. and in Germany, before joining the German national regulatory agency. In the area of biotherapeutics, she is responsible for advising companies on drug development issues, reviewing applications for marketing authorization in the EU and assessing clinical trial applications. She is also a lecturer covering training of experts and executives from academia, regulatory bodies and biopharmaceutical industry. Wolff-Holz has an MD degree from Heidelberg University and a postdoctoral fellowship at Harvard Medical School.
Gillian Woollett, SVP at Avalere, where she leads the FDA Policy and Regulatory Strategy Practice, an advisory services firm she launched in 2012 that supports clients throughout the healthcare system, from patients to biopharma companies and payers/providers. Woollett and her team translate into practical action all aspects of regulatory engagement strategy and policy development relevant to commercial success for multiple multi-national clients. Concurrently, she created the Avalere FDA Fellows Program to enable scientists to transition effectively into the policy environment with over 20 now having used this stepping stone to transition careers. Woollett earned her BA and MA in biochemistry from the University of Cambridge, and her DPhil in immunology from the University of Oxford. She was a postdoc in the Department of Molecular Biology at the University of Edinburgh, and at the Biomedical Research Institute, Rockville, MD funded by USAID.
Jon de Vlieger, PhD
Non Biological Complex Drugs Working Group and Lygature website | publications
Jon de Vlieger obtained his doctoral degree in bio analytical chemistry from Vrije University (the Netherlands). In 2011, he joined Top Institute Pharma, an independent nonprofit organization based that catalyzes the development of new medical solutions for patients by driving public–private collaboration between academia, industry, and society. Recently, a merger between leading Dutch technology institutes Center for Translational Molecular Medicine and Top Institute Pharma formed Lygature. For Lygature, de Vlieger coordinates several international public private partnerships, including the Non Biological Complex Drugs Working Group, an international network of scientific and clinical experts from academia, industry and regulatory bodies, with expertise in many aspects of the development and evaluation of NBCDs. He is a co-editor of the book on NBCDs in the American Association of Pharmaceutical Scientists’ Advances in the Pharmaceutical Sciences Series.
Organizers
Melanie Brickman Borchard, PhD, MSc The New York Academy of Sciences
Alison Carley, PhD The New York Academy of Sciences
Daan J.A. Crommelin, PhD Utrecht University
Wenlei Jiang, PhD Office of Research and Standards, Office of Generic Drugs, US Food and Drug Administration
Scott McNeil, PhD Nanotechnology Characterization Laboratory
Vinod Shah, PhD Non Biological Complex Drugs Working Group
Jon de Vlieger, PhD Lygature
Presented by
How to cite this eBriefing
The New York Academy of Sciences. Equivalence of Complex Drug Products: Scientific and Regulatory Challenges.Academy eBriefings. 2016. Available at: www.nyas.org/ComplexDrugs16-eB
Introduction
Speakers
Jon de Vlieger Non Biological Complex Drugs Working Group
Scott McNeil Lygature and Nanotechnology Characterization Laboratory
According to the Generic Pharmaceutical Association, almost 90% of prescriptions in the United States in 2015 were for generic drugs. Because generics are considered identical to their branded counterparts, pharmaceutical companies can forgo costly large-scale clinical trials. Instead, companies must demonstrate that a generic has pharmaceutical equivalence and bioequivalence to a licensed product. Pharmaceutical equivalence refers to the active ingredient, dosing, and strength, and can be confirmed via chemical and analytical methods. Bioequivalence refers to how a drug acts in the body and is evaluated via pharmacokinetic and/or pharmacodynamic studies. If these two conditions are met, regulatory agencies consider the generic to be safe and efficacious based on the clinical studies conducted on the branded drug.
Demonstrating the equivalence of generic complex drugs to their branded counterpart has unique challenges not encountered with small molecules.
Despite the success and advantages of generic drugs, users of certain drug categories, such as orally inhaled drugs used to treat asthma, currently have no access to generic counterparts. In addition, less than 50% of ophthalmic products and less than 40% of topical drugs have generic versions. That’s largely because these drugs represent complex drug products. In the newly released Generic Drug User Fee Act (GDUFA) “Regulatory Science Pritories,” the FDA defines complex drugs as those having complex active ingredients, such as peptides, polymers, or complex mixtures; complex formulations and/or dosages, such as liposomes, iron colloids, and long-acting injectables; complex routes of delivery, such as locally acting drugs, ophthalmic drugs, suspensions, emulsions, and gels; and/or complex drug–device combinations, such as nasal sprays and inhalers.
Demonstrating the equivalence of generic complex drugs to their branded counterpart has unique challenges not encountered with small molecules. First, the active components of complex drugs are often unknown, as are the critical attributes, i.e., the physical and chemical characteristics essential for efficacy and safety. Complex drugs are also difficult to fully characterize, and the products are very sensitive to changes in manufacturing, which is often proprietary.
In addition to above mentioned complex drug categories, the symposium also addressed biosimilars, generic versions of biologics, such as monoclonal antibodies, which share several of the hurdles to demonstrating equivalence.
Drugs can be classified into three categories. Small molecules are easy to characterize and to demonstrate equivalence. Biologics and complex drugs are more complicated, and it is difficult to demonstrate equivalence. (Image courtesy of Stefan Mühlebach)
Lawrence Mayer of Jazz Pharmaceuticals gave the keynote address on the development of a liposome-based drug delivery vehicle designed to maintain optimal levels of two cytostatics.
Several speakers spoke about the regulatory issues for biosimilars and complex drugs. Daan Crommelin of Utrecht University and Gillian Woollett of Avalere Health outlined some of the general issues to regulating generic complex drugs. Wenlei Jiang of the US Food and Drug Administration (FDA) and Elena Wolff-Holz of the Paul Ehrlich Institute provided the perspectives of the FDA and European Medicines Agency (EMA), respectively. Elywn Griffiths of the World Health Organization (WHO) outlined the WHO’s perspective.
There were several presentations on the approval of Glatopa (glatiramer acetate injection), a generic version of Copaxone (glatiramer acetate injection) for the treatment of multiple sclerosis. Andre Raw of the FDA outlined the evidence that the FDA required for approval of Glatopa while Joseph Glajch of Momenta Pharmaceuticals described the company’s approach to developing and characterizing it. Iris Grossman of Teva Pharmaceuticals presented data that show differences between the brand name drug and its generic counterpart.
Several generic versions of iron sucrose have been approved throughout the world. Stefan Mühlebach of Vifor Pharma presented evidence that several iron sucrose similars (ISS) are less effective than their branded counterparts. Beat Flühmann, also of Vifor, discussed his work on understanding pharmacists’ perspective on ISS.
Three speakers presented their approaches to evaluating the equivalence of complex drugs. Chetan Pujara of Allergan presented data on analyzing the equivalence of ophthalmic emulsions. Gary West of Azaya Therapeutics discussed regulatory hurdles to developing a generic form of Doxil (doxorubicin HCl liposome injection). Kouros Motamed of NantBioScience discussed the company’s efforts to develop a new drug delivery method for the cytostatic paclitaxel.
Two speakers focused on technical challenges to characterizing complex drugs. Wyatt Vreeland of the National Institute of Standards and Technology (NIST) described the advantages and caveats of several techniques to measure nanoparticle size. Stephan Stern of the Nanotechnology Characterization Laboratory (NCL) described a new technique to more accurately measure nanomedicines in the blood.
Speaker Presentation
Keynote Presentation
Keynote Speaker
Lawrence Mayer Jazz Pharmaceuticals
Highlights
Drug-delivery vehicles can control the pharmacokinetics of drug combinations to maintain a drug ratio that maximizes efficacy while minimizing toxicity.
Vyxeos, a nanoscale drug delivery system, was developed to deliver two chemotherapies, daunorubicin and cytarabine, in a 5-to-1 molar ratio.
In Phase 3 trials, Vyxeos demonstrated improved overall survival compared to daunorubicin plus cytarabine in patients with acute myeloid leukemia.
Built to scale
Lawrence Mayer described the development of Vyxeos (formerly CPX-351), a drug delivery system in Phase 3 trials for the treatment of acute myeloid leukemia (AML).
Vyxeos is a liposome-based drug delivery system that delivers the chemotherapies daunorubicin and cytarabine in a 5-to-1 ratio. In various cancer cell lines, this ratio was shown to have either additive or synergistic efficacy. Mayer described several of the technical features that can be altered to achieve the desired drug release rate, including membrane rigidity, charge, cholesterol content, and copper content.
The relative ratios of the chemotherapies cytarabine and daunorubicin can affect the combination’s efficacy. Some ratios are synergistic, while others are additive or antagonistic. (Image courtesy of Lawrence Mayer)
Vyxeos was compared to the current chemotherapy regimen of cytarabine and daunorubicin in two Phase 2 and one Phase 3 clinical studies in patients with AML. In all three trials, patients treated with Vyxeos had a significantly higher overall survival. Other indicators of efficacy, such as response rates and post-transplant survival were also better in patients treated with Vyxeos. Jazz Pharmaceuticals is pursuing FDA approval of Vyxeos. The FDA granted the drug breakthrough status earlier this year.
Mayer stressed the importance of a scalable manufacturing process and biophysical characterization early in drug development. A well-characterized biophysical profile ensures that the product produced in large-scale production is the same as that produced and studied during small-scale testing. It also ensures that the features of the product do not vary considerably from batch to batch.
Speaker Presentation
Video Chapters 00:00 Introduction 06:00 Key to exploiting drug ratio-dependent synergy 12:34 Leukemia cell update of intact liposomes 19:18 A robust commercial-scale nanomedicine 27:00 Conclusions
Regulatory Considerations
Speakers
Daan J.A. Crommelin, PhD Utrecht University
Elwyn Griffiths World Health Organization and Health Canada
Wenlei Jiang, PhD Office of Research and Standards, Office of Generic Drugs, US Food and Drug Administration
Elena Wolff-Holz Paul Ehrlich Institute
Gillian Woollett Avalere Health
Panel Discussion Moderator:
Scott McNeil Nanotechnology Characterization Laboratory
Highlights
Regulatory pathways for small molecule generics and biosimilars are well established, while requirements for non-biologic complex drugs are considered on a case-by-case basis.
The FDA is continually investigating new pharmacokinetic data and methods to assess the bioequivalence of complex drugs.
New guidance was released by the EMA in 2014 that expands the definition of biosimilar and provides additional direction to industry.
Regulatory pathways for generics and biosimilars
Daan Crommelin began by defining some key terms relating to complex drug products and outlining the regulatory pathways for different types of drugs. According to Crommelin, drugs can be divided into three main categories: small molecules; biologics, such as vaccines, blood and blood components, gene therapies, tissues, and recombinant proteins; and non-biologic complex drugs (NBCDs), synthetic drugs that do not have a single, homogeneous active substance and cannot be fully characterized. The composition, quality and in vivo performance of NBCDs are highly dependent on the manufacturing processes of the active ingredient as well as (in most cases) the formulation. They often consist of nanomedicines such as polymeric micelles, liposomes, or peptide-polymers. Crommelin pointed out that regulatory agencies do not always agree on these definitions; while the EMA considers low molecular weight heparin a biologic, the FDA considers it a complex drug.
The regulatory pathways for small molecules and biologics are relatively well defined. For small molecules, therapeutic equivalence (TE) is assumed by demonstrating pharmaceutical equivalence (PE) and bioequivalence (BE). For biosimilars, additional data, including pharmacokinetic (PK) and (pre)clinical data are required. Unlike small molecules, biosimilars are not considered identical to the branded agent. (Image courtesy of Daan Crommelin)
The regulatory approval process for generic small molecules is well established, and generics are considered interchangeable with their branded counterpart. A separate process has been created for biologics. Similar to generics, biosimilars can be approved via an abbreviated regulatory process that usually involves pharmaceutical equivalence, pharmacokinetic, and preclinical data. Biosimilars are considered highly similar, but not identical, to the original drug.
The regulatory process for NBCDs is often conducted on a case-by-case basis. Because NBCDs cannot be fully characterized and the critical attributes required for efficacy are often unknown, it is difficult to demonstrate bioequivalence for a generic NBCD. The FDA and EMA release guidance documents for NBCD classes outlining which analyses are needed to demonstrate similarity. These documents are continually reviewed and revised.
Multi-faceted considerations for regulatory approval of biosimilars and complex drugs
Gillian Woollett stressed that the considerations for biosimilars and complex drug similars are not only scientific, but also legal, regulatory, and economic. Regulatory agencies must balance the need for scientific and clinical evidence with the need to provide patients affordable drugs in a timely manner. According to Woollett, too high a standard can be as problematic as too low a standard if it prevents access to drugs. The FDA and EMA have an additional responsibility to set a standard for the rest of the world. A product approved in the EU and US can generally be approved anywhere; however, one approved in emerging markets, such as China, Russia, and Brazil, may not be approved in other markets. In the US, only four biosimilars have been approved; however, several agents have been approved under the definition of generic biologics. In comparison, 23 biosimilars have been approved in the EU.
The considerations for biosimilars and complex drug similars are not only scientific, but also legal, regulatory, and economic.
One issue surrounding biosimilars is that they must be compared to the reference biologic approved in a given market. This can make it difficult for companies to pursue approval globally. Another issue that may need to be addressed is the addition of orphan indications to reference biologics. Because the FDA gives exclusivity for orphan indications, these indications would not be included in the biosimilar’s product label.
The FDA’s perspective on determining the equivalence of complex drugs
Wenlei Jiang described how the FDA assesses the bioequivalence of complex generics. Jiang stressed the FDA’s commitment to complex generics through the abbreviated new drug application (ANDA) approval pathway and GDUFA, which employs regulatory science initiatives for generic drugs. Specifically, Jiang showed research efforts under GDUFA that have developed new bioequivalence methods for complex drugs.
Traditional pharmacokinetic studies to demonstrate the bioequivalence of complex drugs are difficult to conduct. For some drugs, such as long-acting polymeric microspheres, which are commonly used in drug delivery, their long-acting nature would require very long studies, which may be impractical. Based on pharmacokinetic modeling research conducted by Alkermes, the FDA updated its guidance on the bioequivalence requirements for long-acting polymeric microspheres to include drug exposure up to 28 hours.
For complex drugs that act locally, such as topical skin products and nasal sprays, conventional studies that monitor drug blood levels may not be relevant. The FDA has sponsored research on new options for dermal pharmacokinetic studies, such as open-flow microperfusion (see slide).
Open-flow microperfusion can be used to monitor drug levels of topical creams in the dermis. (Image courtesy of Wenlei Jiang)
Jiang also presented a new analytic technique, morphology-directed Raman spectroscopy (MDRS), that can determine drug particle size and shape within a nasal suspension. MDRS has supported the recent approval of mometasone nasal suspension.
CHMP/EMA perspective on biosimilars
Elena Wolff-Holz described the EMA’s perspective on evaluating biosimilars and how the process has evolved over time. The EMA releases several overarching and product-specific guidelines, which are continually reviewed and revised. In a recent update to the overarching guidance (CHMP/437/04 Rev. 1), the EMA expanded the concept of a biosimilar to any biological medicinal product, including vaccines, allergens, and cell and tissue therapies, which were previously excluded. It also stressed that a biosimilar contains “a version of the active substance of an already authorized original biological medicinal product,” implying that biosimilars should not be used as reference products. In the new guidance, the goal of clinical data is to address slight differences in product characteristics, and safety and efficacy do not need to be re-established. Finally, if the reference biologic receives a new indication, the indication of the biosimilar may also be extended without the need for additional studies, if scientifically justified.
The evolution of biosimilars in the EU. New legislation is shown in red; new EMA guidelines are shown in green, and new authorizations are shown below the blue arrow. (Image courtesy of Elena Wolff-Holz)
Wolff-Holz noted that the approval process for biosimilars, which emphasizes physicochemical properties, can be difficult for clinicians, who want to know the clinical information for a drug, to accept. While clinical data for biosimilars are not included in the product’s Summary of Product Characteristics (SmPC), they are in the European Public Assessment Reports (EPAR), which clinicians are not as familiar with.
The WHO’s role in biosimilars and complex generics
Elwyn Griffiths described WHO’s role and position on biosimilars. While WHO is not a regulatory agency, it sets global standards for safety and quality. The WHO Expert Committee on Biological Standardization meets annually to establish recommendations and guidance on the quality, safety, and efficacy of biologics.
There are three major WHO guidance documents pertaining to biologics and biosimilars: Guidelines on the quality, safety and efficacy of biotherapeutic protein products prepared by recombinant DNA technology, published in 2013, Recommendations for the evaluation of animal cell cultures as substrates for the manufacture of biological medicinal products and for the characterization of cell banks, published in 2010, and Guidelines on the evaluation of similar biotherapeutic products, published in 2009.
The 2009 guidelines on similar biotherapeutics define similar biotherapeutic products (SBPs) as similar in terms of quality, safety, and efficacy to a licensed reference biological product (RBP). Similarity is established by characterizing the SBP and comparing it to the RBP in head-to-head studies. Comparison trials should be designed to detect differences in safety and efficacy between the SBP and RBP, not to establish the efficacy of the SBP. The guidelines also state that if an RBP has more than one indication, the indication of the SBP may also be expanded if scientifically warranted. One subject the WHO guidelines leave up to national regulatory agencies is whether SBPs should be considered interchangeable with RBPs.
Speaker Presentations
Video Chapters 00:00 Introduction 01:52 Complex drug products definitions 07:47 Three drug classes 13:16 What is the issue? 17:47 No access to biosimilar pathway for NBCD-similars
Video Chapters 00:00 Introduction 03:35 WHO biological standards 09:29 Regulatory oversight of biotherapeutics 15:13 WHO guidelines on evaluation of similar biotherapeutic product 23:38 Summary WHO standards
Video Chapters 00:00 Introduction 02:32 NDA versus ANDA 07:12 Consideration on PLGA sameness 13:24 Challenges for therapeutic equivalence of nasal spray products 15:13 Scientific rationale for weight-of-evidence approach 20:54 Summary
Video Chapters 00:00 Introduction 03:03 Scope includes next generation biosimilars 10:43 Manufacturing changes authorized by EMA 18:09 What if PK similarity is not convincingly demonstrated?
Video Chapters 00:00 Introduction 01:38 Working definitions for biologics 05:51 Biologic approvals have increased and are expected to rise 10:27 Biosimilars approvals across the world 18:58 Biosimilars represent a new and different business
Video Chapters 00:00 Introduction 00:50 Thoughts on the definition of the API and does it need to be updated 05:48 Measuring release of drugs 07:40 Critical factors, quality attributes for complex drugs 17:51 Looking forward to how further complexity affects biological responses 21:49 IP and open data review in a profit-driven industry
Comparisons of Copaxone (glatiramer acetate injection) with Its Generic Glatopa (glatiramer acetate injection)
Speakers
Joseph Glajch Momenta Pharmaceuticals
Iris Grossman Teva Pharmaceuticals
Andre Raw U.S. Food and Drug Administration
Highlights
Glatopa (glatiramer acetate injection), an FDA-approved generic of Copaxone(glatiramer acetate injection) is considered similar to the branded product based on the tests required by the FDA.
Additional comparisons have revealed differences between the drugs that may affect safety and efficacy.
Glatopa: a complex generic drug for multiple sclerosis
Glatopa was approved by the FDA in 1996 as a generic version of Copaxone for the treatment of multiple sclerosis. These drugs consist of glatiramer acetate, a complex mixture of polypeptides produced by polymerizing four amino acids and then partially depolymerizing the resulting peptides.
Scientific considerations to approaching complex generics
Andre Raw discussed the scientific considerations to approaching generic versions of Copaxone (glatiramer acetate) and Lovenox (enoxaparin sodium) injections, two of the complex active ingredients recently approved in generic versions by the FDA. Raw argued that understanding the nature of the complexity of these drugs is key to evaluating generic similars. For instance, the complexity of Copaxone comes from the polymerization of activated amino acids, which determines the sequences of the polypeptides, and the subsequent partial depolymerization.
To ensure similarity of Copaxone and Lovenox similars, the FDA drafted guidance listing four criteria that generic products must meet. First, the pharmaceutical company must demonstrate equivalence in its reaction scheme. Second, the FDA places constraints on several physicochemical properties, such as molecular weight distribution and amino acid composition. This also means that the structural signatures, which reflect the polymerization and depolymerization processes, and biological assays will be similar as well.
The third criterion requires that generic manufacturers identify “process signatures;” equivalence in these signatures ensures that the generic active ingredient is manufactured with effectively the same polymerization kinetic and cleavage biases as the brand name. Finally, the fourth criterion relies on the equivalence of biochemical and/or biological markers for activity to ensure sameness. Unlike the previous three criteria, which in their aggregate ensure equivalency of molecular diversity, this criterion serves as a confirmatory test to ensure equivalency in functional biochemical or biological markers.
Comparison of Copaxone and Glatopa for FDA approval
Joseph Glajch described the tests that Sandoz conducted to demonstrate the equivalence of Glatopa and Copaxone. In approximately 50 physiochemical and 10 biological tests, Glatopa fell within an acceptable range considered to be equivalent to Copaxone. Glajch stressed that these analyses must be conducted on dozens of lots to understand the diversity and variability within the drug. He showed the data from some of these analyses, including molecular weight distribution, amino acid composition, and structural signatures. He also showed that the drugs have similar effects on disease intensity in a model of autoimmune encephalomyelitis and similar results on histamine release from cells.
Additional comparisons of Copaxone and Glatopa
While Raw and Glajch showed that Glatopa and Copaxone are similar according to the methods required by the FDA, Iris Grossman described studies using higher-resolution techniques conducted by Teva Pharmaceuticals that reveal differences in surface charge and molecular weight density and distribution. In addition, Glatopa had greater batch-to-batch variability in these characteristics than Copaxone.
Copaxone and Glatopa are similar based on the physicochemical tests required by the FDA (rows 1, 2, and 4). However, other, higher-resolution methods demonstrate differences. (Image courtesy of Iris Grossman)
These differences may have consequences on efficacy and safety. In mice, of the thousands of genes affected by Glatopa and Copaxone, approximately 10% were different between the two drugs. The genes that differed were involved in pathways important for efficacy, including inflammation and immune response.
Based on these results, Teva has submitted comments on the draft FDA guidance on glatiramer acetate injections.
Speaker Presentation
Video Chapters 00:00 Introduction 02:37 Physicochemical differences relevant to mode of action 10:22 Relevance of differences to function and safety 13:50 Immunological triad 17:25 Functional effects summary and conclusions
Issues with Iron Carbohydrate Similars
Speakers
Beat Flühmann Vifor Pharma Ltd
Stefan Mühlebach, PhD Vifor Pharma Ltd
Panel Discussion Moderator:
Daan J.A. Crommelin Utrecht Universit
Highlights
Several approved generics of iron carbohydrate complexes are not as effective as their branded counterparts.
Hospital pharmacists are not aware of the differences between iron carbohydrate products and often substitute these products without informing a patient’s physician.
Iron carbohydrate similars
Iron carbohydrate products are used to treat anemia in patients with chronic kidney disease. Several iron carbohydrate generics were approved in Europe in the mid-2000s. According to Stefan Mühlebach, there was no regulatory process for complex similars at this time, and the drugs were approved via the small molecule generic route. Researchers and regulators were not aware that the active pharmaceutical ingredient was not fully characterized, and iron carbohydrate similars were deemed identical to and interchangeable with the original drugs without additional efficacy or safety studies. Since then, real-life clinical studies have shown that show the approved iron carbohydrate similars are not clinically identical to the original formulations.
The EMA and FDA have reacted to these data and have published several guidance papers on iron carbohydrate similars.
The hospital pharmacist’s approach to iron complex carbohydrates
Beat Flühmann of Vifor Pharma described the pharmacist’s perspective of complex generics using iron sucrose, a type of iron carbohydrate, as an example. In a survey hospital pharmacists in France and Spain, Flühmann found that pharmacists substitute 30% to 50% of branded iron sucrose prescriptions with a generic version. Approximately 40% of pharmacists believed that the products have the same efficacy and safety, while the remaining 60% had no opinion. In addition, many pharmacists did not inform the physician that they had dispensed the generic version.
Despite clinical data that show significant differences in efficacy and safety among iron sucrose similars, most pharmacists are not aware of these differences. (Image courtesy of Beat Flühmann)
Flühmann stressed the importance of educating pharmacists on the differences in biosimilars and complex generics. Vifor conducted a roundtable discussion earlier this year with leading hospital pharmacists throughout Europe to discuss how to select nanosimilars for hospital formularies. The roundtable added several criteria for hospital formulary committees to consider when selecting a nanosimilar, including particle size and size distribution, pharmacokinetics, and stability of ready-to-use formulations.
Speaker Presentations
Video Chapters 00:00 Introduction 04:40 Therapeutic equivalence from manufacturing to efficacy and safety 09:32 Current situation for follow-on approval 14:48 NBCD product evaluation 18:32 Landscape of drugs follow-ons
Video Chapters 00:00 Introduction 03:11 Making biosimilars available globally 08:25 The unbound drug vs release and release mechanisms 12:11 Interchangeability and acceptability in the market 16:27 Proposed systems for biosimilars and for currently approved biologics 20:12 Concluding thoughts
Other Case Studies of Complex Generics
Speakers
Kouros Motamed NantBioScience, Inc.
Chetan Pujara Allergan
Gary West Azaya Therapeutics
Highlights
The bioequivalence of Cynviloq, a polymeric micelle formulation of the chemotherapy paclitaxel, and Abraxane (paclitaxel protein-bound particles for injectable suspension), an approved albumin-bound paclitaxel, is being investigated in the study TRIBECA.
Robust criteria are needed to ensure the equivalence of different ophthalmic emulsions.
Greater harmony between the FDA and EMA could streamline the approval of a generic version of Doxil (doxorubicin HCl liposome injection).
Cynviloq: a new formulation of paclitaxel
Kouros Motamed discussed a polymeric micelle formulation of the chemotherapy paclitaxel, Cynviloq, which is approved in several Asian countries for breast and lung cancer under the brand name Genexol-PM. These approvals were based on comparisons to Taxol (paclitaxel), a formulation of paclitaxel containing the excipient Cremophor EL. In the US and EU, approval requires comparison to Abraxane, an albumin-bound formulation of paclitaxel approved for breast, lung, and pancreatic cancer.
Evolution of paclitaxel therapies. (Image courtesy of Kouros Motamed)
In in vitro studies, Abraxane and Cynviloq had similar pharmacokinetic properties at therapeutic doses. At higher doses, the Abraxane concentration sharply increased, resulting in increased toxicity. The concentration of Cynviloq, however, did not increase as quickly, and therefore may be less toxic at higher doses.
A pharmacokinetic bioequivalence study, TRIBECA, was conducted in patients with metastatic breast cancer. Sorrento Therapeutics issued a press release stating that TRIBECA demonstrated bioequivalence of Abraxane and Cynviloq. In 2015, Cynviloq was acquired by NantWorks and has been renamed Nant-paclitaxel.
Demonstrating equivalence of ophthalmic emulsions
In 2013, the FDA released draft guidance on cyclosporine emulsions. To test whether this guidance was sufficient, Allergan tweaked its manufacturing process to make nine cyclosporine emulsions similar to Restasis (cyclosporine ophthalmic emulsion). Chetan Pujara showed that although these emulsions met the FDA criteria for similarity, there were key physicochemical and biological differences. For example, the cyclosporine distribution between the phases of the emulsion varied between the drugs. This corresponded with differences in the drug’s ability to permeate human corneal cells. Allergan also saw variability in the amount of cyclosporine in tears in rabbits.
The updated FDA guidance, released in 2016, incorporates suggestions by Allergan based on these data. However, Pujara stressed that further research on linking in vitro results to in vivo performance and on robust methods to characterize emulsions is still needed.
Regulatory barriers to a generic version of Doxil
Gary West called for harmony between regulatory authorities, citing the recent difficulties that Azaya Therapeutics has had in gaining approval for its generic doxorubicin. Doxorubicin, a treatment for ovarian cancer, is marketed by Janssen in the US under the brand name Doxil and in the EU under the brand name Caelyx (pegylated liposomal doxorubicin hydrochloride for injection).
Can international regulatory agencies work together to remove barriers facing approval of generic drugs?
Currently, Caelyx is the reference drug for doxorubicin in the EU. In the US, the FDA established a generic version of doxorubicin, ANDA 203263, as the reference drug for doxorubicin due manufacturing concerns with Doxil. However, the FDA discovered that the plant manufacturing the generic version was not complying with several guidelines, which led to contamination. West argued that due to these issues, the FDA-approved doxorubicin generic may not be the best comparator. He showed certificates of analysis from the sole manufacturer that made both Caelyx and Doxil in 2013 that demonstrate that, at that time, the two drugs were the same product with a different label and argued that they should therefore be considered interchangeable by regulatory agencies.
Azaya Therapeutics’ investigational doxorubicin generic, dubbed ATI-0918, was shown to be bioequivalent to Caelyx. However, because the EMA requires that Caelyx be sourced within the EU, and the FDA requires generics to be compared against the reference standard ANDA 203263, the company faced regulatory hurdles from both agencies. West called upon the agencies to work together to remove the barriers facing approval of generic drugs.
Speaker Presentation
Video Chapters 00:00 Introduction 03:21 A triple-down, unintended, regulatory catch 22 09:52 Lipodox versus Sun product 18:28 Regulatory barriers 22:29 Conclusions
Analytical Techniques for Characterizing Complex Drugs
Speakers
Stephan Stern Nanotechnology Characterization Laboratory
Wyatt Vreeland The National Institute of Standards and Technology
Highlights
Choosing the right analytical method is important when measuring the size of nanoparticles.
A new method to measure plasma drug concentration for nanomedicines is being validated by the NCL.
Techniques to measure nanoparticle size
Wyatt Vreeland described the advantages and disadvantages of several techniques to measure nanoparticles size.
The most common technique for measuring nanoparticle size is batch light scattering. In this method, the particle size is determined based on their ability to scatter light waves. This method is quick, simple, and nondestructive. However, because larger particles scatter light much more than smaller particles, a small amount of large particles can drown out the signal due to smaller particles, resulting in significant errors.
To avoid this complication, mixtures can be separated by size by either size-exclusion chromatography (SEC) or field flow fractionation (FFF) and then measured by light scattering. One advantage of FFF over SEC is that it can separate delicate or soft colloidal particles, which are often components of complex drugs. FFF can be used to separate particles of a few nanometers to 1000 nanometers.
Vreeland also discussed several new techniques that measure particle size by monitoring individual particles. In nanoparticle tracking analysis (NTA), particles are imaged directly with a laser, and their size is determined by tracking the extent of diffusion over time. While NTA is a robust tool to measure particle size, it is only effective within a narrow concentration range. A second technique, resonant mass measurement measures the change in frequency a particle causes as it flows through a vibrating cantilever. In addition to size, this technique, unlike others, can also measure buoyant density; however the cantilever is prone to clogging and cannot be used to measure liposomes. Finally, electrical sensing zone measures the change in electrical conductivity as a particle travels through a pore between two electrodes. This technique is similar to Coulter counter, which is used to measure bacteria and viruses. This is a very new technique for nanoscale particles.
A new method to measure nanomedicine plasma levels
The concentration of drugs administered via nanoparticles can be divided into three forms: the nanoparticle-encapsulated form, the unencapsulated free form, and the unencapsulated protein-bound form. Current methods to separate the encapsulated from unencapsulated drug promote un-encapsulation and do not differentiate protein-bound from encapsulated drug.
In two pharmacokinetic studies of Caelyx, the measured levels of unencapsulated drug differed by 6-fold, while the levels of unencapsulated drug differed by almost 12-fold, likely due to problems in fractionation methods.
Stephan Stern presented a new stable isotope tracer technique being developed by the NCL to separate and measure nanomedicine drug fractions. NCL is working with the FDA to evaluate this method for determining the bioequivalence of generic nanomedicines. As part of this effort, the NCL is conducting in vitro bioanalytical studies as well as bioequivalence studies in rats of Abraxane and Genexol-PM, discussed by Motamed, and doxorubicin HCl and Doxil, discussed by West.
In the stable isotope tracer method, an isotopically-labeled drug is added to the blood sample. The free and bound drug forms are then separated through a semi-permeable membrane. The percentage of labeled drug that does not pass through the membrane is used to determine the percent of bound drug, which can then be used to calculate the concentrations of bound and unbound drugs. (Image courtesy of Stephan Stern)
Speaker Presentations
Video Chapters 00:00 Introduction 03:48 Nanomedicine pharmacokinetics 08:39 Sources of intra-subject variability 13:43 Novel stable isotope tracer method 19:26 Measuring unbound drug in evaluating nanomedicine pharmacokinetics
Video Chapters 00:00 Introduction 02:50 Batch light scattering 08:11 How laminar flow works in FFF 13:18 Dynamic light scattering 17:52 Resonant mass measurement 20:18 Future directions
Open Questions
How can researchers determine the critical attributes for complex drugs?
What are the best methods to characterize complex drugs?
What are the most appropriate pharmacokinetic methods to evaluate bioequivalence of complex drugs?
Should biosimilars and complex generics be considered interchangeable with their branded counterparts? What criteria are necessary to demonstrate interchangeability?
How can regulatory agencies balance the need for robust scientific and clinical evidence with the need for affordable medications when evaluating complex generics?
How can regulatory agencies reach agreements on how to evaluate complex drugs?
How can companies and regulatory agencies communicate the potential clinical differences between original and generic complex drugs?
Teva Pharmaceuticals Industries Ltd. [press release] Teva Files Citizen Petition with the U.S. Food and Drug Administration (FDA) Regarding the Complexity of COPAXONE® (glatiramer acetate) Following the Agency’s Guidance. July 3, 2014.
Wenlei Jiang
Babiskin A et al. Pharmacokinetic modeling and simulation of naltrexone for extended-release injectable suspension to derive alternative BE metrics. ACoP. 2015.
Ambardekar and Stern. NBCD Pharmacokinetics and Bioanalytical Methods to Measure Drug Release. In Daan Crommelin D and de Vlieger J (ed) Non-Biological Complex Drugs; the Science and Regulatory Landscape. Springer, New York, NY; 2015: In-press.
The processes associated with aging may be risk factors for age-related diseases. Conversely, many age-related chronic diseases accelerate aging. However, because most research is focused on specific diseases, the broad mechanisms of disease as a driver of aging have not been well studied. Understanding how disease drives aging could not only help people live longer but also improve health and quality of life during old age.
On April 13–14, 2016, researchers studying aging and three disease areas—HIV/AIDS, oncology, and diabetes—met at the New York Academy of Sciences for the Disease Drivers in Aging: 2016 Advances in Geroscience Summit. The meeting expanded on the National Institutes of Health’s 2013 Advances in Geroscience Summit, examining how chronic diseases and their treatments affect aging. The meeting also aimed to stimulate collaboration between researchers studying aging and researchers studying disease. The summit was presented by the Gerontological Society of America, the American Federation for Aging Research, the Trans-NIH GeroScience Interest Group, and the New York Academy of Sciences.
The meeting opened with four keynote presentations from geroscience researchers, followed by a series of short talks and panel discussions featuring researchers focused on HIV/AIDS, diabetes, and cancer. This eBriefing reviews the panel discussions on each disease area and the overarching discussion on common themes and ideas for collaboration between researchers studying aging and disease.
Presentations available from:
Timothy Ahles, PhD (Memorial Sloan Kettering Cancer Center) Kathryn Anastos, MD (Albert Einstein College of Medicine) Steven Austad, PhD (University of Alabama at Birmingham) James Becker, PhD (University of Pittsburgh) Caroline Blaum, MD (New York University) Judith Campisi, PhD (Buck Institute for Research on Aging) Harvey J. Cohen, MD (Duke University) Wendy Demark-Wahnefried, PhD (University of Alabama at Birmingham) Jan van Deursen, PhD (Mayo Clinic) Elissa Epel, MD (University of California, San Francisco) Kristine Erlandson, MD (University of Colorado) Brooke Grindlinger, PhD (The New York Academy of Sciences) Jeffrey Halter, MD (University of Michigan) Richard Hodes, MD (National Institute on Aging, NIH) Peter Hunt, MD (University of California, San Francisco) Beth Jamieson, PhD (University of California, Los Angeles) C. Ronald Kahn, MD (Joslin Diabetes Center) Balakuntalam Kasinath, MD (University of Texas Health Science Center) Gretchen Neigh, PhD (Virginia Commonwealth University) Rosario Scalia, MD, PhD (Temple University) Marissa Schafer, PhD (Robert and Arlene Kogod Center on Aging) Felipe Sierra, PhD (National Institute on Aging, NIH) Mary Sehl, MD, PhD (University of California, Los Angeles) Christopher Wiley, PhD (Buck Institute for Research on Aging) Panel Discussions
Presented by
How to cite this eBriefing
The New York Academy of Sciences. Disease Drivers of Aging: The 2016 Advances in Geroscience Summit. Academy eBriefings. 2016. Available at: www.nyas.org/Geroscience2016-eB
Media
00:01 1. Introduction and overview 04:25 2. What we know from basic research 11:58 3. Progress made; What we want to know; Conclusion
00:01 1. Introduction and overview 08:20 2. Chronic stress and cell aging 13:04 3. Telomeres and disease risk 15:55 4. Disease drivers; Conclusion
00:01 1. Presentation by Beth Jamieson 10:20 2. Presentation by James Becker 19:52 3. Presentation by Gretchen Neig
00:01 1. Presentation by Kathryn Anastos 10:16 2. Presentaton by Peter Hunt 20:23 3. Presentation by Kristine Erlandson
00:01 1. Introduction; HIV and aging 08:25 2. HIV and macrophages; Primate studies; Where to intervene 16:21 3. Maximizing control group resources; Biomarkers for stress 23:48 4. Regarding Alzheimer’s; Mitochondrial dysfunction; Aging and viral dormancy; Data set creation 28:56 5. Supressor mutations; Cognitive dysfunction; Conclusion
00:01 1. Presentation by Marissa Schafer 11:07 2. Presentation by Christopher Wiley 22:09 3. Presentaton by Mary Sehl
00:01 1. Presentation by C. Ronald Kahn 10:29 2. Presentation by Balakuntalam Kasinath 20:47 3. Presentation by Rosario Scalia
00:01 1. Presentation by Caroline Blaum 10:35 2. Presentation by Jeffrey Halter
00:01 1. Treatment with CDK4 inhibitors; What is accelerated aging? 09:03 2. Increased phosphorylation; Obesity, asthma, and diabetes 13:55 3. Amino acids and insulin secretion; More on accelerated aging 18:52 4. Regarding astroglial cells; The blood-brain barrier 26:40 5. Treatment with metformin; Diabetes and immunodeficiency; Rapamycin; Conclusion
00:01 1. Introduction; Choosing the right journal 04:20 2. General manuscript preparation; Discussion and introduction 11:44 3. The abstract; The title 14:38 4. Authorship; The cover letter 21:44 5. Referees; Peer review 27:44 6. Decisions; Common reasons for rejection; Revision and resubmission 34:35 7. Preparing a response; Appealing a negative decision 39:12 8. Parting thoughts; Conclusion
00:01 1. Presentation by Jan van Deursen 11:48 2. Presentation by Harvey Jay Cohen 22:09 3. Presentation by Judith Campisi
00:01 1. Presentation by Wendy Denmark-Wahnefried 10:29 2. Presentation by Timothy Ahles
00:01 1. Introduction 07:48 2. Synergy between aging and cancer research models; Aging in animal models 17:30 3. Disease interplay across disciplines; Dietary restriction; Senescent T-cells 24:12 4. Computational and systems biology; Chemotherapy and senescence; Funding 31:11 5. Anti-depressants before chemo; Intervention 40:15 6. Regarding exosomes and evolution; Conclusion
00:01 1. Panelists’ opening remarks 13:17 2. Disease treatment and lifespan extension; Targeting senescenct cells 21:06 3. Embracing complexity; Developmental manipulation in aging research; Inflammation 33:20 4. Review and funding 41:00 5. Metabolic reprogramming; Healthspan vs. lifespan; Regarding data sets 48:18 6. Mitochondrial dysfunction; Going forward; Common tools 61:28 7. Aging as disease; Stress and trauma; Drug discovery; Influence of local environment 69:28 8. Exercise; Incentivizing collaboration; Policy and funding 82:06 9. Focus on gene expression; Big data; Public perceptions 87:27 10. Cohort development; Conclusion
Sierra F, Kohanski R (eds). Advances in Geroscience. Springer International Publishing. 2016. [Ebook] Provides a comprehensive overview of geroscience.
General aging resources: journal articles
National Institute on Aging (NIA) NIA, one of the 27 Institutes and Centers of NIH, leads a broad scientific effort to understand the nature of aging and to extend the healthy, active years of life.
Jennifer Cable lives in New York City, where she experiments with different outlets to communicate science. She enjoys bringing science to scientists and nonscientists alike. She writes for Nature Structural and Molecular Biology, Bitesize Bio, Under the Microscope, and the Nature New York blog. She received a PhD from the University of North Carolina at Chapel Hill for her research in investigating the structure/function relationship of proteins.
Funding for the eBriefing of this conference was made possible, in part, by 1 R13 AG 053043-01 from the National Institute on Aging. Co-funding has been provided by the National Institute of Diabetes and Digestive and Kidney Diseases, and the National Cancer Institute. The views expressed in written conference materials or publications and by speakers and moderators do not necessarily reflect the official policies of the Department of Health and Human Services; nor does mention by trade names, commercial practices, or organizations imply endorsement by the U.S. Government.
This activity is supported by an educational grant from Lilly. For further information concerning Lilly grant funding visit www.lillygrantoffice.com
Although age is an important variable in clinical research, the effects of aging are often understudied.
Improving the quality of life during aging is as important as increasing longevity.
Short-term stress can promote resilience to aging; however, chronic stress accelerates aging.
Introduction
Aging is often accompanied by chronic diseases including heart disease, cancer, diabetes, and Alzheimer’s disease, to name a few. Many processes associated with aging may be risk factors for these diseases. While aging occurs in the absence of disease—a steady decline in health is expected as a person ages—chronic diseases also accelerate aging, exacerbating normal physical and cognitive decline.
As people age, a steady decline in health is expected (red line). Some diseases cause a temporary decrease in health followed by full recovery (first black dip). However, other diseases can change the trajectory of aging, leading to a faster decline in health (fuchsia line). (Image courtesy of Felipe Sierra)
The field of geroscience has focused on how aging affects disease, and this topic was the theme of the first geroscience summit, “Advances in Geroscience: Impact on Healthspan and Chronic Disease,” which took place in October, 2013, in Bethesda, Maryland. Papers related to that summit were published in a supplement to the Journals of Gerontology in June, 2014. However, the reverse question—how disease affects aging—has gone largely unstudied, and this topic was the theme of this 2016 meeting.
The 2016 summit examined how three diseases—HIV/AIDS, diabetes, and cancer—affect the major pillars of aging established at the first Geroscience Summit: macromolecular damage, stress response, epigenetics, stem cells, proteostasis, inflammation, and metabolism.
The meeting opened with four keynote presentations from geroscience researchers who described successful interventions to delay aging and increase life span in animal models. They also noted the need for multidisciplinary research, challenging attendees to work across disease states. Understanding common mechanisms in aging and chronic diseases could help people live not only longer but also healthier lives.The keynote presentations were followed by a series of short talks and panel discussions featuring researchers focused on HIV/AIDS, diabetes, and cancer. This eBriefing reviews the panel discussions on each disease area and the overarching discussion on common themes and ideas for collaboration between researchers studying aging and disease.
The seven pillars of aging. (Image: Kennedy BK et al., Cell 159: 709-713 [2014])
A multidisciplinary approach to aging
Richard Hodes of the National Institute of Aging (NIA) outlined the multidisciplinary structure at the NIA and National Institutes of Health (NIH) to raise awareness of the role of aging in disease and to fund aging-based research. Targeting aging may reduce the incidence of age-related diseases. The divisions of the NIA span basic biology to clinical and behavioral studies. Because aging touches so many fields, the NIH also created the Geroscience Interest Group (GSIG), with members from 21 institutes. Hodes called on researchers to step outside the silos of their specialties and to study features of aging common to disparate disciplines and diseases.
Hodes also presented evidence of the importance of considering age when choosing treatments for patients, and highlighted the need to include elderly subjects in preclinical and clinical studies. In the Diabetes Prevention Program, both medication and lifestyle changes reduced the risk of developing diabetes in at-risk patients younger than 60 years. However, in subjects older than 60, only lifestyle changes were effective. In a pre-clinical study, elderly mice with cancer died sooner when given immunotherapy than those who did not receive treatment.
Felipe Sierra, also from the NIA, pointed to the need to re-examine our approach to disease. The elderly often present with several comorbidities. Instead of considering each disease individually, researchers should consider interactions between diseases, and between disease and aging.
The keynote speakers also described efforts to promote aging research. In late 2015, the NIA released a request for applications to test whether the age of laboratory animals affects outcomes in studies investigating disease. In the NIA’s Interventions Testing Program (ITP), researchers can submit compounds to be tested for an effect on extending life span in mice.
Increasing health span as well as life span
Steven Austad of the University of Alabama at Birmingham emphasized that increasing longevity is not the same as improving health. Several interventions can extend life span in animals. In some cases, such as the use of rapamycin in mice, health span is also improved. Indeed, rapamycin extends life and delays Alzheimer’s disease, cancer, atherosclerosis, and heart dysfunction in mice. However, genetic mutations that increase life span in the worm Caenorhabditis elegans do not extend the period of good health. Furthermore, life-extending interventions are not without side effects. In mice, dietary restriction and rapamycin have been linked to low bone density, immunosuppression, cataracts, diabetes, and hyperlipidemia.
Life expectancy (gray) and health expectancy (blue) of men and women at age 65. An increase in life span does not always correlate with improved health. (Image: Kennedy BK et al., Cell 159: 709-713 [2014])
Longer human life expectancy with improved treatments for fatal diseases often comes at the cost of declining quality of life and increased disability—Alzheimer’s disease, dementia, frailty, vision loss, pain, joint replacement, and other conditions. Treating the underlying causes of aging may prevent this deterioration in quality of life.
Telomere length as a marker of aging
Elissa Epel of the University of California, San Francisco, discussed the relationship between stress and cell aging. Epel uses telomere length—stretches of repeat DNA at the end of chromosomes—as an indicator of aging. Chronic disease can accelerate telomere attrition; while there are myriad biochemical alterations in each disease, many diseases of aging feature the triad of oxidative stress, inflammation, and hyperglycemia / insulin resistance. For example, in diabetes the disease processes of impaired β-cell function, and resulting higher levels of biochemical stressors, further shorten telomeres.
Psychiatric diseases, particularly major depression and anxiety disorders, are also associated with shortened telomeres. Given the high comorbidity of medical and psychiatric conditions, Epel noted, it is important to consider that depression may affect aging biology, not just the physical disease condition. Treatments for diseases may further affect the rate of telomere attrition, either speeding it up or slowing it down. For example, statins and possibly metformin, used in diabetes treatment, may prevent telomere attrition, while HAART therapy in HIV may accelerate telomere attrition. Chemotherapy can work through telomere damage of cancerous as well as healthy cells. Childhood traumas followed by chronic stressors in adulthood result in shortened telomeres, which correlate with several diseases of aging, including diabetes, cardiovascular disease, stroke, and cancer. Shortened telomeres might be both a cause and a consequence of chronic disease, although this has yet to be fully confirmed.
Disease Drivers of Aging: HIV, Diabetes, and Cancer
Chairs
Ronald Kohanski
National Institutes on Aging and Geroscience Interest Group, NIH
Steven Deeks
AIDS Research Institute; University of California, San Francisco
Claudia Gravekamp
Albert Einstein College of Medicine
Arti Hurria
City of Hope National Medical Center
Jeffrey Halter
University of Michigan
Kevin High
Wake Forest University
Nir Barzilai
Albert Einstein College of Medicine
Highlights
Each person has a unique fingerprint of chronic viral infections—HIV is one example.
HIV treatment normalizes some markers of aging.
Some manifestations of diabetes are relevant to aging, others are not.
Insulin resistance in the brain may accelerate age-related cognitive impairment.
Both cancer and cancer therapies promote cellular senescence and inflammation, which contribute to aging and disease.
Cancer treatment affects areas of the brain that are also changed by aging; these treatments can promote cognitive decline.
Aging with HIV
Despite the success of antiretroviral (ARV) therapy in improving health and increasing life span, people living with HIV are at an increased risk for many age-related diseases, such as cardiovascular disease, cancer, osteoporosis, liver disease, and cognitive impairment. Several panelists stressed the need for a multidimensional approach to investigate HIV and aging, saying that researchers should consider interactions between the seven pillars of aging described during the keynote presentations and focus on possible root causes driving aging.
Although the molecular pathways of aging in people living with HIV are well understood, the field lacks high-quality biomarkers to assess the effectiveness of interventions in clinical trials. The panelists advised aging researchers to make use of the large cohorts established in HIV, particularly MACS, WIHS, and VACS. Researchers have been following both infected and uninfected subjects in these cohorts for up to 30 years, and several types of samples, including serum, DNA, plasma, and urine, are available for study.
Many factors associated with HIV infection and treatment affect pathways involved in aging. (Image courtesy of Steven Deeks)
Gretchen Neigh of Virginia Commonwealth University discussed social stress and HIV. Her work in a rhesus monkey model, used to mimic human infection, showed that previous social stress increased the viral load of simian immunodeficiency virus (SIV) and delayed ARV response. The audience was curious as to whether this effect was attributable to the virus itself or to the illness that SIV causes. This question is difficult to answer in current animal models. Neigh added that the rhesus monkey model could be useful for studying the psychosocial aspects of HIV infection and for studying how social stressors affect viral reservoirs.
Beth Jamieson of the University of California, Los Angeles, showed that ARV therapy can partially normalize DNA methylation patterns, a hallmark of aging. She would like to explore this area further to find out how factors such as duration of infection and early treatment influence this effect. One attendee suggested targeting mitochondrial dysfunction to mitigate the effects of HIV on aging. The panelists pointed to the dearth of studies linking mitochondrial dysfunction to end-organ disease and noted that several older ARVs are mitochondrial toxins, complicating such analyses. Another area of investigation is infection of macrophages by HIV. While most of the panelists focused on infection of T cells, HIV infects macrophages during later stages of disease and could be a source of persistent inflammation.
The effects of type 2 diabetes on aging
It is difficult to establish which complications of type 2 diabetes accelerate age-related effects and which are specific to hyperglycemia, unrelated to aging. For example, patients with diabetes may experience vascular complications, such as neuropathy and nephropathy. However, these effects do not occur with normal aging and are likely a specific consequence of hyperglycemia. However, as Nir Barzilai of the Albert Einstein College of Medicine reminded attendees, researchers are not starting from scratch. Metformin, a common diabetes medication, also prevents several age-related diseases. Understanding this mechanism could be a starting point from which to investigate the effect of diabetes on age-related diseases.
Several audience members asked about the role of insulin resistance in the brain. During his presentation, C. Ronald Kahn of the Joslin Diabetes Center showed that knocking out the insulin receptor in the brain increased measures of anxiety in elderly mice but not in young mice. Kahn’s data also showed the importance of astroglia in insulin signaling. Attendees asked whether there were different families or subsets of astroglia in terms of insulin receptor expression or whether the cells had increased epigenetic variance with age. Kahn replied that he has not seen either effect, but added that he had not specifically looked for them.
One attendee questioned whether a homozygous knockout, which eliminates insulin signaling, is the best model for diabetes, noting that patients with diabetes retain some insulin signaling. Kahn replied that a heterozygous model may better recapitulate the biology of insulin resistance and that it may be worthwhile to use such a model.
There are many pathways and sites through which insulin resistance can affect aging in the brain. (Image courtesy of C. Ronald Kahn)
Another attendee asked about the use of CDK4 inhibitors, which are approved to treat some types of cancer. Jeffrey Halter of the University of Michigan showed that knocking out CDK4 in mice destroys β cells, which are responsible for producing insulin. Halter suggested that oncologists monitor for signs of β-cell dysfunction in patients taking CDK4 inhibitors for cancer. In addition, data from clinical trials of CDK4 inhibitors could be assessed retrospectively to evaluate whether these drugs have negative effects on β-cell function in humans.
One attendee asked the panel about the effects of asthma and decreased oxygen in obese people with diabetes and asthma. While no one on the panel has specifically investigated this relationship, the panelists cited studies in obese diabetics in which sleep apnea was shown to exacerbate insulin resistance. Improving sleep apnea decreased insulin resistance and diabetes.
Diabetes causes a subtle immunodeficiency. In other immunodeficiency models, such as HIV and transplant, cytomegalovirus (CMV) has been shown to play a role in driving vascular disease. One attendee postulated that CMV infection could be a good model to study the interaction between diabetes and aging in terms of vasculature, leukocytes, and endothelial function.
Premature aging caused by cancer and chemotherapy
Jan van Deursen of the Mayo Clinic explained that, in addition to apoptosis, chemotherapy can also induce cellular senescence in tumor cells. The panelists further explained that senescent tumor cells can be cleared by the immune system and that their ability to persist depends on the type of chemotherapy administered.
In patients with cancer, cellular senescence can occur as a consequence of normal aging or as a consequence of disease or treatment-related factors. (Image courtesy of Jan van Deursen)
Timothy Ahles of Memorial Sloan Kettering Cancer Center described how cancer and its treatment result in cognitive decline. One attendee remarked on how brain imaging in normal aging has evolved to not only monitor damage but also to look at compensatory mechanisms that may result from more serious brain damage. Ahles explained that cancer researchers have learned a lot from imaging studies of both normal aging and cognitive impairment because many of the systems affected by normal aging are also affected by cancer treatment. Wendy Demark-Wahnefried of the University of Alabama at Birmingham presented data on accelerated adverse body composition changes that occur as a result of cancer treatment, with chemotherapy inducing gains in fat and losses in muscle in the year following diagnosis that are comparable to 10 years of normal aging.
There are many good mouse models of cancer, but the disease is often studied in young animals, and studies using these models cannot investigate how aging affects cancer. The panelists noted that there has been a push in the research community to use models that develop cancers more slowly, and for researchers using models to induce cancer in older animals. However, achieving these goals can be difficult because it is time consuming and costly to maintain elderly animals. To defray some of these costs, the trans-NIH Geroscience Interest Group (GSIG) put out an RFA, joined by several other Institutes including NCI, to age animal models of disease. Funding for these research projects will be provided jointly by NIA and other relevant NIH institutes. The panelists encouraged researchers to look outside mouse models; a recent review described studies of naturally occurring cancers in pet dogs. The panelists also suggested studying cancer in nonhuman primates.
Several attendees asked about how to mitigate the effects of chemotherapy. Some patients undergo short-term fasting before chemotherapy, which has been shown to promote tumor shrinkage in mice. However, researchers have not studied whether this strategy promotes longevity, similar to the effect of dietary restriction in mice. Similarly, researchers have not systematically studied the effects of antidepressant use before chemotherapy, which has been shown to prevent negative cognitive outcomes of chemotherapy in animal models.
The panelists recommended early interventions, such as exercise during chemotherapy, to prevent or reverse decline in physical function in cancer patients. However, they also noted that later interventions can be effective. In the RENEW trial, an international sample of 641 older, long-term cancer survivors at least 5 years out from diagnosis who received materials and counseling on good dietary and exercise habits had a slower decrease in physical function than those who did not. In another initiative, cancer survivors paired with a gardener had healthier habits, improved function, and improved biomarkers of aging after one year of gardening.
The Way Forward
Moderator
Felipe Sierra
National Institute on Aging, NIH
Highlights
There is a need for a uniform definition of accelerated aging and standardized biomarkers to monitor aging.
Researchers should identify and focus on the root causes that drive aging instead of downstream effects.
Funding agencies should ensure that suitable aging-related experiments are included in grant proposals.
A call for uniformity
The meeting ended with a panel discussion on common themes and open research questions to advance therapies for chronic diseases and aging. Several attendees mentioned the need for a uniform definition of accelerated aging. There are many ways to define aging, ranging from molecular and cellular processes to functional ability and population age. In many animal models of aging, life span is the primary outcome for aging. However, this outcome would not be informative for clinicians; it does not reveal whether a patient is experiencing accelerated or normal aging or whether a treatment is improving the effects of aging. One attendee suggested creating an NIH toolbox of biological markers of aging to provide a common vocabulary for researchers. Currently, the best biomarkers of aging are composite measures that usually include function. The panelists recommended that studies measuring aging should include data representing at least two pillars of aging, such as DNA methylation and resistance to a stressor.
Several attendees also suggested that the research community create a single database, such as those housed at WikiPathways, to organize the biological pathways involved in aging and disease. Websites that currently house this information for aging do not include information on the relationships between aging and disease.
The big picture
Several panelists noted the importance of interactions between the seven pillars of aging. However, they cautioned against focusing on any single pillar and advised that the pillars be used as a guide and not as rigid categories for aging research. It is nonetheless clear that cellular senescence and inflammation are among the most important features of aging common to the three diseases discussed at this meeting. Cellular senescence has many forms, and targeting one form may not prevent others. Several attendees pointed out that therapeutic targeting of any one marker of inflammation or cellular senescence may not remedy their underlying cause(s) and their subsequent effects on aging and disease.
Funding and resources
The panelists also noted the need for more aging studies in general. One reason that investigators are hesitant to study aging is the time and expense of using aged animal models. While some larger centers, such as the Pepper Institute at Florida State University and the Shock Center at the University of Washington, have the infrastructure to do so, smaller institutions do not. Audience members recommended that the facilities at these centers be made available to researchers, particularly junior faculty, to help recruit more people to the aging field. The panelists also noted that datasets of relevance to aging are available on the NIA website.
Another reason for the lack of aging studies is the difficulty of acquiring funding for long-term, complex studies. The panelists remarked that grant reviewers sometimes ask that aging-related experiments be removed from proposals. Instead, aging experts on review committees should ensure that such complexity is included in proposals and confirm that an appropriate model system is being used so that studies on diseases that affect the elderly are not conducted in young mice. One audience member suggested supplements to existing grants be made available to fund extra samples for aging research. For example, ancillary studies could make use of specimens collected in clinical trials to analyze predictors of aging.
Open Questions
General
How can we best bring together those who study disease and those who study aging?
How should clinicians define aging and accelerated aging?
What biomarkers can be used to evaluate accelerated aging in the presence of chronic diseases and to assess the effects of interventions?
What are the best animal models to study accelerated aging in the presence of chronic disease?
Are life-extending therapies that work in animal models relevant to humans, and will they also extend health?
How can funding agencies, such as the NIA, encourage investigators to consider the effects of aging in their model systems?
Effects of HIV on aging
What is the role of senescent T cells in age-related diseases?
What can epigenetic changes in T cells tell us about the link between these cells and diseases of aging?
How does psychosocial stress affect HIV pathogenesis and response to treatment in humans?
What information can be gleaned from established HIV cohorts with respect to HIV and aging?
Future research questions for HIV and aging
How do disease factors, such as duration of infection and time of treatment, influence the effects of ARV therapy on markers of aging?
What can primate models of HIV infection tell us about psychosocial aspects of disease and how social stressors affect disease reservoirs?
What role might mitochondrial dysfunction play in HIV’s effect on aging?
How does infection of macrophages contribute to inflammation?
Effects of diabetes on aging
How do some diabetes therapies (eg, metformin and acarbose) increase longevity?
Which complications of diabetes are relevant to aging, and which are specific to increased blood glucose?
Could insulin resistance be a protective mechanism against accelerated aging?
Future research questions for diabetes and aging
How do CDK4 inhibitors affect β-cell function?
How do conditions that decrease the supply of oxygen, such as asthma and sleep apnea, influence insulin resistance?
What role might the immunodeficiency caused by diabetes play in driving vascular dysfunction?
Effects of cancer on aging
What are the different signs of, effects of, and treatments for cancer-related and chemotherapy-related senescence?
How can we definitively show that inflammation and coagulation affect function and survival?
Future research questions for cancer and aging
Can lifestyle changes improve cognitive function in older cancer patients?
How might short-term fasting prior to chemotherapy affect aging?
Can taking antidepressants before initiating chemotherapy mitigate cognitive decline?

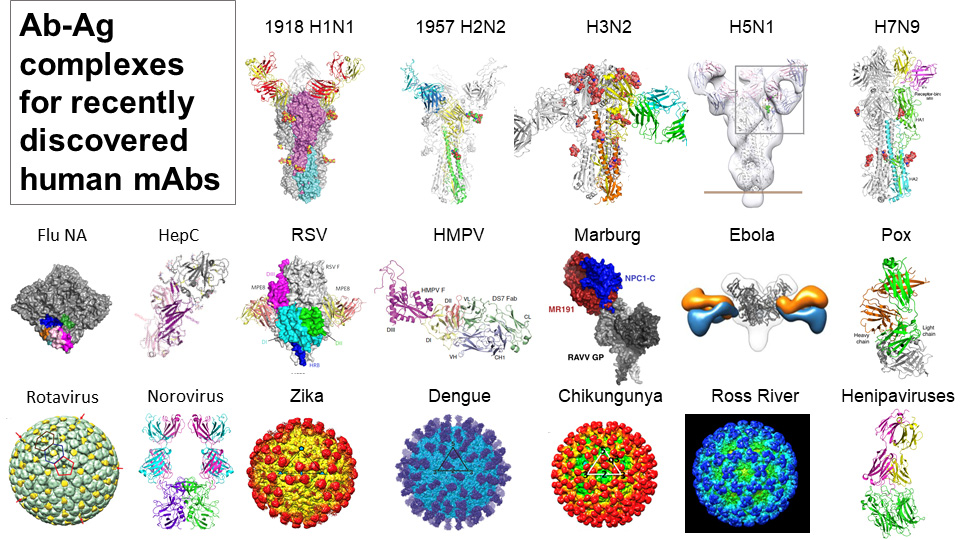
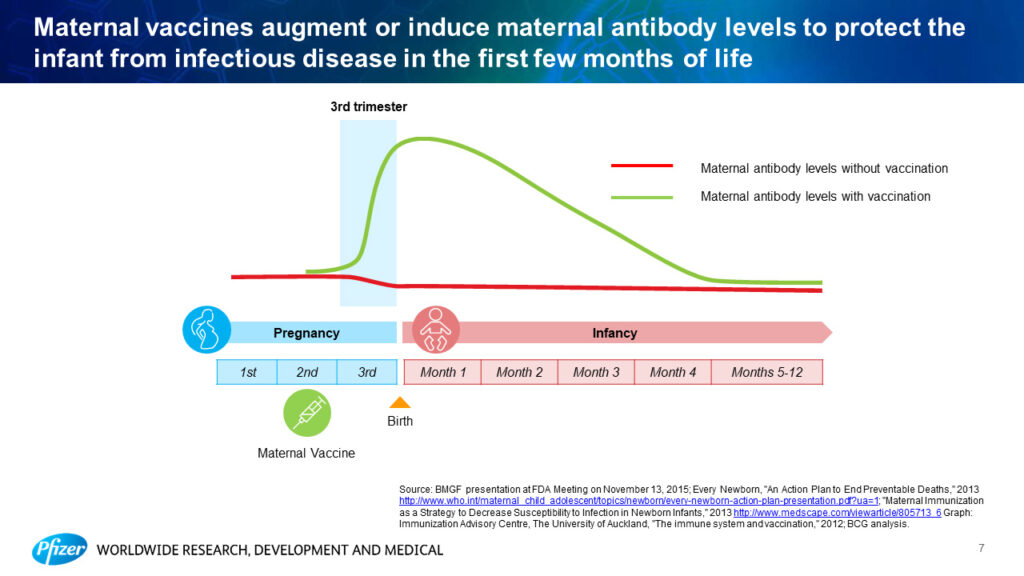
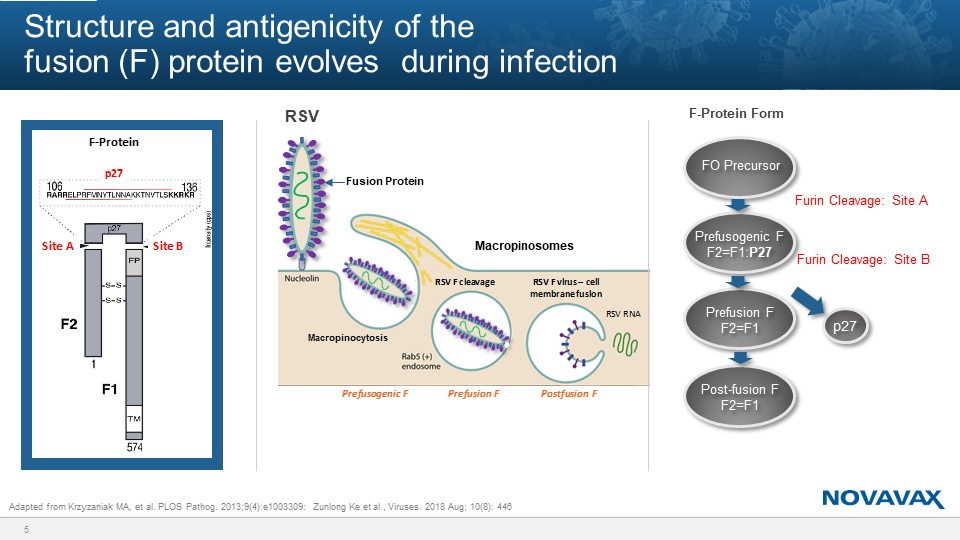

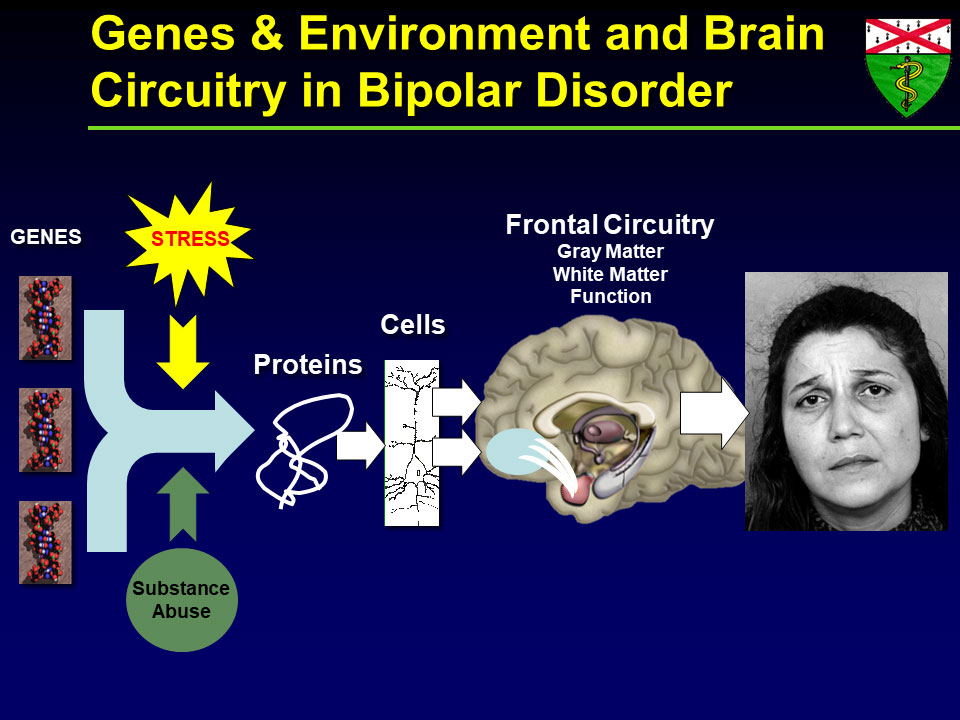
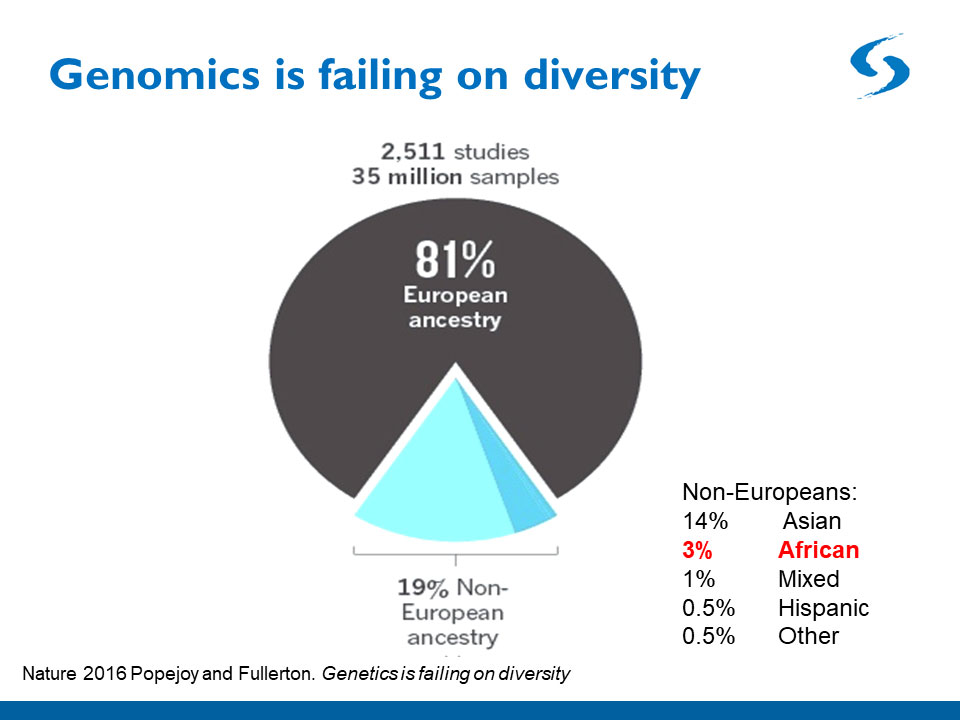

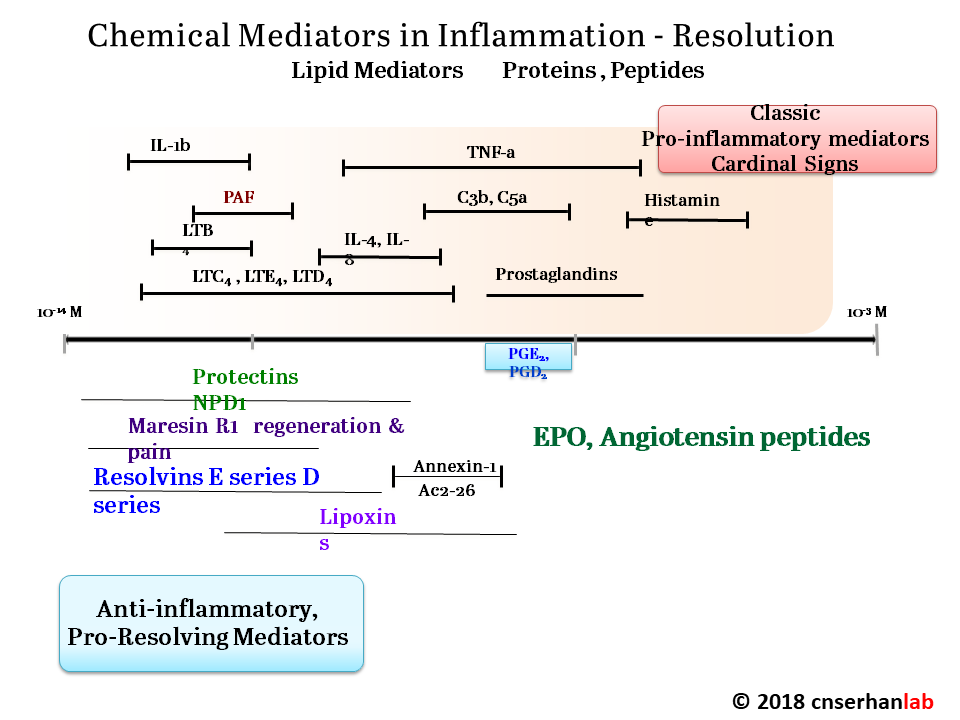
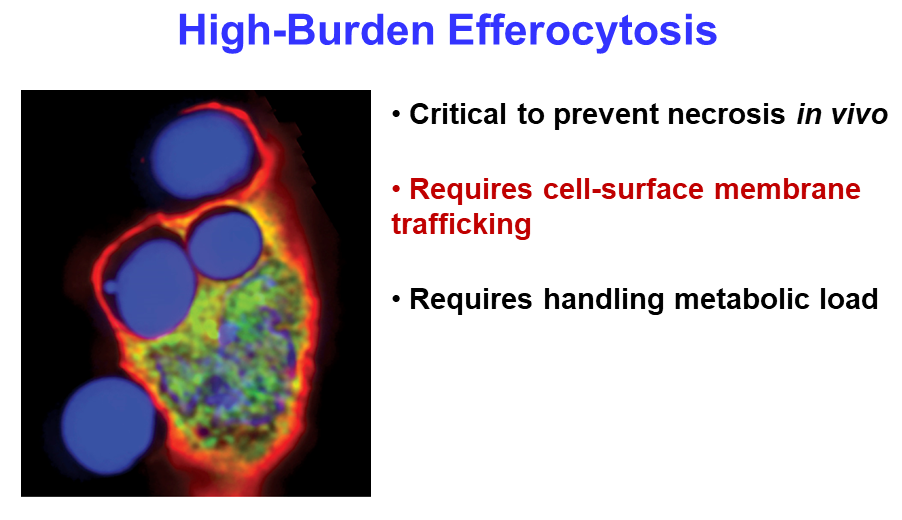
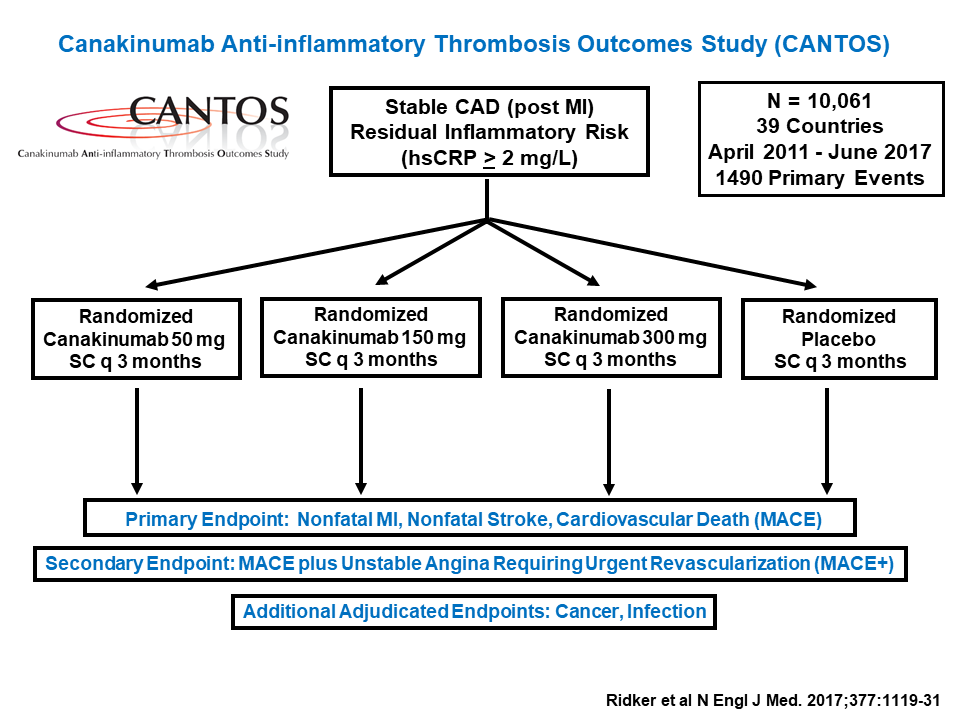
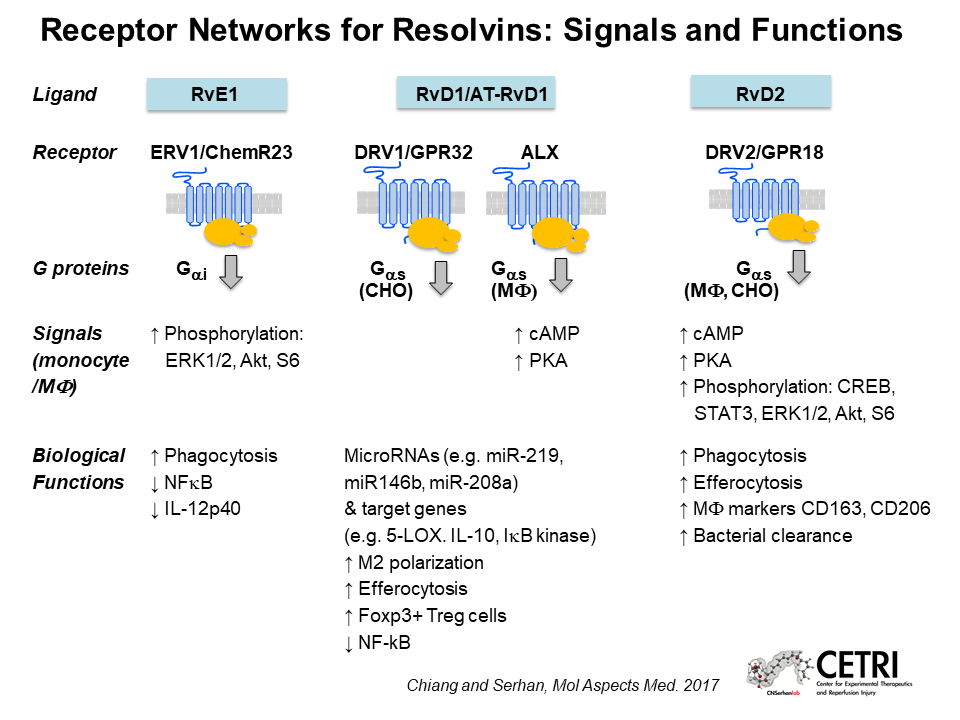
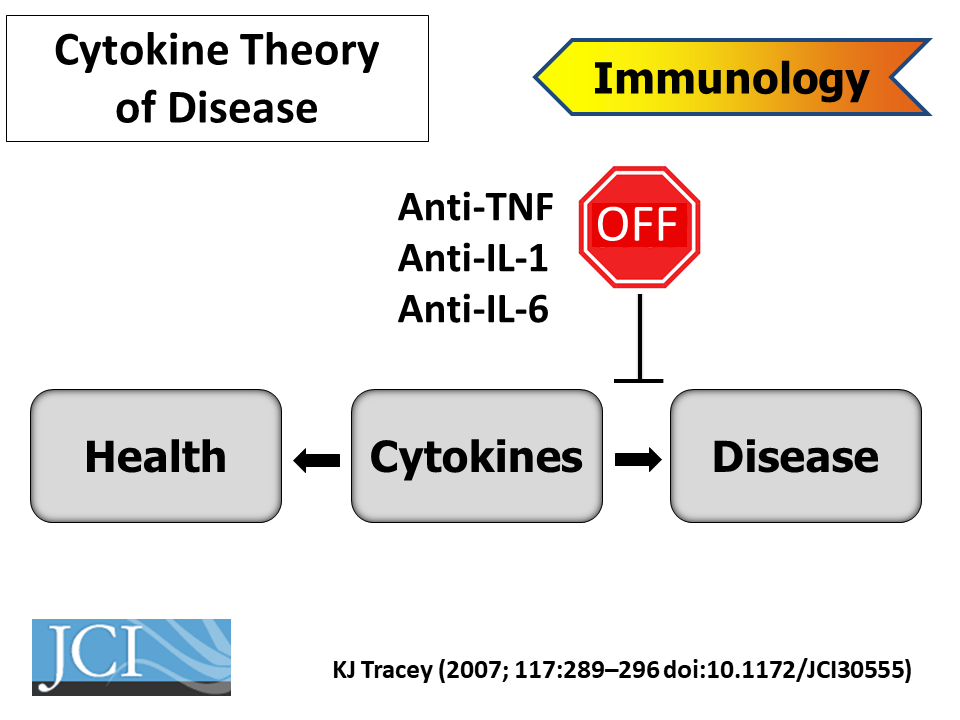
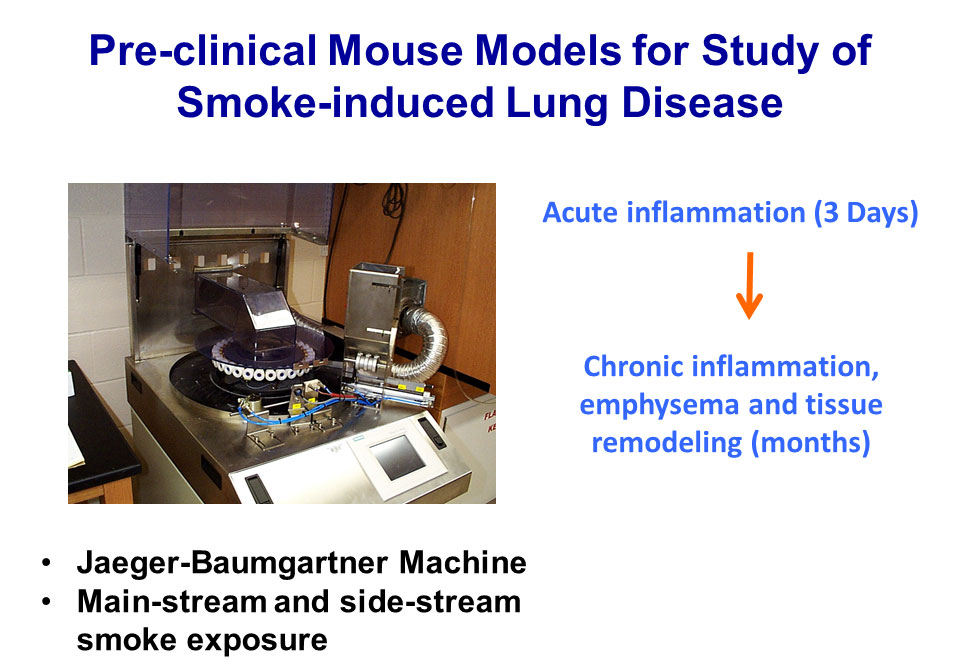
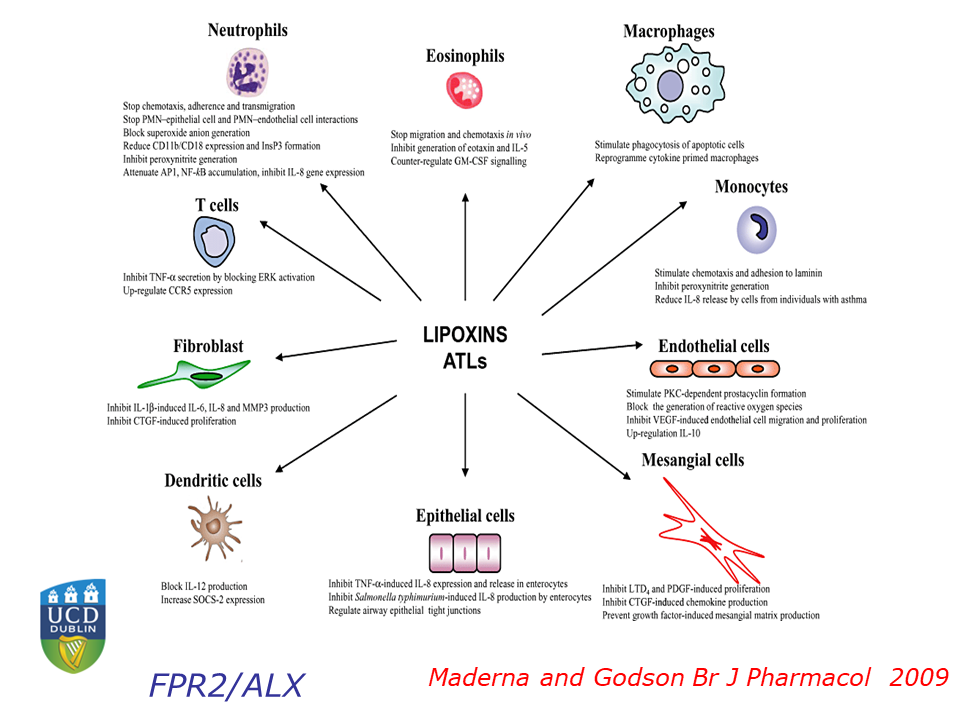
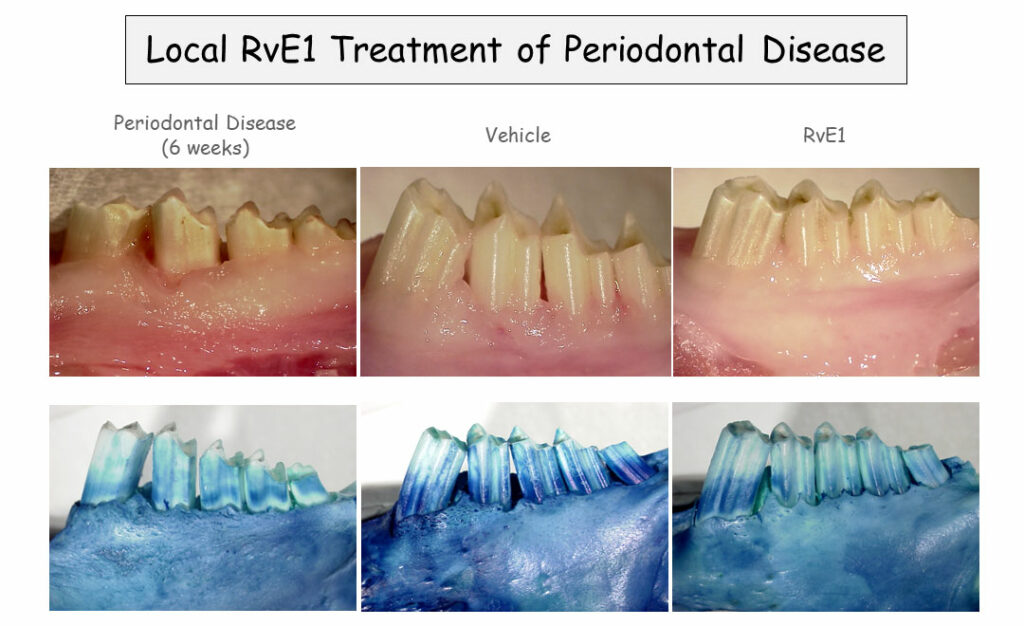
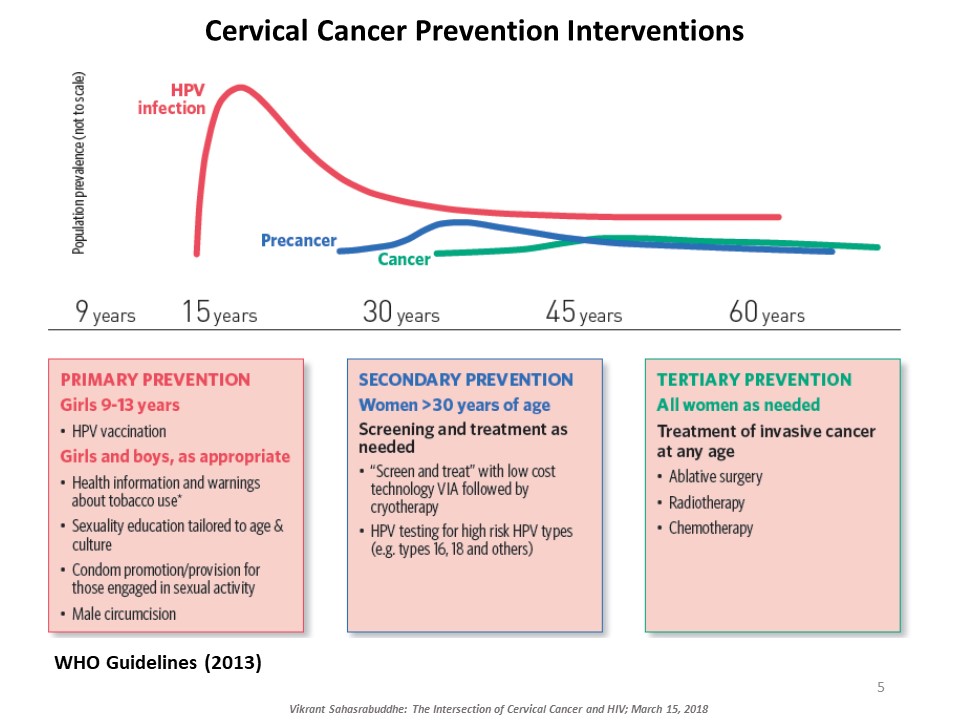
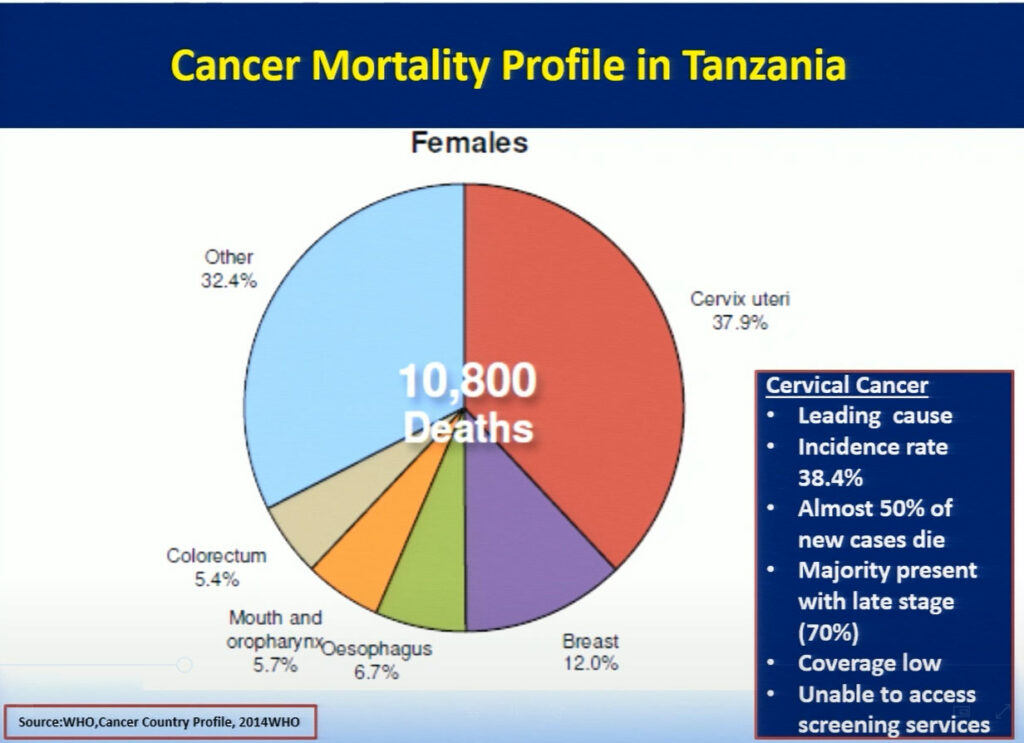
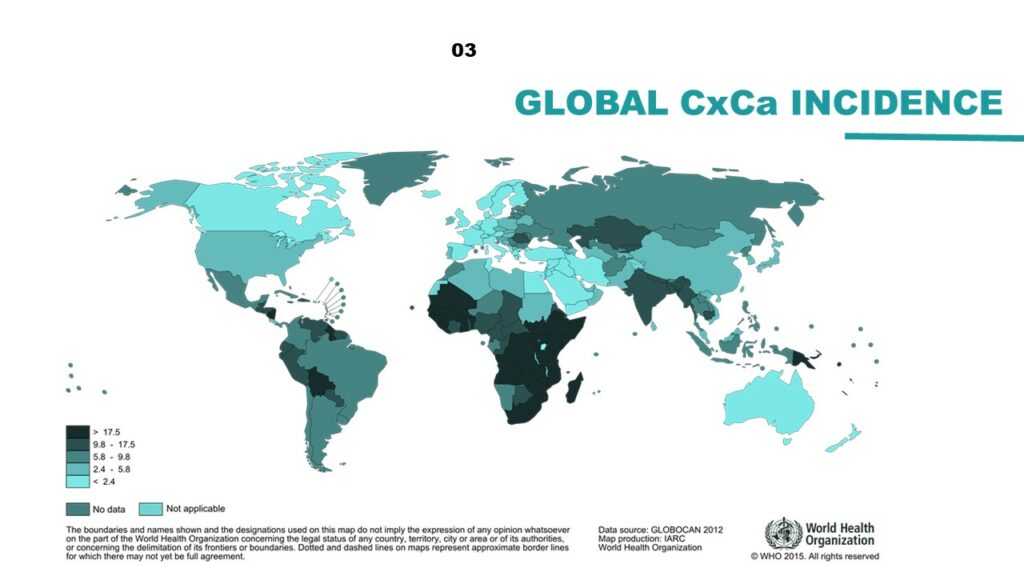
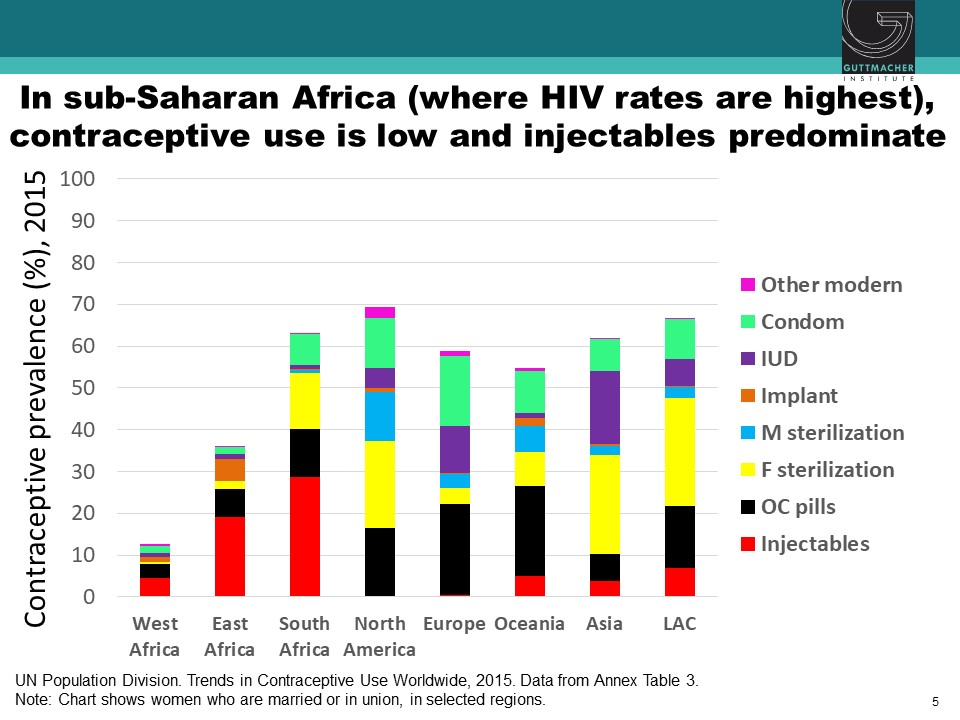
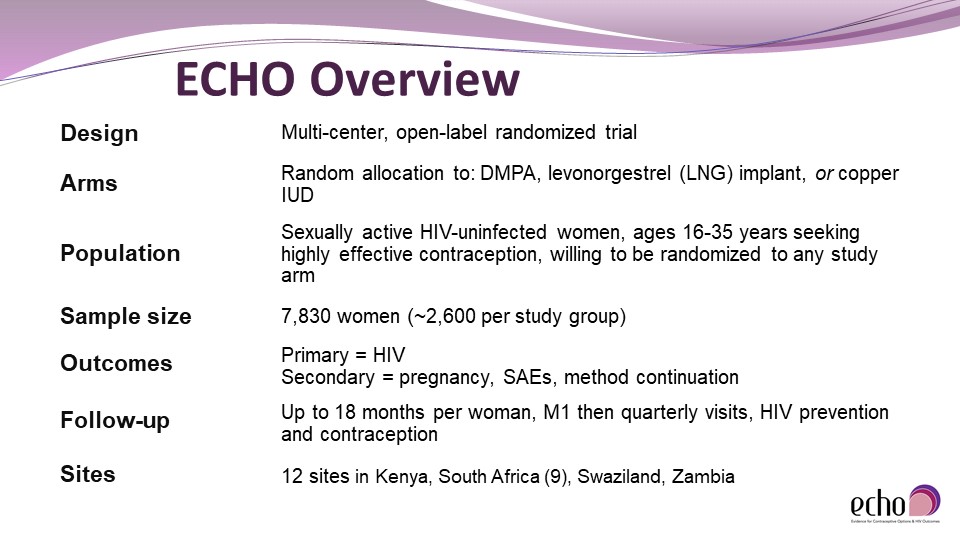
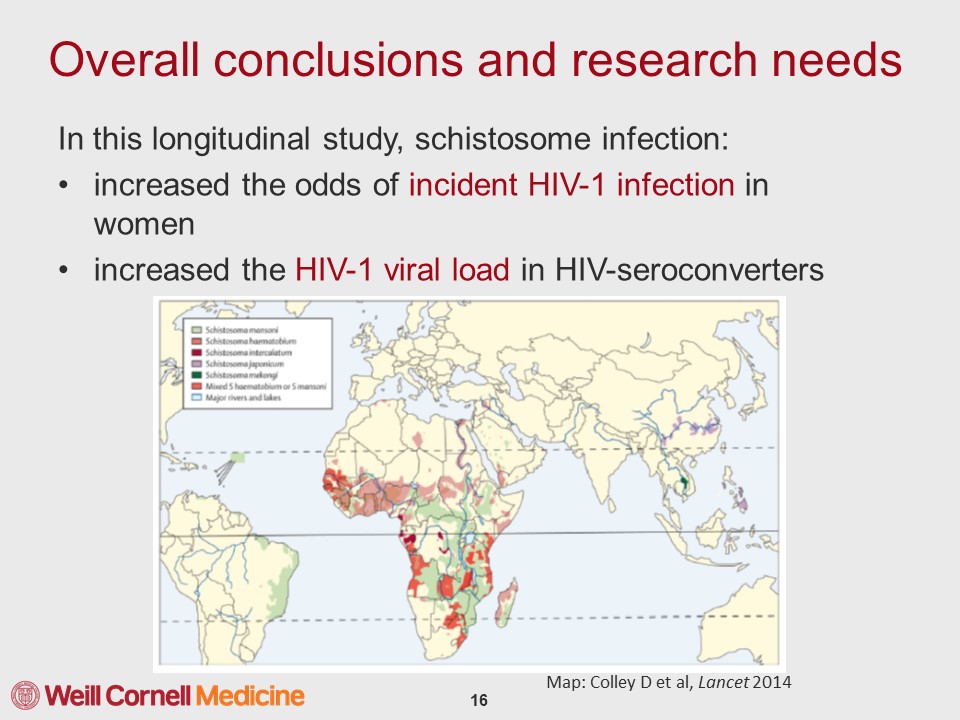
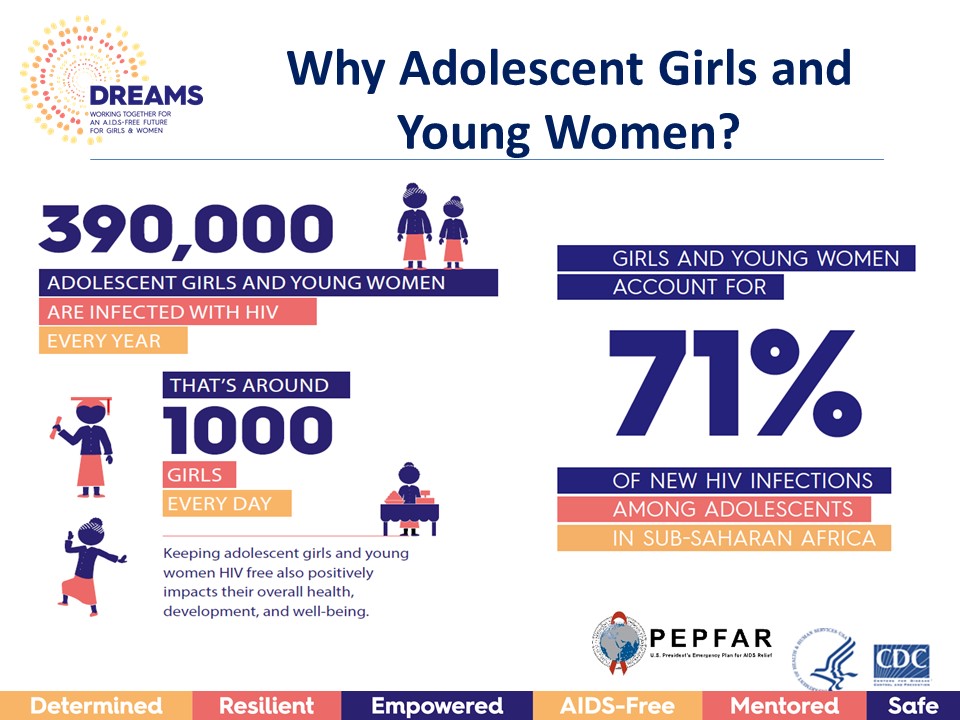



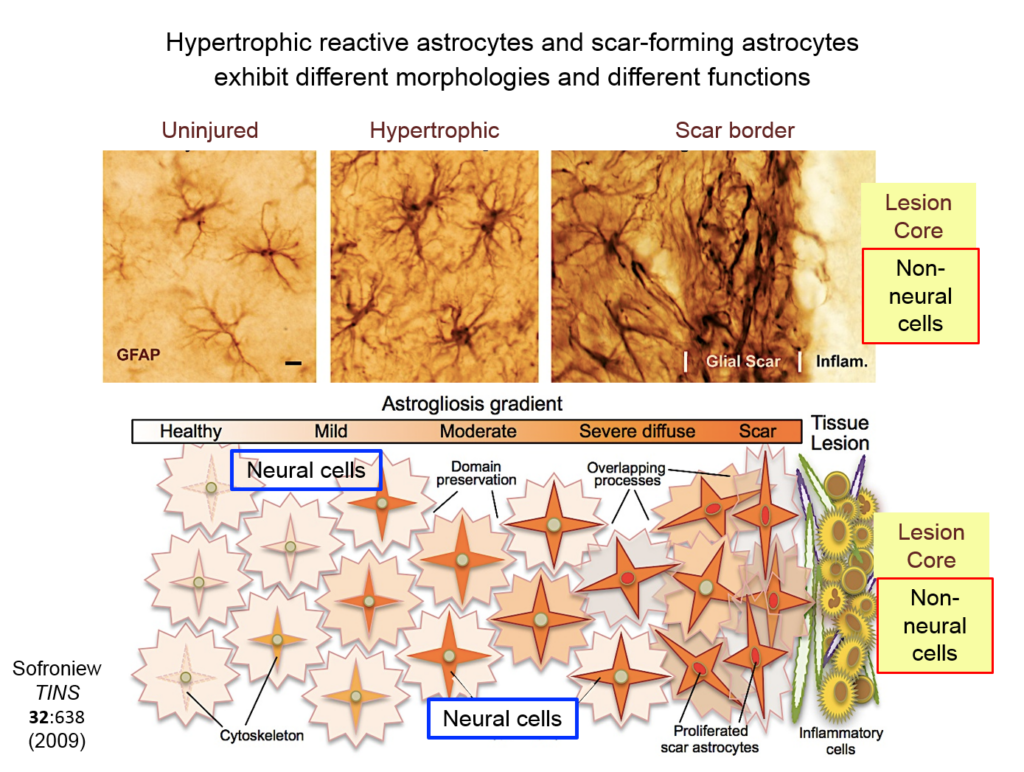
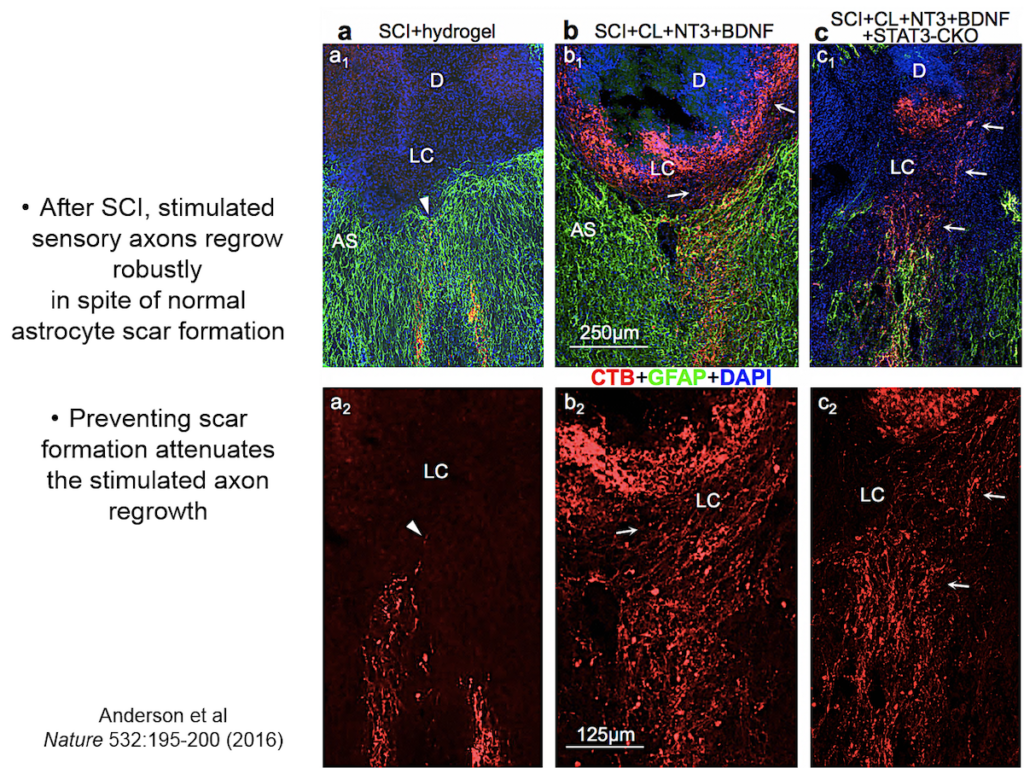
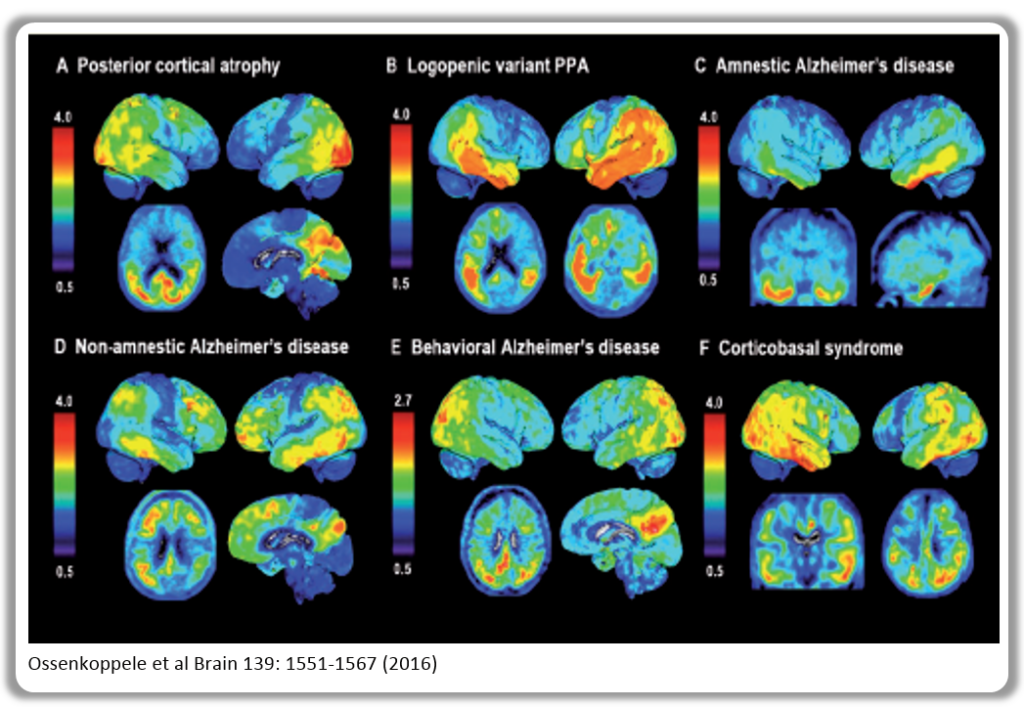
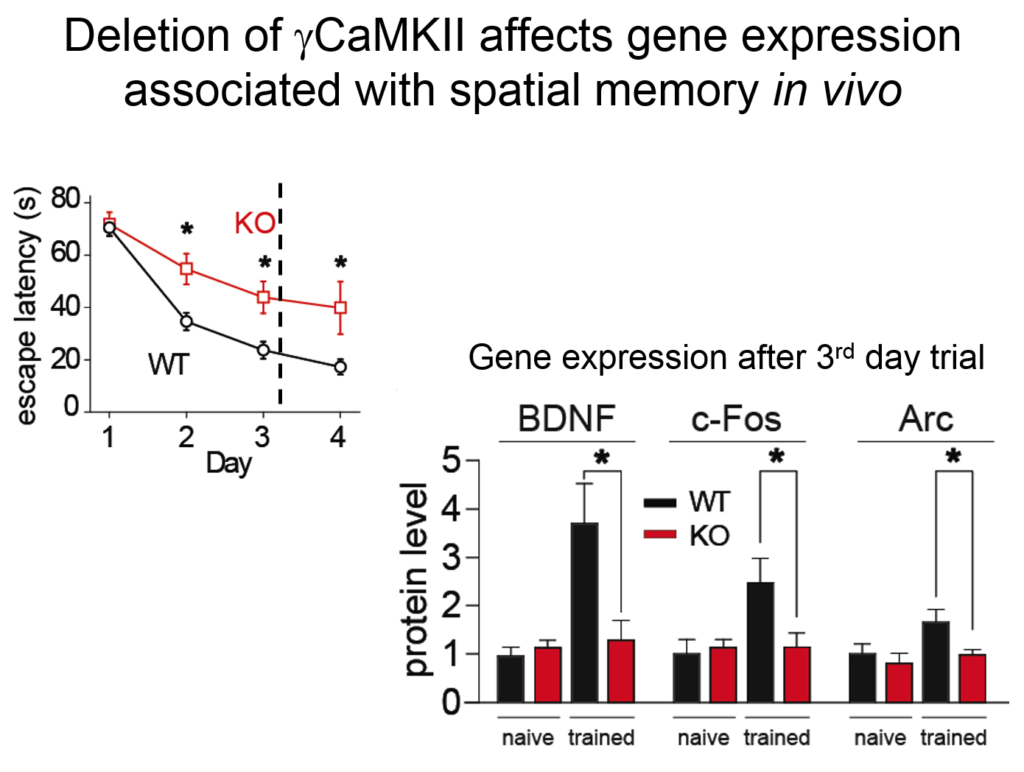
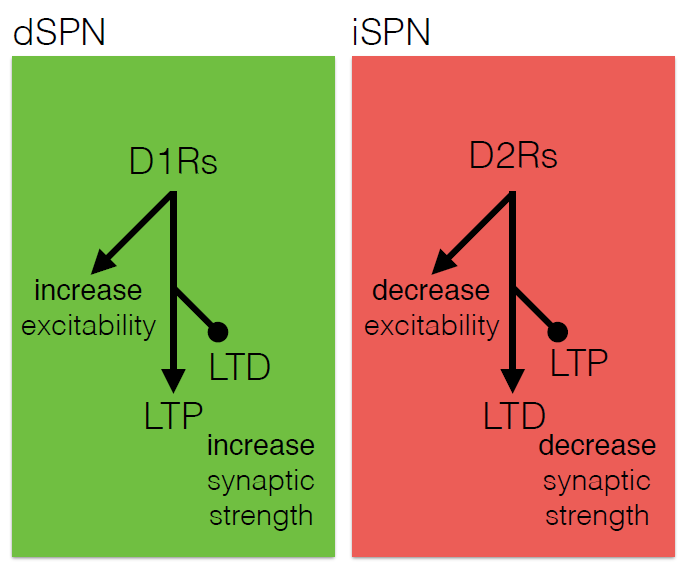
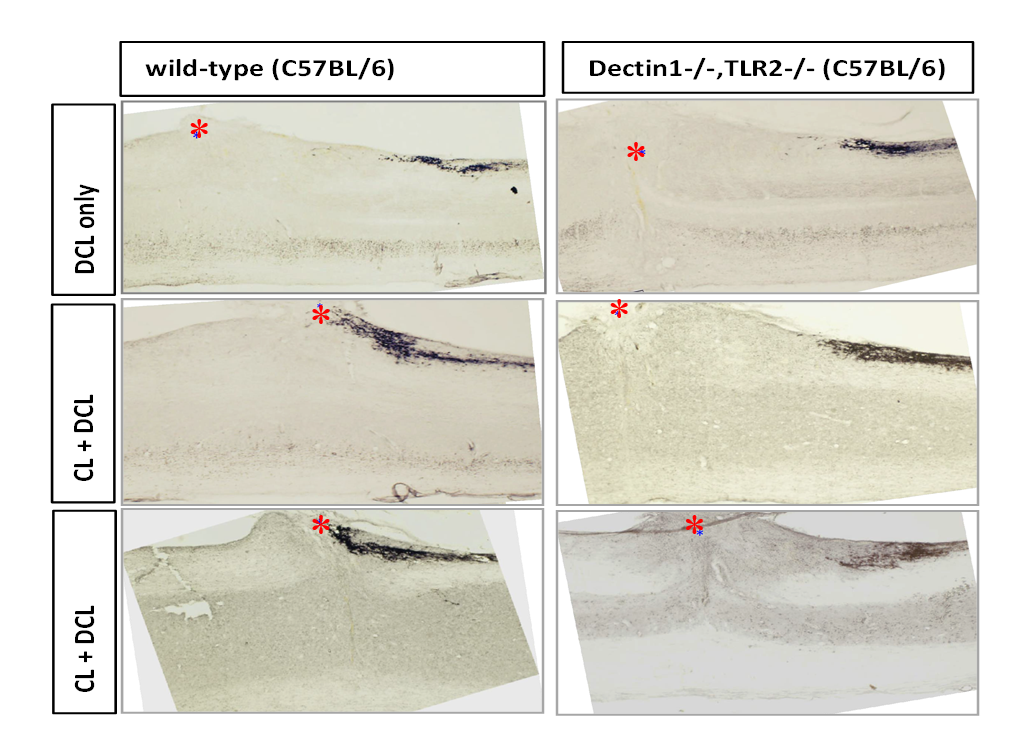
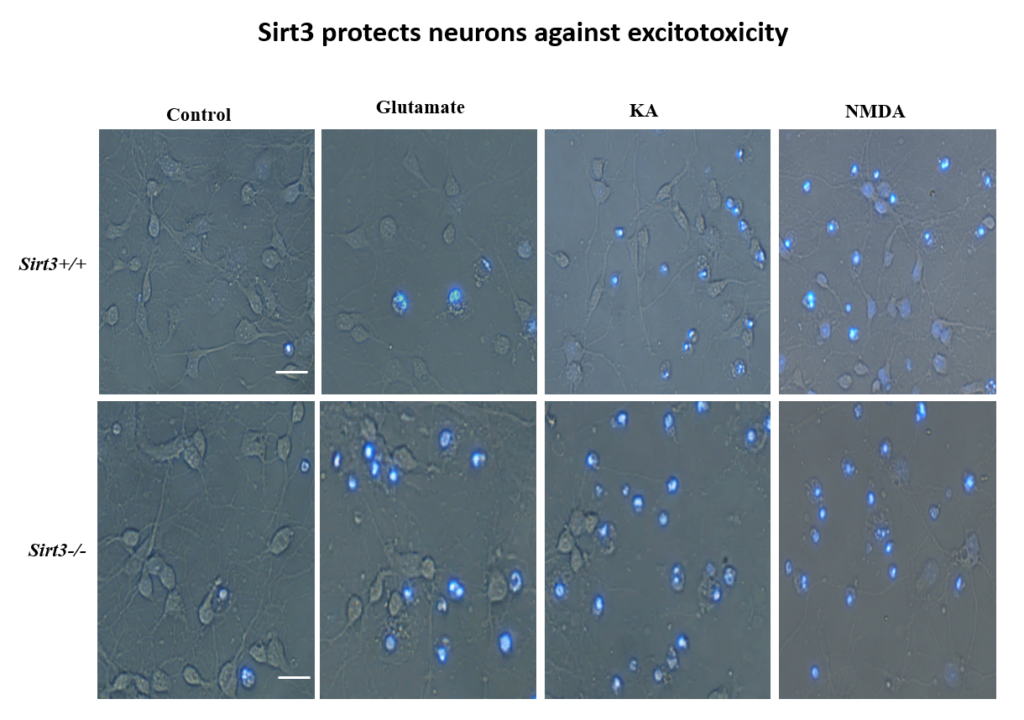
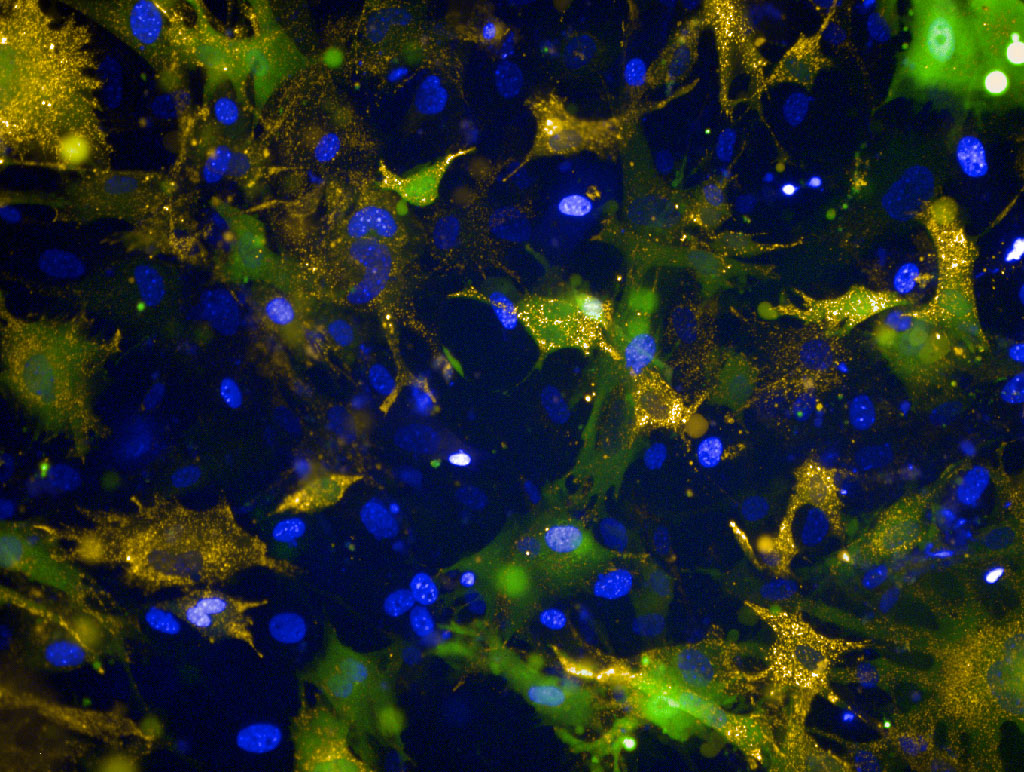
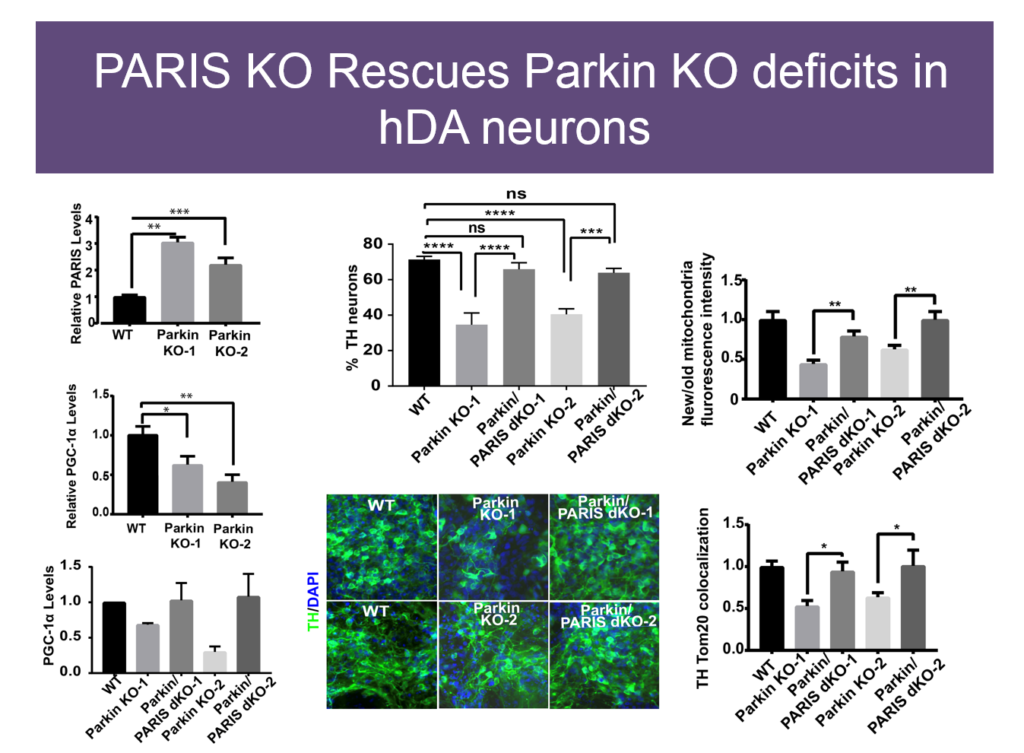
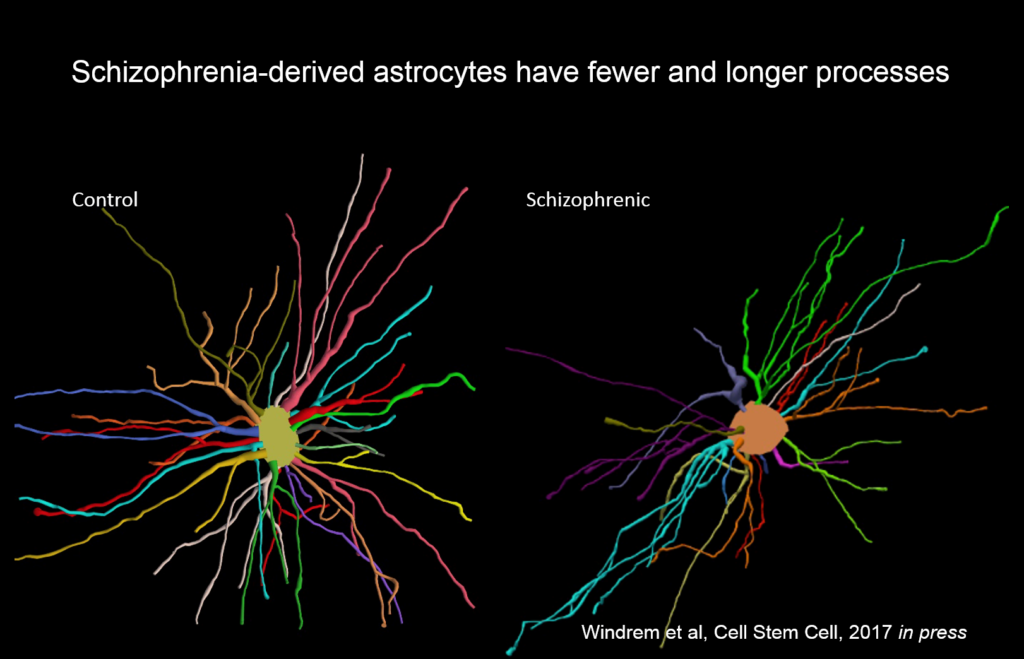
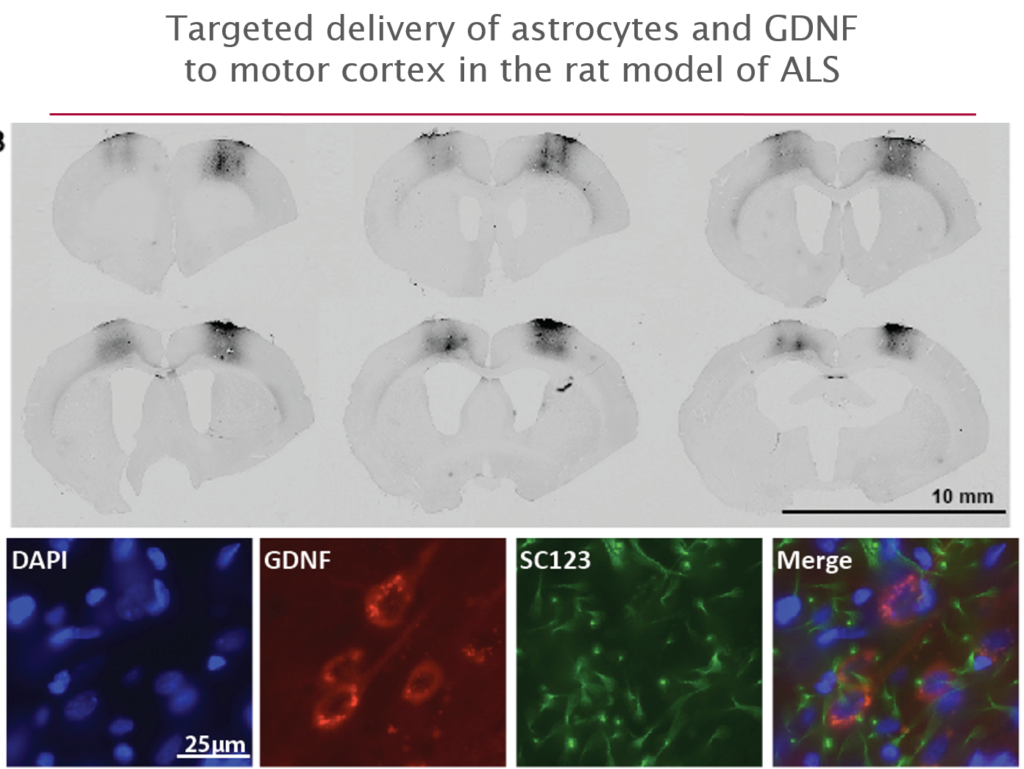
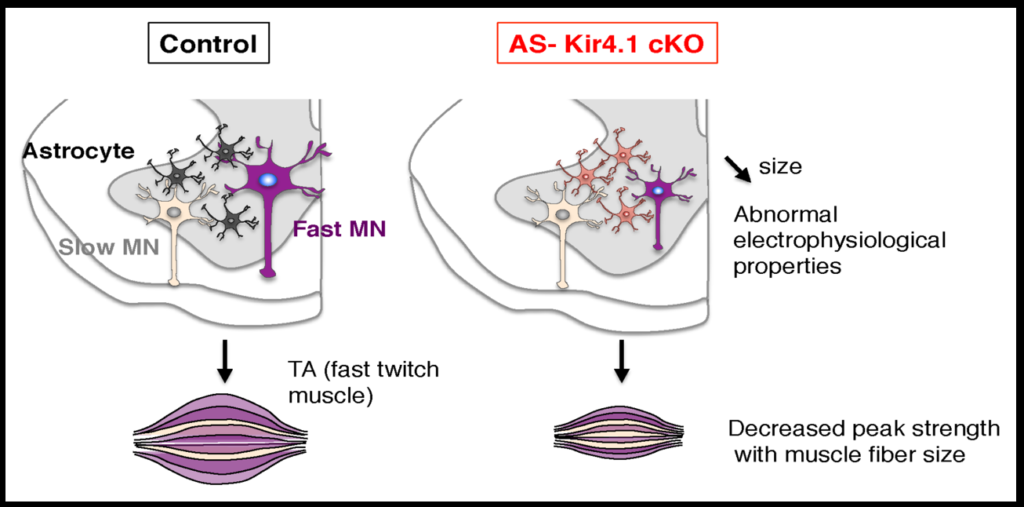
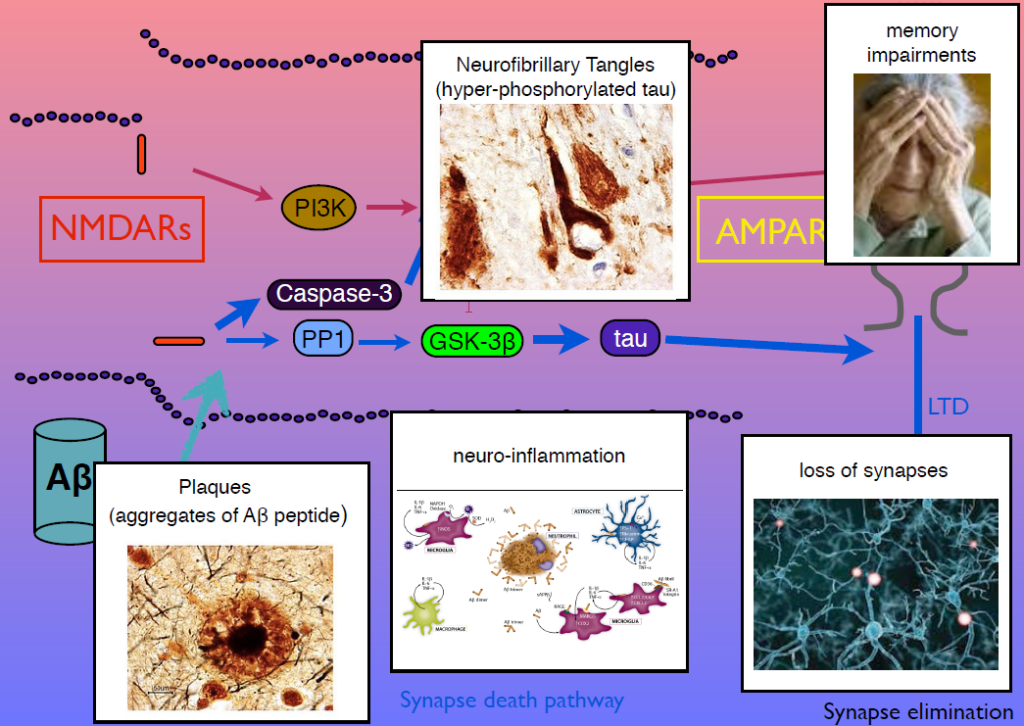
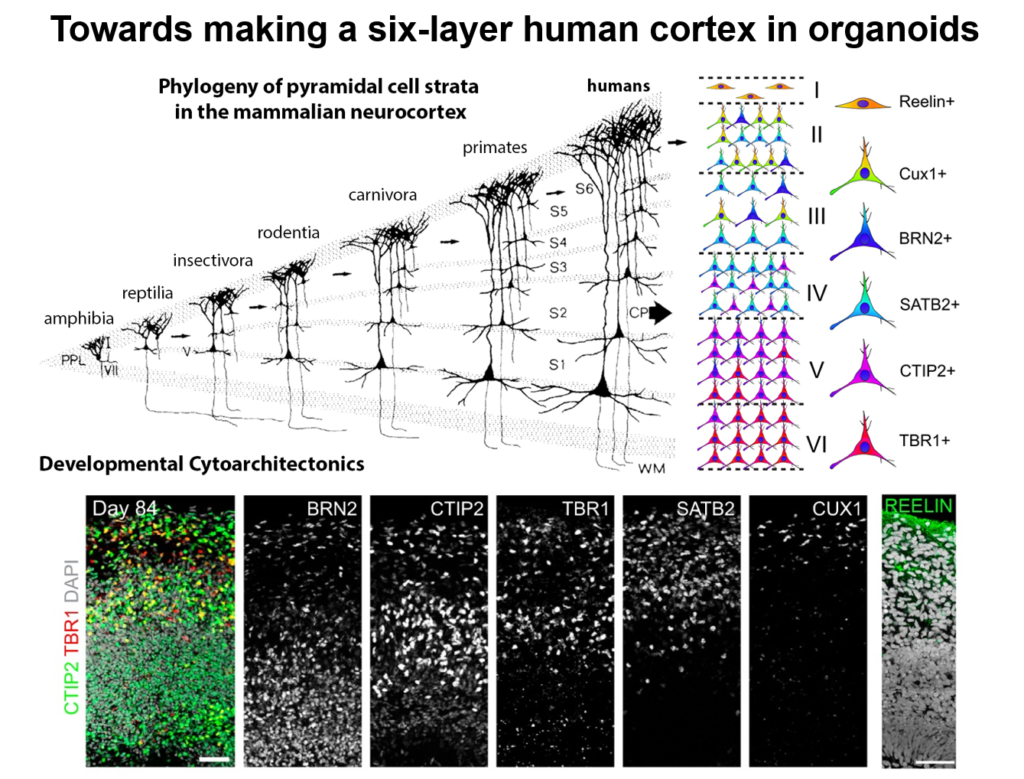
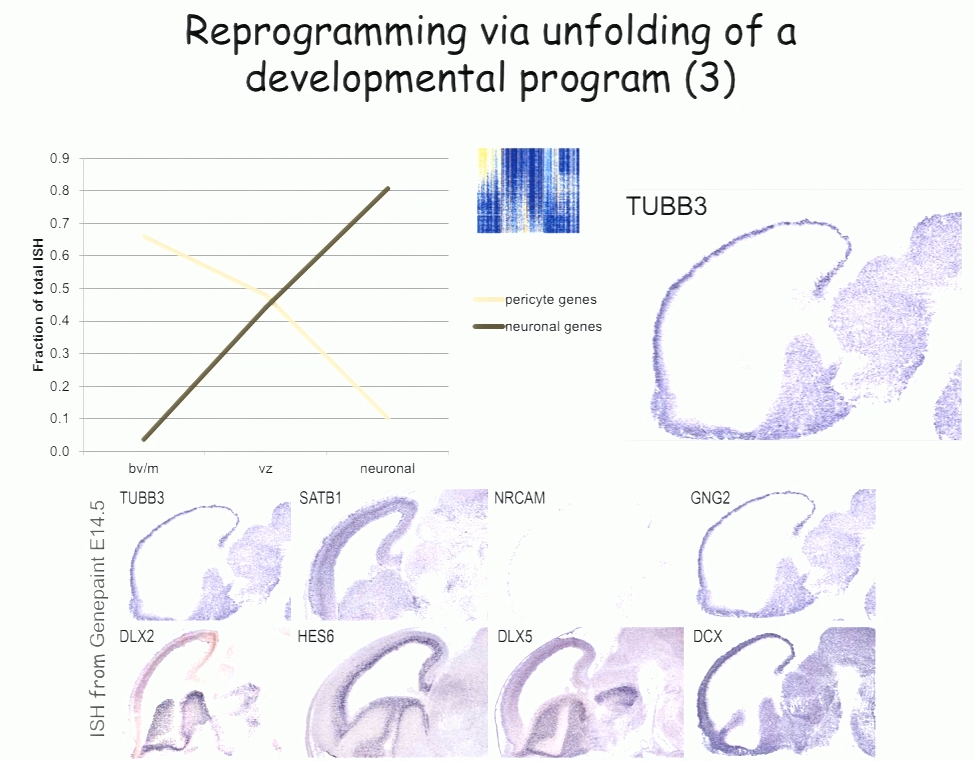
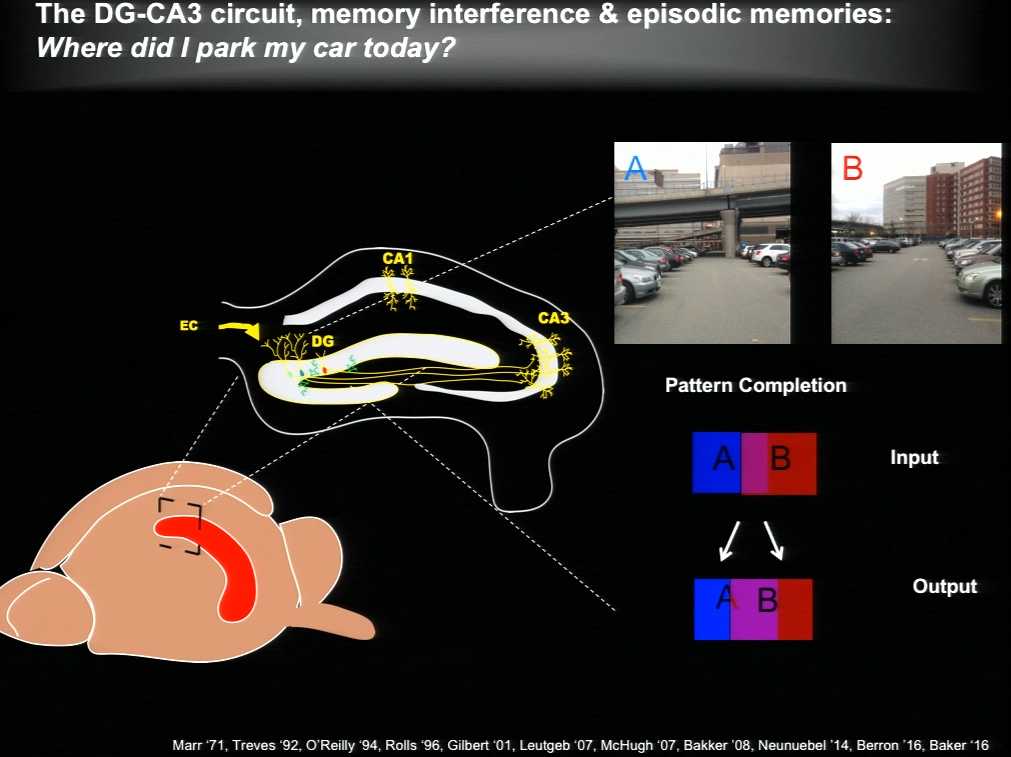
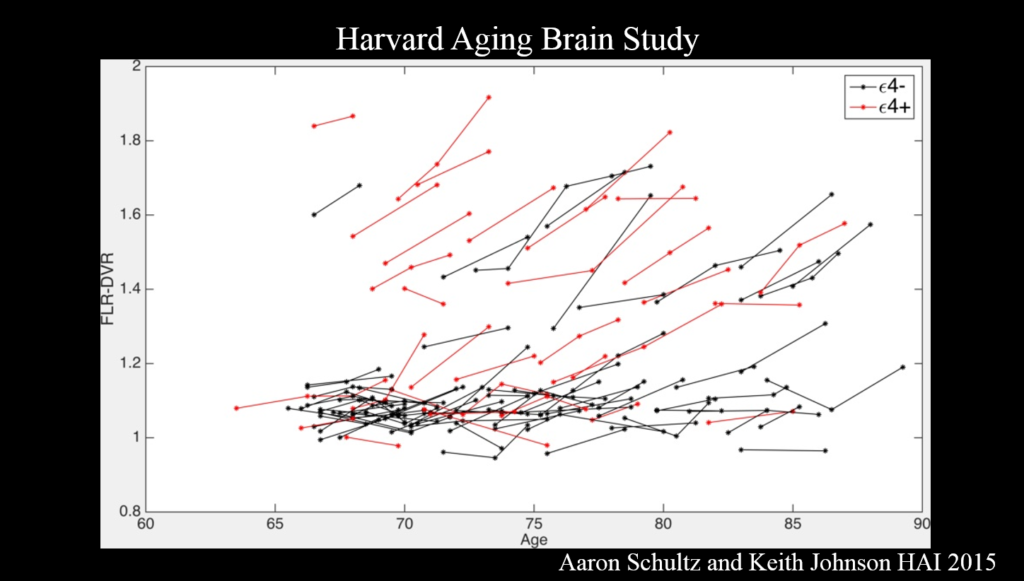
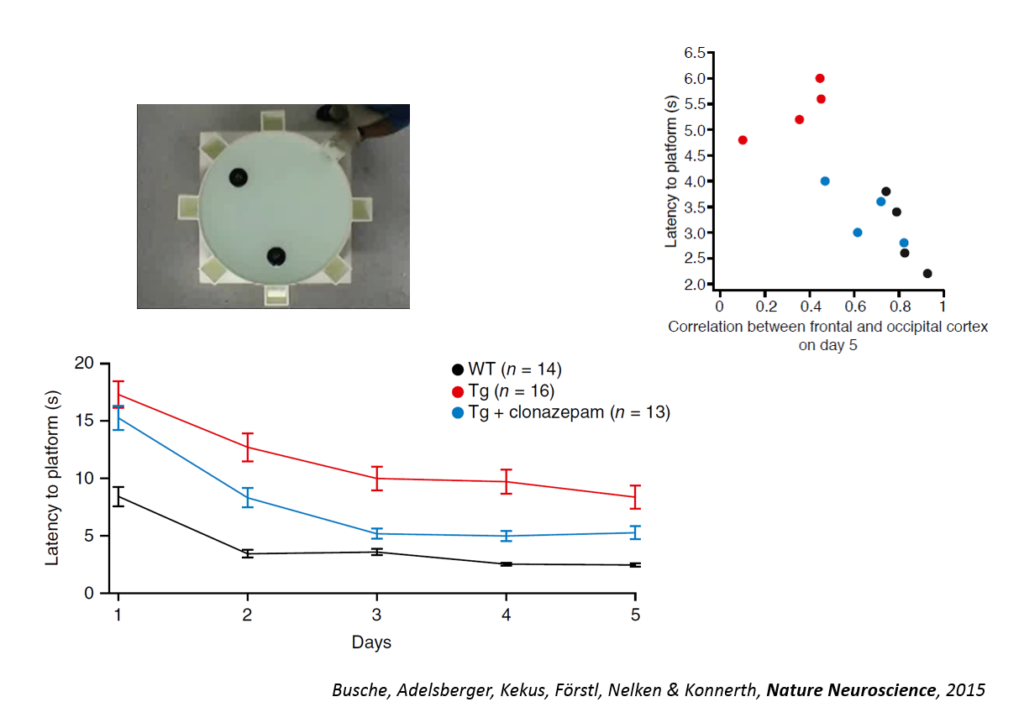
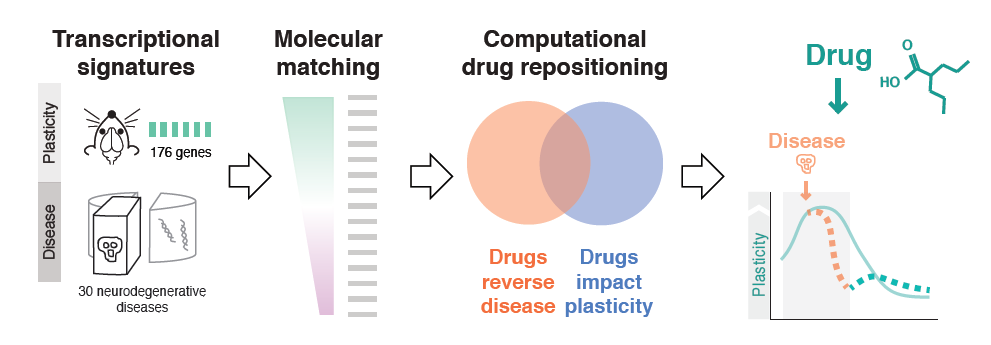

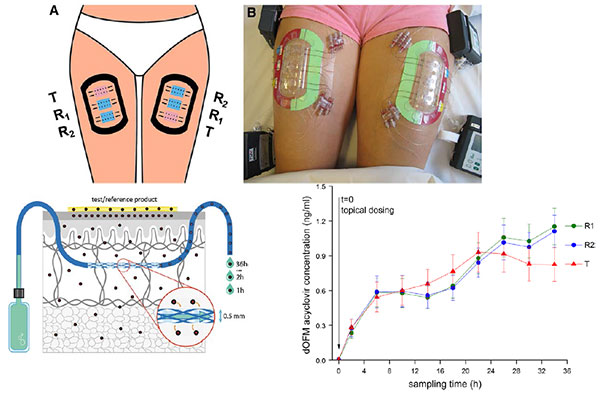
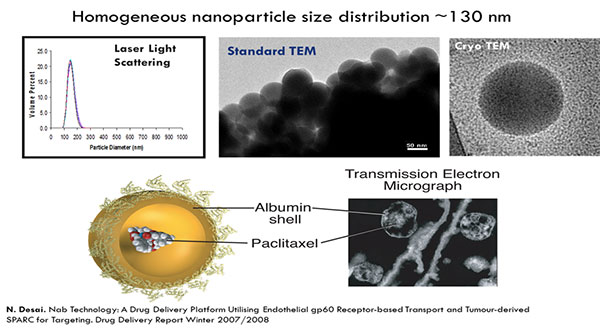



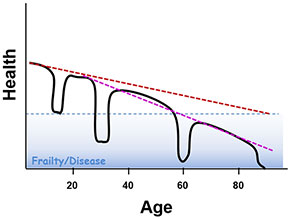
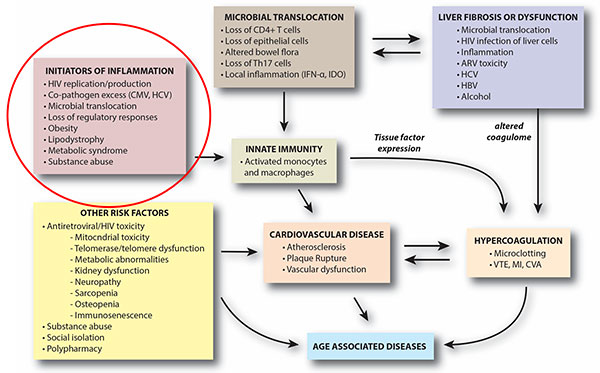

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}